
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
In addition to lung involvement, several other diseases and syndromes coexist in patients with chronic obstructive pulmonary disease (COPD). Our purpose was to investigate the prevalence of idiopathic arterial hypertension (IAH), ischemic heart disease, heart failure, peripheral vascular disease (PVD), diabetes, osteoporosis, and anxious depressive syndrome in a clinical setting of COPD outpatients whose phenotypes (predominant airway disease and predominant emphysema) and severity (mild and severe diseases) were determined by clinical and functional parameters.
Methods
A total of 412 outpatients with COPD were assigned either a predominant airway disease or a predominant emphysema phenotype of mild or severe degree according to predictive models based on pulmonary functions (forced expiratory volume in 1 second/vital capacity; total lung capacity %; functional residual capacity %; and diffusing capacity of lung for carbon monoxide %) and sputum characteristics. Comorbidities were assessed by objective medical records.
Results
Eighty-four percent of patients suffered from at least one comorbidity and 75% from at least one cardiovascular comorbidity, with IAH and PVD being the most prevalent ones (62% and 28%, respectively). IAH prevailed significantly in predominant airway disease, osteoporosis prevailed significantly in predominant emphysema, and ischemic heart disease and PVD prevailed in mild COPD. All cardiovascular comorbidities prevailed significantly in predominant airway phenotype of COPD and mild COPD severity.
Conclusion
Specific comorbidities prevail in different phenotypes of COPD; this fact may be relevant to identify patients at risk for specific, phenotype-related comorbidities. The highest prevalence of comorbidities in patients with mild disease indicates that these patients should be investigated for coexisting diseases or syndromes even in the less severe, pauci-symptomatic stages of COPD. The simple method employed to phenotype and score COPD allows these results to be translated easily into daily clinical practice.
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous condition diagnosed by not completely reversible airflow obstruction detected during spirometry. Beyond this unifying functional definition, it is known that the lung may react to cigarettes smoking and environmental exposure with conductive airways remodeling or parenchymal destruction. The prevalence of airways or parenchymal changes determines the prevalent phenotype of COPD. The extent and the concomitance of airways and parenchymal changes determine the severity of the disease. In the last few years, several methods to identify the predominant phenotype and the severity of COPD in clinical practice have been proposed.Citation1–Citation5
In addition to lung involvement, several “comorbidities” may coexist in patients with COPD such as cardiovascular disease, metabolic dysfunctions, and anxious–depressive disorders as the most commonly reported. A number of potential biological mechanisms linking COPD and comorbidities have been proposed: the proinflammatory milieu,Citation6–Citation8 increased oxidative stress,Citation9 increased arterial stiffness,Citation10,Citation11 catabolic state,Citation12 and sedentary lifestyle.Citation13 As a matter of fact, patients with COPD are often “multi-diseased patients,” presenting different clinical pictures, with a poorer quality of life and outcomes,Citation14 and a high disease-related burden.Citation15,Citation16 They also need a complex diagnostic and therapeutic approach.Citation17
The prevalence of the various comorbidities in COPD varies widely according to the methods used to define phenotype and severity of the disease.Citation18–Citation22 The purpose of this study is to investigate the prevalence of idiopathic arterial hypertension (IAH), ischemic heart disease (IHD), heart failure (HF), peripheral vascular disease (PVD), diabetes (D), osteoporosis (O), and anxious depressive syndrome (ADS) in a clinical setting of COPD outpatients whose predominant phenotype and severity were determined by a standardized method, derived from computerized tomography (CT),Citation2 allowing patients to be classified based on simple clinical and pulmonary function parameters.
Materials and methods
Patients
A total of 412 outpatients with COPD (299 males), in stable clinical condition were consecutively enrolled and completed the study. The ethical committee of the University Hospital of Florence approved the study and an informed consent was signed by each patient.
