
Abstract
Background and objectives
Chronic obstructive pulmonary disease (COPD) is one of the most debilitating somatic diseases, having anxiety and depression frequently as comorbidities. The coping style, the way in which the subject manages to control the difficult and stressful situations of life, can influence its evolution and also the existence of the comorbidities. In this study, coping styles in a group of subjects with COPD and their association with the intensity of depressive and anxiety symptoms as well as medical determinants were identified.
Materials and methods
In this cross-sectional study, 28 male patients with COPD risk class D were enrolled. The patients performed spirometry tests, Borg scale, 6-minute walking test, Hospital Anxiety and Depression Scale, and COPE Inventory were recorded.
Results
According to their higher coping subscale score, the depression score was the highest in patients with avoidance-type coping and the lowest in patients with problem-focused coping (11.0 vs 5.6; P=0.042), respectively, patients with social support-focused coping having the highest anxiety score in contrast to patients with emotion-focused coping, which had the lowest anxiety score (11.6 vs 5.0; P=0.006). Regarding respiratory parameters, significant differences were present for the variation of the medians between the four groups only for forced vital capacity (FVC%) (the lowest FVC% was in patients with predominant social support-focused coping and the highest in patients with problem-focused coping) and 6-minute walking test (%) (the lowest score for patients with social support-focused coping and the highest value in patients with avoidance-type coping). Problem-coping score was significantly and positively associated with FVC% (Spearman’s r=0.400; P=0.035), emotion-focused coping score was significantly and positively associated with FVC% (Spearman’s r=0.395; P=0.038), and social support-focused coping score was negatively and significantly correlated with forced expiratory volume in 1 second/FVC% ratio (Spearman’s r=0.389; P=0.041). A significant, negative correlation was found only between depression score and forced expiratory volume in 1 second (Spearman’s r=−0.435; P=0.026) with respect to psychiatric symptoms.
Conclusion
Coping styles in patients with COPD affect the intensity of associated depressive and anxiety symptoms as well as medical determinants, thus the coping style should be considered an important part in the multidisciplinary approach of these patients.
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the most prevalent and debilitating disease in adults all over the world. It is a progressive airway disease associated with psychological distress.Citation1 Therefore, two of the most frequent comorbidities of COPD are depression and anxiety; some studies mention the presence of depressive and anxious symptoms in over 70% of cases.Citation2–Citation8 Failure in identifying and treating the depressive and anxious symptoms in patients with COPD has a negative impact on the quality of life and medical outcomes, contributing to a substantial burden of COPD-related morbidity.Citation9,Citation10
A recent meta-analysis of 25 studies on subjects with COPD, that was designed to find a connection between depression and this disease, considers this relation to be bidirectional: depression can be both a cause and a consequence of COPD.Citation11 The mechanism that determines the frequent association of COPD with depression and anxiety has not been identified yet; therefore, further studies in this direction are necessary. The existence of at least three comorbidities in patients with COPD (eg, myocardial infarction, lung cancer, depression, anxiety, and hip fracture) results in an increased frequency of their hospitalization, and also in their premature mortality.Citation12,Citation13
A greater amount of information sustains the impact of psychological stress on the somatic level, such as pulmonary function, exercise capacity, and pulmonary-specific symptoms of COPD.Citation14–Citation17
Therefore, the way in which a subject manages this stress (the style of coping used) might become an important factor in the progression of the illness, as well as in its successful treatment and rehabilitation. Teaching adequate coping strategies should be considered for a better control of the disease.
Coping represents a psychological process developed at a conscious level that we use when we try to manage the difficult and stressful situations of life. The coping style can be both adaptive, implying the stress reduction, and maladaptive, situation in which the maintenance and the amplification of the current symptomatology are present or can determine the appearance of some new symptomatic elements and behaviors. It can also influence the person’s reaction at a biological level leading to a normal or pathological reaction of the human subject, depending on its efficiency in reducing the psychological distress.Citation18
Therefore, it is important to identify the impact of coping style both on the maintenance or in the reduction of anxiety or depression symptoms and also on respiratory parameters and exercise tolerance in COPD. After identifying the type of association between the coping styles used by COPD patients and the aforementioned aspects, we can hope to improve the psychotherapeutic intervention as well as the recovery and prevention of exacerbation in terms of time and costs.
The aim of this study was to identify the coping styles of a group of people suffering from COPD and the association of this group with the depressive and anxious symptomatology and with the medical determinants.
Materials and methods
This study included 28 male patients with COPD risk class D (patients who present more than two exacerbation per year, having a modified Medical Research Council score >2, and a COPD Assessment Test score >10, being spirometric classified in class Global Initiative for Chronic Obstructive Lung Disease [GOLD] 3–4; FEV1 <50% predicted) who came to a control visit and who met the GOLD criteria ().Citation19 Prior to participation in the study, all patients signed an informed consent form. The consent forms and the study were approved by the Psychiatric Clinic “Eduard Pamfil”.
Table 1 Patients’ demographic data
Inclusion criteria: male patients >60 years, former smoker >10 packs/year, COPD GOLD class D without exacerbation of respiratory symptoms in the last 2 months, and no mental illness or use of drugs that could influence the tests.
Exclusion criteria: dementia, psychosis, acute suicide or homicide risk, other somatic illnesses (eg, cancer) that could possibly cause death in the near future. On admission day, all the data were collected, and the self-administered psychiatric questionnaires were filled in by the patients. On the same day, spirometry tests were performed in the patients using Jaeger device (Wuerzburg, Germany).
The measurement of maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP) was performed with the same device. This test is a quick and noninvasive clinical procedure for determining the index o inspiratory and expiratory muscle strength. It is useful in assessing the degree of abnormality and in monitoring respiratory muscle weakness in individual patients over time.Citation20
On admission day, the participants filled in the following two psychiatric questionnaires:
COPE Inventory: Elaborated by Carver et al,Citation21 COPE questionnaire is an instrument of self-defense that assesses the strategies that people use to cope with difficult or stressful life events. The scale contains 60 questions with answers rated on a scale from 1 to 4: where 1 represents “I usually don’t do this thing” and 4 represents “I often do this thing”. The evaluation of the modalities of coping was done by analyzing the next four levels: 1) problem-focused coping, which includes planning, active approach, and deletion of concurrent activities; 2) emotion-focused coping, which includes the positive interpretation and growth, restraint, and acceptance; 3) social support-focused coping, which includes the use of the social–instrumental support, the use of the social–emotional support, and the expression of feelings (venting of emotions); and 4) avoidant coping, which includes denial, mental, and behavioral deactivation. Higher subscale scores indicate greater use of that coping strategy.Citation22
The Hospital Anxiety and Depression Scale is a self-administered questionnaire that detects and distinguishes between anxiety and depression and measures the severity of emotional disorder. The questionnaire consists of just 14 items selected to be relatively unaffected by physical illness; hence, it is quick to complete. It contains two subscales: one evaluates anxiety and the other evaluates depression (each of them consists of seven items). Each item has four possibilities/alternatives of answers that reflect the severity marked from 0 to 3. The two subscale scores are registered separately from 0 to 21. The appreciation score of the intensity of anxiety and depression is the following: 0–7 normal, 8–10 mild, 11–14 moderate, and 15–21 severe.
Functional exercise capacity was assessed using the 6-minute walking test (6MWT) according to the guidelines of the American Thoracic Society.Citation23 The shortness of breath was evaluated with the Borg scale in which the subjects report symptoms associated with a current physical activity. The Borg scale rates dyspnea on a scale of 0–10 to quantify the intensity of shortness of breath during activity.
The coping style was compared using the following medical determinants: forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1) obtained though spirometry, MIP, MEP, functional exercise level through 6MWT, and dyspnea with the help of the Borg scale.
According to their higher coping subscale scores, they were classified into one dominant coping type as follows: patients with problem-focused coping type, emotion-focused coping, social support-focused coping, avoiding coping type. Based on this classification, the studied group was divided into four subcohorts and was analyzed accordingly.