Patients’ evaluation consisted of a thorough clinical history and physical examination. Severity of dyspnea was assessed by the modified Medical Research Council (mMRC) dyspnea scale. Static and dynamic lung volumes and single breath diffusing capacity (DLCO) were measured (V6200 Autobox Body Plethysmograph; Sensor Medics, Yorba Linda, CA, USA) according to American Thoracic Society/European Respiratory Society guidelines and expressed as percentage of the predicted values (%).Citation23 Each patient was assigned a predominant airway or predominant emphysematous phenotype and a mild or severe category of disease according to the results of a multivariate analysis of 14 continuous variables (age, years; body mass index [BMI]; pack/years; forced vital capacity [FVC]% predicted; forced expiratory volume in 1 second [FEV1] % predicted; FEV1/vital capacity [VC] and FEV1/FVC ratios, total lung capacity [TLC] % predicted, residual volume [RV] % predicted, RV/TLC ratio, functional residual capacity [FRC] % predicted; VC% predicted; inspiratory capacity [IC] % predicted; DLCO % predicted plus three categorical variables (mMRC dyspnea scale, cough, and sputum, scored as follows: dyspnea [0= none; 1= slight; 2=moderate; 3= severe; 4= very severe]; cough [0= absent; 1=occasional; 2= chronic]; and sputum [0= absent/occasional; 1= chronic non-purulent; 2= chronic purulent]), which have been validated by quantitative CT.Citation2 The variables entered to classify COPD patients according to the predominant mechanism of airflow limitation were DLCO%, TLC%, and sputum purulence. These variables were linearly combined to determine the relative predominance of an airway or emphysema phenotype according to the following computation. Sputum purulence was assigned a categorical value (0, absent; 1, present).
Patients were classified as being affected by predominant emphysema or by predominant airway disease when the result of the above-mentioned equation was either positive or negative, respectively.Citation2
FEV1/VC ratio, FRC%, and sputum purulence were entered to classify the severity of the disease. These variables were linearly combined to compute the COPD severity score according to the following equation:
Patients were classified as being affected by severe or mild disease when the result of the computation was positive or negative, respectively.Citation2
Comorbidities
The following comorbidities were chosen to investigate cardiovascular, metabolic, and behavioral domains in patients with COPD. We ascertained the presence of IAH, IHD, HF, PVD, D, O, and ADS by means of an interview, outcomes of functional diagnostic procedures, and current medical treatment. The presence of each comorbidity was confirmed by the investigators through a detailed review of available medical records and medications or therapy specific to any disease. Self-reported diagnoses were not considered.
Statistical analysis
Data were presented as mean ± standard deviation for continuous variables, and as counts and proportions for nominal and ordinal variables. The Student’s t-test was used to compare the mean of continuous variables among different subsets of patients. The Fisher’s exact test was used to compare the prevalence of categorical variables among different subsets of patients. The significance level was set at P<0.05.
Results
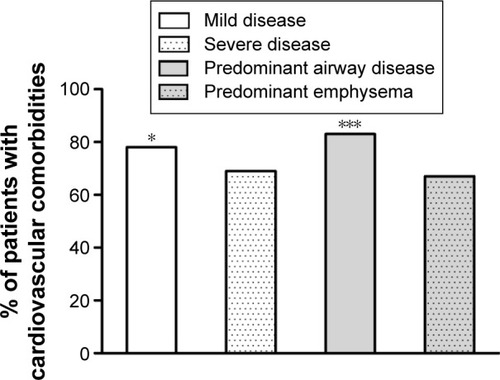
Anthropometric, smoke exposure, and functional data of the recruited patients and classification according to the prevailing phenotype and severity of the disease are reported in . Mild and severe COPD patients were matched for age. No difference in smoke exposure was found across the subgroups. Compared with patients with predominant airway disease, those with predominant emphysema were younger, with a lower BMI and a more impaired lung function involving all the considered functional variables. shows the number of comorbidities in the whole set and according to prevailing phenotype and disease severity. No comorbidities were found in 16% of patients (65 out of 412). In more details, 29 (13%) predominant airway disease patients and 36 (19%) predominant emphysema patients had no detectable comorbidities. The number of patients with no comorbidities was similar in both the subgroups. The vast majority of patients turned out to be affected by two or three comorbidities (). reports the overall prevalence of each comorbidity. and display the prevalence of each comorbidity within each of the two phenotypes. Out of 422 patients, 347 (84%) had at least one comorbidity. The most frequent was IAH, which affected 62% of the patients, followed by PVD (28%). shows the prevalence of comorbidities in the two phenotypes. While IAH was significantly more prevalent in patients with predominant airway disease, osteoporosis prevailed in those with predominant emphysema. As for COPD severity (), we found a significantly higher prevalence of IHD and PVD in patients with mild COPD. Out of 412 patients, 309 (75%) were affected by at least one cardiovascular comorbidity. The prevalence of all considered cardiovascular comorbidities was significantly higher in patients with mild disease and in those with predominant airway phenotype of COPD ().
Table 1 Anthropometric and functional data in patients with COPD according to phenotypes and severity of the disease
Table 2 Number of comorbidities in patients with COPD according to phenotypes and severity of the disease
Figure 1 Prevalence of comorbidities in 412 outpatients with COPD.
Abbreviations: ADS, anxious depressive syndrome; com, comorbidities; COPD, chronic obstructive pulmonary disease; D, diabetes; HF, heart failure; IAH, idiopathic arterial hypertension; IHD, ischemic heart disease; O, osteoporosis; PVD, peripheral vascular disease.
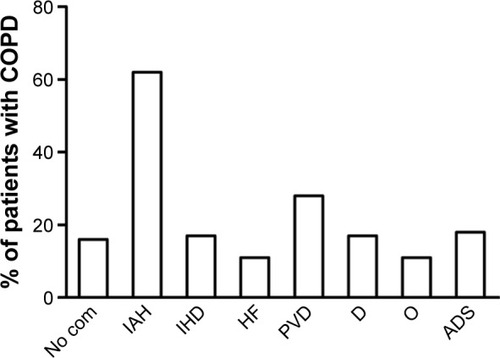
Figure 2 Prevalence of comorbidities in 222 patients with the predominant airway disease (A) phenotype and in 190 patients with the predominant emphysema phenotype (B).
Abbreviations: ADS, anxious depressive syndrome; com, comorbidities; D, diabetes; HF, heart failure; IAH, idiopathic arterial hypertension; IHD, ischemic heart disease; O, osteoporosis; PVD, peripheral vascular disease.
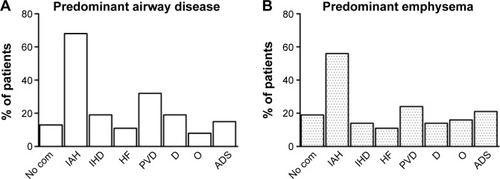
Figure 3 Comparisons of the prevalence of each examined comorbidity in 222 patients with a predominant airway disease phenotype and in 190 patients with a predominant emphysema phenotype.
Note: *P<0.05.
Abbreviations: ADS, anxious depressive syndrome; com, comorbidities; D, diabetes; HF, heart failure; IAH, idiopathic arterial hypertension; IHD, ischemic heart disease; O, osteoporosis; PVD, peripheral vascular disease.
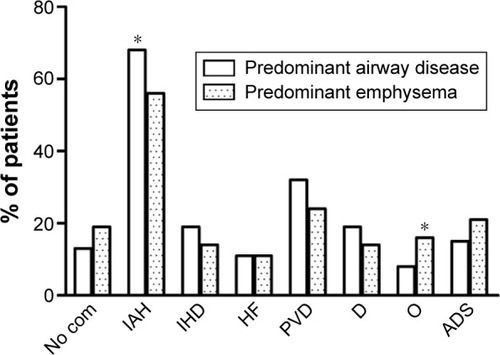
Figure 4 Prevalence of comorbidities in 412 outpatients according to mild or severe grade of COPD.
Notes: *P<0.05; ***P<0.0001.
Abbreviations: ADS, anxious depressive syndrome; com, comorbidities; COPD, chronic obstructive pulmonary disease; D, diabetes; HF, heart failure; IAH, idiopathic arterial hypertension; IHD, ischemic heart disease; O, osteoporosis; PVD, peripheral vascular disease.