Statistical analysis
Data were collected and analyzed using the SPSS v.17 software suite (SPSS Inc., Chicago, IL, USA) and are presented as medians and interquartile range for continuous variables without Gaussian distribution or average ± standard deviation for continuous variables with Gaussian distribution. To assess the significance of the differences between groups (problem-focused coping, emotion-focused coping, social support-focused coping, and avoidance-type coping), Mann–Whitney U and Kruskal–Wallis tests (medians, non-Gaussian populations), unpaired t-student, and analysis of variance (averages, Gaussian populations) tests, respectively, were used. Continuous variable distributions were tested for normality using Shapiro–Wilk test. The correlation between studied variables was evaluated using Spearman’s rank sum correlation coefficient (non-Gaussian distributed variables), and the statistical significance was assessed using the t-distribution score test. In this study, a P-value <0.05 was considered as the threshold for statistical significance.
Results
In this cross-sectional study, 28 patients with COPD were enrolled. According to their higher coping subscale score, they were classified in one dominant coping type as follows: patients with problem-focused coping type (n=9), emotion-focused coping (n=10), social support-focused coping (n=6), avoiding coping type (n=3).
The four cohorts had similar general characteristics: age (average ranging from 56.3 to 61.5 years; P=0.442), body mass index (average ranging from 21.6 to 27.5 kg/m2; P=0.655), and education level (all medians 12 years of education; P=0.845), a fact which emphasizes that potential biases caused by these external factors are not to be found in our study.
The average coping scores in the entire studied cohort were as follows: problem-focused coping (33.2±8.2), emotion-focused coping (34.3±6.4), social support-focused coping (31.4±7.7), and avoidance-type coping (26.6±6.6).
The significant differences between the four studied subgroups regarding depression and anxiety are as follows: the depression score was the highest in patients with avoidance-type coping and the lowest in patients with problem-focused coping (11.0 vs 5.6; P=0.042); patients with social support-focused coping style had the highest anxiety score in contrast to patients with emotion-focused coping who had the lowest anxiety score (11.6 vs 5.0; P=0.006). presents the detailed comparison of the studied characteristics between the four subgroups.
Table 2 Studied group characteristics stratified according to their dominant coping type
With regard to respiratory parameters, significant differences were present for the variation of the medians among the four groups only for FVC% and 6MWT (%); patients with social support-focused coping type had the lowest FVC% (43%), and this value increases for patients with emotion-focused coping (47.5%), avoidance-type coping (53%), and problem-focused coping (59%). Regarding the 6MWT (%), the lowest score of the scale was observed for patients with social support-focused coping (26.5%), followed by patients with emotion-focused coping (83.5%) and problem-focused coping type (87%), whereas the highest value was observed in patients with avoidance-type coping (99.7%).
Although the variance among all the four groups was not statistically significant, the following patterns were observed: the FEV1% value was significantly lower in patients with social support-focused coping (16.5%) compared with any of the other three groups; the MIP% value was significantly higher in social support-focused coping type when compared with any other group; and the BORG scale score was significantly lower in patients with problem-focused coping type (a median score of 7). presents the association between the dominant coping type and respiratory parameters.
Table 3 Respiratory parameters in relation to the dominant coping type
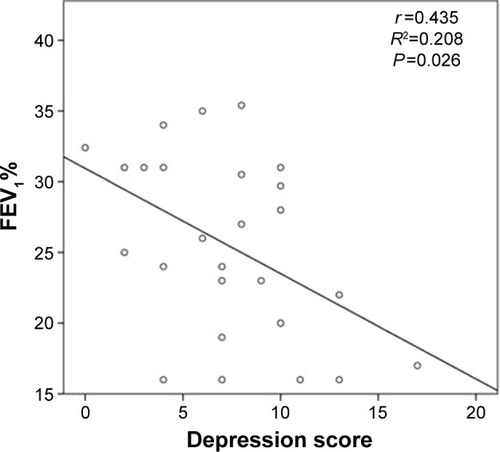
When the association between the four coping scales and the respiratory parameters were analyzed, different patterns of relationships were observed. Problem-focused coping score was significantly and positively associated with FVC% (Spearman’s r=0.400; P=0.035; ). Emotion-focused coping score was positively and significantly associated with FVC% (Spearman’s r=0.395; P=0.038; ). Social support-focused coping score was negatively and significantly correlated with FEV1/FVC% ratio (Spearman’s r=0.389; P=0.041), which means that a more significant social support-focused coping type is associated with the lower values of this ratio (). The other studied pairs of correlations had no statistical significance (). Regarding the association between anxiety or depression and respiratory parameters, a significant, negative correlation only between depression score and FEV1 (Spearman’s r=−0.435; P=0.026; ), denoting that patients with more advanced depression symptomatology have a decreased FEV1% value, was found in this study. The other pairs of studied variables were not significantly correlated ().