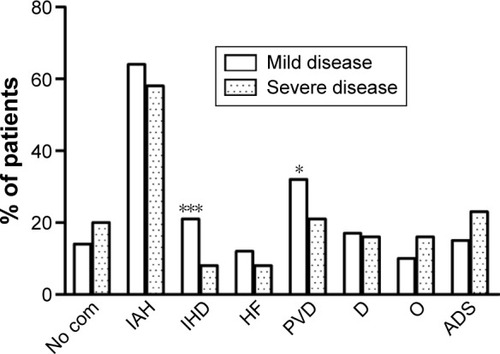
Figure 5 Prevalence of cardiovascular comorbidities in 412 outpatients according to mild or severe grade of COPD and according to the predominant phenotype. Notes: *P<0.05; ***P<0.0001.
Discussion
The main finding of this study was that specific comorbidities prevailed in the two considered phenotypes of COPD; notably the highest prevalence of comorbidities was found among patients with mild stage of the disease. In particular, IAH was significantly more prevalent in patients with the predominant airway phenotype, whereas osteoporosis seemed to prevail in the predominant emphysema phenotype. In addition, we found a significantly higher prevalence of IHD and PVD in the subset of patients with mild COPD. The second relevant result was that the cardiovascular comorbidities were found to be significantly more prevalent in patients with the predominant airways phenotype and with a milder expression of the disease.
A growing body of evidence suggests that COPD is associated with comorbidities whose prevalence varies largely among epidemiological studies. In this study, the prevalence of the whole set of considered comorbidity and cardiovascular comorbidities was consistent with those of Anecchino et al,Citation18 which was based upon a different method for comorbidity detection and classification. Indeed, they found at least one prescription of drugs for a chronic condition other than respiratory disease in a vast majority of their wide cohort of patients with COPD. It is important to underline that the presence of comorbidities in our study has been investigated by an objective method, with the exclusion of patients with a single drug prescription and/or a self-reported diagnosis, which was not considered probative for the presence of a comorbidity.
In our study, patients with predominant airway disease were slightly older than those with predominant emphysema. This result is in contrast with those of Feary et alCitation20 and Sode et alCitation19 who showed the highest risk of comorbidity in the youngest patients with COPD, suggesting to look for comorbidities at earlier stages of the disease. On the other hand, the present results of a higher prevalence of comorbidities in mild diseases’ severity confirm the hypothesis of individual susceptibility to factors implicated in the genesis of COPD, which could arise and develop up to different degrees of severity, and progress more or less into more severe stages independently of the age of the patients.
In patients with predominant airway phenotype of COPD, we observed that the most prevailing comorbidity was IAH. This result is consistent with that of Watz et al,Citation24 who detected IAH in a high proportion (73%) of patients with symptoms of chronic bronchitis without airflow limitation, as well as in those with mild COPD (77%). Interestingly, they found that circulatory markers of systemic inflammation were increased in patients with chronic bronchitis and COPD when metabolic syndrome was detected, irrespective of the degree of lung function impairment. Visceral adipocytes have been suspected to play a role by producing interleukin-6, which in turn induces the synthesis of C-reactive protein by hepatocytes. This finding has been confirmed in a study by Poulain et al,Citation25 who demonstrated that systemic inflammation was higher in obese patients with moderate COPD compared with those with normal weight and severe disease. We confirmed these observations indirectly, as BMI was significantly higher in patients with the predominant airway phenotype compared with those with predominant emphysema phenotype, and in moderate disease compared with severe disease.
Recently, new evidence has emerged suggesting that hypoxia, a frequent finding in patients with COPD, may be an additional cardiovascular risk factor for its role in the atherosclerosis process.Citation26–Citation29 Moreover, patients with COPD are often affected by a neglected condition such as sleep disorders, resulting in nighttime hypoxia. Obesity strongly contributes along with age and active smoking for sleep disordered breathing, accelerated pulmonary hypertension, obesity–hypoventilation syndrome, and obstructive sleep apnea, irrespective of the degree of airflow obstruction.Citation29
Hypoxia resulting from the above-mentioned conditions can be continuous or intermittent.Citation26 These high frequency cycles of hypoxia and reoxygenation are similar to ischemia–reperfusion injury and result in an increased production of reactive oxygen species and oxidative stress. Cell damage, remodeling of extracellular matrix and blood vessels, endothelial dysfunction, and inactivation of antiproteases are some of the consequences of oxidative imbalance. Furthermore, in animals models, chronic intermittent hypoxia increases the amount of oxidized lipids and low-density lipoproteins in serum and arterial walls, which have stronger atherogenic effects, such as the formation of plaques in arteries which start due to lipid peroxidation. These results have been confirmed and extended in a small cohort of patients with COPD and sustained nocturnal, nonapneic hypoxia, which showed increased levels of serum lipid peroxidation and decreased paraoxonase activity.Citation28
Patients with COPD and obesity, hypoventilation syndrome, and obstructive sleep apnea resemble the so-called “blue bloater” phenotypeCitation29 and also the predominant airway phenotype objectively classified in this paper.
Among the extrapulmonary effects of COPD, osteoporosis has been recognized as a major comorbidity. This association has been explained in terms of age, sex, reduced daily activity, chronic hypoxemia, and systemic corticosteroids therapy.Citation30 Recently, the presence of osteoporosis also in patients with milder airflow obstruction and clinically stable conditions has led to linking osteoporosis to a low-grade systemic inflammation sustained by increased plasma levels of C-reactive protein, interleukin-6, and tumor necrosis factor-α.Citation31 Furthermore, COPD exacerbations, associated with increased systemic inflammation, have been demonstrated to enhance osteoporosis progression.Citation32 The high prevalence of osteoporosis in the predominant emphysema phenotype in our study supports the view that, beyond a pure catabolic process, a mechanical derangement of lung structure due to hyperinflation and parenchymal disruption might also be relevant in sustaining a widespread chronic inflammation and its consequences. It could not be otherwise explained that a significant improvement of bone mineral density occurred 1 year after lung volume reduction surgery in patients with a pure, severe, CT-detected emphysema phenotype of COPD compared with a control group undergoing rehabilitation.Citation33
The other important finding of this study was that IHD and PVD are significantly more prevalent in the subset of patients with mild COPD. This finding is in keeping with the previous studiesCitation19,Citation20 demonstrating that the association between cardiovascular comorbidities and COPD is a risk factor for poor prognosis, hospitalization, and death of patients with mild COPD.Citation19 Our results showed that the highest burden of comorbidities is seen mostly in patients with less severe pulmonary disease. These findings were in agreement with findings of Watz et alCitation24 and in contrast with those of Mahboub et alCitation22 and Dal Negro et alCitation21 who reported an association between the prevalence of comorbidity and COPD severity measured by a COPD assessment test score >10 or by Global Initiative on Obstructive Lung Disease stages, respectively. Our results were also in contrast with Mannino et alCitation34 and Johnston et alCitation35 who reported a direct relationship between severity of airflow limitation and risk for cardiovascular diseases, and for IHD, arrhythmias, stroke, and IAH, each one considered separately. Furthermore, other studies failed to demonstrate any significant association between the prevalence of cardiovascular comorbidities and the severity of COPD evaluated by the level of airflow obstruction in a small cohort of patients,Citation36 or by the degree of airflow obstruction, exercise capacity, and BODE index.Citation37
The discrepancies may be related to the method by which the disease severity was scored. Conceivably, disease severity is unlikely to be satisfactorily depicted by the reduction of a single functional parameter (eg, FEV1). Indeed, this has been the sole criterion employed to assess COPD severity in many studies, actually before the publication of the revised Global Initiative on Obstructive Lung Disease guidelines in 2011; here symptoms and clinical events (exacerbations) have been introduced first, along with airway obstruction, to describe a disease that is actually far more complex than airway obstruction alone. Furthermore, this functional feature also reflects at least two pathological mechanisms, namely reduction of airway caliber (due to inflammation) and reduction of elastic recoil (due to parenchymal destruction). We are confident that the method employed to investigate COPD in this study takes into account both the predominant mechanism of airway obstruction for phenotyping each patient and the total amount of parenchymal and airways involvement to score severity.Citation2
We acknowledge that this study has some limitations: 1) the small cohort of patients recruited; 2) the retrospective collection of data concerning diagnosis and therapy of each examined comorbidity; and 3) the methodology used to report the presence of a comorbidity that is not completely objective because it was not based on repeating or seeking confirmatory tests for each disease, a task that would have been prohibitively expensive.Citation14,Citation16 Therefore, based on this consideration and in keeping with most of the studies on the subject, we preferred to assess the presence of a comorbidity by means of a combination of clinical history and medical records documentation.