Table 4 Correlations between coping scales and respiratory parameters
Table 5 Correlations between depression, anxiety, and respiratory parameters
Figure 1 Correlation between problem-focused coping score and FVC%.
Abbreviation: FVC, forced vital capacity.
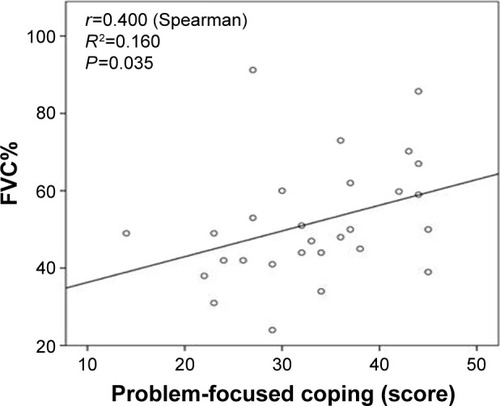
Figure 2 Relationship between emotion-focused coping score and FVC%.
Abbreviation: FVC, forced vital capacity.
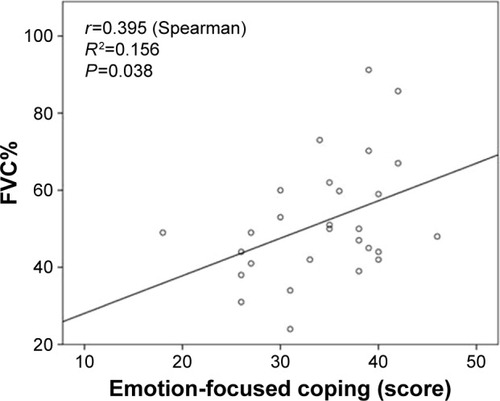
Figure 3 Correlation between social support-focused coping score and FEV1/FVC ratio.
Abbreviations: FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
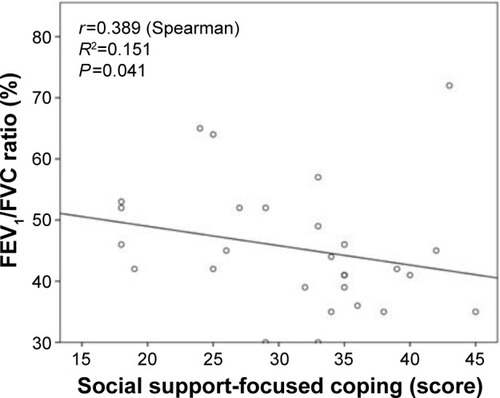
Figure 4 Correlation between depression score and FEV1%.
Discussion
The psychological features of a subject can influence his or her somatic condition, and in the case of those who suffer from COPD, it is a known fact that these can influence the way in which these people manage to control the disease toward a more favorable evolution.Citation24
However paradoxical as it may seem, there were studies on chronic somatic diseases that have proven that psychological factors may predict an outcome announced by different physical parameters better than the clinical variables. Therefore, a more complex psychological analysis of these people is considered to be very important for the management of this disease, among the psychological factors that require review are those related to coping.
This is the first article that evaluates coping styles in patients with COPD in Romania. There are studies in literature that have successfully applied the concept of coping in COPD. In patients suffering from lung disease, passive copings have been associated with a low quality of life, with a decrease in their professional performance, and with a worse mental state (as the presence of depression) although negative findings have also been reported.Citation25–Citation29
Moreover, a style of active coping (including problem-focused coping type), in patients with chronic somatic diseases (including patients who suffer from lung disease), has been associated with a better health-related quality of life and mental health symptoms.Citation26,Citation30–Citation32 While problem-focused coping type is considered adaptive and is negatively associated with stress, depression, and anxiety, avoidant coping is considered maladaptive and is associated positively with these.Citation33–Citation36 With regard to the emotion-focused coping and social support-focused coping, the findings in the literature are contradictory as to their association with stress, anxiety, and depression symptoms. This happens mainly as a result of the coping mechanisms that form these styles (levels) of coping as a consequence of the different definitions given in the literature. Therefore, emotion-focused coping contains positive interpretation, growth, abstinence, and acceptance. While positive interpretation, growth, and acceptance are considered active adaptive mechanisms, abstention has both an active and a passive one.Citation36
At social support-focused coping, coping mechanisms such as utilization of emotional, instrumental, and social support and also manifestation of emotions are found. Seeking social and emotional support is considered active and adaptive coping mechanisms.Citation37 On the other hand, manifestation of emotions is considered in general a maladaptive coping even though some authors find an adaptive dimension of it.Citation38,Citation39
In this study, patients who had predominantly a problem-focused coping style had the most reduced depressive symptomatology and those who had an avoidant coping style had the most intense depressive symptomatology, in accordance with the literature.Citation34,Citation40 With respect to anxious depressive symptomatology, patients suffering from COPD who had a predominant emotion-focused coping had the lowest level of anxiety meanwhile those who had a social support-focused and an avoidant coping are associated positively with its intensity. If for emotion-focused coping and social support-focused coping, the literature did not find any association between stress and anxious and depressive symptomatology, as it has been explained earlier, avoidant coping that was clearly mentioned has a positive association with the anxious symptomatology.Citation34,Citation41
Scharloo et alCitation25 have also found a positive association between seeking social support and anxiety level in their study on 24 subjects suffering from COPD. Therefore, patients with the highest intensity of depression had a predominant avoidant coping style, and those with the highest intensity of anxiety had a predominant social support-focused coping. As to the association of the coping style with respiratory parameters and exercise tolerance, there are only few studies in the literature for COPD patients, and the existing relation between these has not been clarified until now.Citation40,Citation42,Citation43
Buchi et alCitation42 in their study on 32 subjects suffering from COPD have found a major impact of the coping strategies on the improvement of lung functionality evaluated through the modification of the FEV1 value; only one mechanism of coping, wishful thinking, is significantly associated with a greater improvement in FEV1.
The present study is the first study that uses the well-validated COPE on Romanian population for this purpose. Those who had a predominant social support-focused coping style had significantly lower values of FVC, FEV1, and 6MWT but the highest values of MIP in comparison with other subgroups. Considering the fact that social support-focused coping has been significantly associated in a positive way with the FEV1/FVC ratio and the intensity of the anxious symptomatology has been the highest in this subgroup, it can be concluded that this type of coping is maladaptive in COPD subjects, although there is a positive association with MIP values. This latter association could be caused by the inclusion of some coping mechanisms into this style of coping, mechanisms that are considered adaptive (social, instrumental, and emotional social support). There are studies that mention that the use of seeking social support-focused coping style is not associated with better outcomes in COPD patients.Citation25,Citation43
Subjects with a predominant problem-focused coping style had significantly higher FVC values and significantly smaller values on the BORG scale, and also the same values on the depressive intensity in comparison with the other subgroups. Considering the positive statistical association of the problem-focused coping style with FVC values, a conclusion about the adaptive style of this coping as to COPD can be drawn.
With reference to emotion-focused coping, the positive association of this with FVC values and the fact that the intensity of the anxious symptomatology has been the lowest in the sublot of coping predominant style, the emotion-focused one, it is also concluded that this is a coping adaptive style for subjects with COPD.
Thus, the beneficial/unbeneficial role of emotion-focused coping and social support-focused coping varies in the literature; in the present study on subjects with COPD, emotion-focused coping has a positive role in the evolution of COPD disease both on a physical and a psychic level and social support-focused coping has a negative impact. Research studies to prove whether the efficiency of different styles of coping varies according to the type of lung disease have not been carried out so far.
It is interesting that a significant statistical correlation between the coping style considered maladaptive, avoidant-coping, and respiratory parameters or exercise tolerance has not been found. But the subgroup of subjects who had avoidant coping as a main coping style was significantly different from the other subgroup in that they had the highest values at the 6MWT. This result differs from the one mentioned by Stoilkova et al,Citation40 who has found that higher level of avoidance-type coping style was associated with a lower 6MWD.
The significant association between the different styles of coping is greater and more important, as it is not significantly intermediated by the intensity of depression and anxiety. So in this study the only significant association between respiratory parameters and psychiatric psychopathology was between the intensity of depression and FEV1 value. This is not enough to justify the significant association of coping styles with respiratory parameters, in this study, namely, the anxiety and depression represent confounding factors (the impact of the depression and anxiety on the functional status and on the patients with COPD physical health is well known).Citation44–Citation46 The exact interrelation between coping styles and these parameters warrants further investigation.
Until today, the relationship between coping styles and medical determinants in patients with COPD remains unknown. This could be explained by the fact that the use of an active coping style is related to higher self-esteem, life satisfaction, and compliance with medical advice, whereas avoidance-type coping style refers to poorer physical functioning in terms of depression, well-being, and functional disability.Citation47 Thus, it could be a direct relationship and also an indirect one, mediated by psychiatric comorbidities.Citation48 The studies that researched this aspect referred the aforementioned items as mechanisms, but all of them suggested the necessity of further studies in this area.Citation49–Citation52
The most important limitation of this study is the small sample size; however, a prior sample size analysis demonstrated that the study had an appropriate statistical power to support the conclusions drawn. Due to the small sample size, adjustment of the results with respect to other cofactors in a multivariate regression analysis was not possible. As a further direction, we aim at continuing the study in an increased cohort of patients, most probably in a multicenter setting. Another limitation of the study is the cross-sectional design, because it does not dynamically analyze the respiratory parameters, which may be an important predictor for the disease prognosis.
In case of a multidisciplinary approach, identifying the coping styles in patients with COPD represents an important aspect of the individualized treatment of the patient. Thus, for those with avoidant or social support-focused coping, psychological intervention such as cognitive behavior therapy is necessary to either support them or change them to more of a problem/emotional coping style. Cognitive behavior therapy is a form of psychotherapy useful for patients with COPD with maladaptive coping style as well as for those with psychiatric comorbidities such as depression and anxiety.Citation53
The only relevant study that analyzes the prevalence of COPD in Romania has shown that in 10,000 people 23% has obstructive ventilator dysfunction.Citation54 The present study is the first study that analyzes this type of association in the Romanian population with COPD. In our opinion, its importance is enhanced by the characteristics of this population, having significant evidence, which point out to a set of psychological particularities of the Romanian population when compared with other populations in which this relationship has been previously analyzed.
Conclusion
The study findings point out the following: a negative impact of avoidance and social support-focused coping types, on both depression and anxiety; two frequent comorbidities associated with COPD on the respiratory parameters in these patients, demonstrating the fact that interventions aiming at enhancing the problem- or emotion-focused coping may improve COPD prognosis.
Regarding biological parameters, significant correlations were found between problem-coping score, emotion-focused coping score, and FVC% as well as between social support-focused coping and FEV1/FVC% ratio. Research studies on larger groups of patients are needed to clarify the correlation between each mechanism of coping with the biological parameters.
This study demonstrates the paramount importance of the multidisciplinary approach in patients with COPD, emphasizing on the collaboration between the pulmonologist and the psychiatrist.
Disclosure
The authors report no conflicts of interest in this work.
References
- PommerAMPouwerFDenolletJPopVJMManaging co-morbid depression and anxiety in primary care patients with asthma and/or chronic obstructive pulmonary disease: study protocol for a randomized controlled trialTrials20121361322236488
- ParekhPIBlumenthalJABabyakMAPsychiatric disorder and quality of life in patients awaiting lung transplantationChest200312451682168814605035
- KunikMERoundyKVeazeyCSurprisingly high prevalence of anxiety and depression in chronic breathing disordersChest200512741205121115821196
- HynninenKMJBreitveMHWiborgABPallesenSNordhusIHPsychological characteristics of patients with chronic obstructive pulmonary disease: a reviewJ Psychosom Res200559642944316310027
- LacasseYRousseauLMaltaisFPrevalence of depressive symptoms and depression in patients with severe oxygen-dependent chronic obstructive pulmonary diseaseJ Cardiopulm Rehabil2001212808611314288
- BorakJSliwinskiPPiaseckiZZielinskiJPsychological status of COPD patients on long term oxygen therapyEur Respir J19914159622026240
- VögeleCvon LeupoldtAMental disorders in chronic obstructive pulmonary disease (COPD)Respir Med2008102576477318222685
- Van ManenJGBindelsPDekkerFJzermansCJIvan der ZeeJSSchadeERisk of depression in patients with chronic obstructive pulmonary disease and its determinantsThorax200257541241611978917
- DoyleTPalmerSJohnsonJAssociation of anxiety and depression with pulmonary-specific symptoms in chronic obstructive pulmonary diseaseInt J Psychiatry Med201345218920223977821
- DalalAAShahMLunacsekOClinical and economic burden of depression/anxiety in chronic obstructive pulmonary disease patients within a managed care populationCOPD20118429329921827298
- AtlantisEFaheyPCochraneBBidirectional associations between clinically relevant depression or anxiety and COPD: a systematic review and meta-analysisChest2013144376677723429910
- SodeBFDahlMNordestgaardBGMyocardial infarction and other comorbidities with chronic obstructive pulmonary disease: a Danish Nationwide study of 7.4 million individualsEur Heart J201132192365237521875856
- YohannesAMAlexoupolosGSDepression and anxiety in patients with COPDEur Respir Rev20142313334534925176970
- FerrerMAlonsoJMoreraJChronic obstructive pulmonary disease stage and health-related quality of lifeAnn Intern Med199712712107210799412309
- KetelaarsCASchlosserMAMostertRHuyer Abu-SaadHHalfensRJWoutersEFDeterminants of health-related quality of life in patients with chronic obstructive pulmonary diseaseThorax199651139438658367
- WijnhovenHAKriegsmanDMHesselinkAEde HaanMSchellevisFGThe influence of co-morbidity on health-related quality of life in asthma and COPD patientsRespir Med200397546847512735662
- WijnhovenHAKriegsmanDMHesselinkAEPennixBWde HaanMDeterminants of different dimensions of disease severity in asthma and COPDChest200111941034104211296166
- HabraMELindenWAndersonJCWeinbergJType D personality is related to cardiovascular and neuroendocrine reactivity to acute stressJ Psychosom Res200355323524512932797
- RabeKFHurdSAnzuetoAGlobal Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2007176653255517507545
- McelvaneyGBlackieSMorrisonNJWilcoxPGFairbarnMSPardyRIMaximal static respiratory pressures in the normal elderlyAm Rev Respir Dis198913912772812912349
- CarverCSScheierMFWeintraubJKAssessing coping strategies: a theoretically based approachJ Pers Soc Psychol19895622672832926629
- CrasovanDISavaFATranslation, adaptation and validation on Romanian population of COPE questionnaire for coping mechanisms analysisCogn Brain Behav20131716176
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function LaboratoriesATS statement: guidelines for the six-minute walk testAm J Respir Crit Care Med2002166111111712091180
- TselebisABratisDKosmasEPsychological symptom patterns and vital exhaustion in outpatients with chronic obstructive pulmonary diseaseAnn Gen Psychiatry20111013222145925
- ScharlooMKapteinAAWeinmanJAWillemsLNARooijmansHGMPhysical and psychological correlates of functioning in patients with chronic obstructive pulmonary diseaseJ Asthma2000371172910724295
- CohenFLazarusRSActive coping processes, coping dispositions, and recovery from surgeryPsychosom Med19733553753894803347
- MyaskovskyLDewMASwitzerGEAvoidant coping with health problems is related to poorer quality of life among lung transplant candidatesProg Transplant200313318319214558632
- BurkerEJEvonDMSedwayJAEganTAppraisal and coping as predictors of psychological distress and self-reported physical disability before lung transplantationProg Transplant200414322223215495782
- De VitoDADewMAStilleyCSPsychosocial vulnerability, physical symptoms and physical impairment after lung and heart-lung transplantationJ Heart Lung Transplant200322111268127514585388
- Snow-TurekALNorrisMPTanGActive and passive coping strategies in chronic pain patientsPain19966434554628783309
- TaylorJLSmithPJBabyakMACoping and quality of life in patients awaiting lung transplantationJ Psychosom Res2008651717918582615
- GibsonKRuedaSRourkeSBMastery and coping moderate the negative effect of acute and chronic stressors on mental health-related quality of life in HIVAIDS Patient Care STDS201125637138121492004
- WijndaeleKMattonLDuvigneaudNAssociation between leisure time physical activity and stress, social support and coping: a cluster-analytical approachPsychol Sport Exerc200784425440
- HolahanCJHolahanCKMoosRHBrennanPLSchutteKKStress generation, avoidance coping, and depressive symptoms: a 10-year modelJ Consult Clin Psychol200573465866616173853
- SherbourneCHaysRDWellsKBPersonal and psychosocial risk factors for physical and mental health outcomes and course of depression among depressed patientsJ Consult Clin Psychol19956333453557608346
- KnibbRCHortonSLCan illness perceptions and coping predict psychological distress amongst allergy sufferers?Br J Health Psychol200813110311917535490
- HundtNEBensadonBAStanleyMACoping mediates the relationship between disease severity and illness intrusiveness among chronically ill patientsJ Health Psychol Epub2013121
- BouteyreEMaurelMBernaudJLDaily hassles and depressive symptoms among first year psychology students in France: the role of coping and social supportStress Health20072329399
- NinotGFortesMPoulainMGender difference in coping strategies among patients enrolled in an inpatient rehabilitation programHeart Lung200635213013616543043
- StoilkovaAWoutersEFMSpruitMAFranssenFMEJanssenDJAThe relationship between coping styles and clinical outcomes in patients with COPD entering pulmonary rehabilitationCOPD201310331632323713594
- CrockettLJIturbideMITorres StoneRAMcGinleyMRaffaelliMCarloGAcculturative stress, social support, and coping: Relations to psychological adjustment among Mexican American college studentsCultur Divers Ethnic Minor Psychol200713434735517967103
- BuchiSVilligerBSenskyTPsychosocial predictors of long-term success of in-patient pulmonary rehabilitation of patients with COPDEur Respir J1997106127212779192928
- StoilkovaAJanssenDJAFranssenFMESpruitMAWoutersEFMCoping styles in patients with COPD before and after pulmonary rehabilitationRespir Med2013107682583323541485
- YohannesAMBaldwinRCConnollyMJDepression and anxiety in elderly outpatients with chronic obstructive pulmonary disease: prevalence, and validation of the BASDEC screening questionnaireInt J Geriatr Psychiatry200015121090109611180464
- FelkerBKatonWHedrickSCThe association between depressive symptoms and health status in patients with chronic pulmonary diseaseGen Hosp Psychiatry2001232566111313071
- ClelandJALeeAJHallSAssociations of depression and anxiety with gender, age, health-related quality of life and symptoms in primary care COPD patientsFam Pract200724321722317504776
- MaesSLeventhalHde RidderDTDCoping with chronic illnessZeidnerMEndlerNSHandbook of CopingNew YorkWiley & Sons1996221251
- GiltayEJZitmanFGKromhoutDDispositional optimism and the risk of depressive symptoms during 15 years of follow-up: The Zutphen Elderly StudyJ Affect Disorder20069114552
- HandCHBradleyCHealth beliefs of adults with asthma: toward an understanding of the differences between symptomatic and preventive use of inhaler treatmentJ Asthma19963353313388827940
- KlagSBradleyGThe role of hardiness in stress and illness: an exploration of the effect of negative affectivity and genderBr J Health Psychol20049213716115125801
- Flensborg-MadsenTVentegodtSMerrickJSense of coherence and physical health. A review of previous findingsScientificWorldJournal2005566567316127599
- EschlemanKJBowlingNAAlarconGMA meta-analytic examination of hardinessInt JStress Manag2010174277307
- Popa-VeleaOPurcareaVLPsychological intervention – a critical element of rehabilitation in chronic pulmonary diseasesJ Med Life20142727428125408739
- MihaltanFFurtunescuFNemesRPrevalenta BPOC in Romania 2011–2012–Prima ancheta national ace a inclus si explorarea functional spirometrica, Studiu realizat de TOTEM Research pentru Centrul pentru Politici si Servicii de Sanatate