Conclusion
Understanding the association between comorbidities and phenotypes of COPD may be relevant to clarify the relationship between different pathophysiological mechanisms and such a disease: we can hypothesize to assign each phenotype of COPD a specific comorbidity panel.
The increased prevalence of comorbidities among patients with mild disease has several relevant practical aspects: first of all, the need of an early diagnosis of COPD, especially in those patients with slight symptoms who turn to general practitioners more often than to pulmonologists. For this purpose, we wish to stress that the results of this study can easily be translated into daily clinical practice due to the simple method suggested here to phenotype and score the disease. Accordingly, the complementary role of general practitioners and the specialist is highlighted in this study: given the large number of potential candidates to develop COPD, it would be impossible to care for all patients at a specialist level. A need exists to lay bridges and to share a common language that allow both specialists and general practitioners to diagnose and treat COPD and its comorbidities early and effectively, in order to slow the disease progression and improve the quality of life.Citation38,Citation39
Increasing knowledge on links between COPD and comorbidities could provide innovative treatment strategies and it would assign each patient with COPD targeted therapies according to their personalized profile of phenotype, severity, and comorbidity.Citation40
Acknowledgments
Professor Camiciottoli and Dr Diciotti were responsible for the funds allocation of the grant obtained by the Ministry of Health of Italy, Project Code: RF-2010-2321362.
Disclosure
The authors report no conflicts of interest in this work.
References
- PaolettiMCamiciottoliGMeoniEExplorative data analysis techniques and unsupervised clustering methods to support clinical assessment of chronic obstructive pulmonary disease (COPD) phenotypesJ Biomed Inform20094261013102119501190
- CamiciottoliGBigazziFPaolettiMCestelliLLavoriniFPistolesiMPulmonary function and sputum characteristics predict computed tomography phenotype and severity of COPDEur Respir J201342362663523258785
- BurgelPRPaillasseurJLRocheNIdentification of clinical phenotypes using cluster analyses in COPD patients with multiple comorbiditiesBiomed Res Int201442013424683548
- WeatherallMTraversJShirtcliffePMDistinct clinical phenotypes of airways disease defined by cluster analysisEur Respir J200934481281819357143
- MarshSETraversJWeatherallMProportional classifications of COPD phenotypesThorax200863976176718728201
- AgustíAEdwardsLDRennardSIEvaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotypePLoS One201275e3748322624038
- AgustíAGNogueraASauledaJSalaEPonsJBusquetsXSystemic effects of chronic obstructive pulmonary diseaseEur Respir J200321234736012608452
- GanWQManSFSenthilselvanASinDDAssociation between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysisThorax200459757458015223864
- MacNeeWPathogenesis of chronic obstructive pulmonary diseaseProc Am Thorac Soc20052425826616267346
- SabitRBoltonCEEdwardsPHArterial stiffness and osteoporosis in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2007175121259126517363772
- MaclayJDMcAllisterDAMillsNLVascular Dysfunction in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2009180651352019542477
- ScholsAMBroekhuizenRWeling-ScheepersCAWoutersEFBody composition and mortality in chronic obstructive pulmonary diseaseAm J Clin Nutr2005821535916002800
- Garcia-AymerichJLangePBenetMSchnohrPAntóJMRegular physical activity modifies smoking-related lung function decline and reduces risk of chronic obstructive pulmonary disease: a population-based cohort studyAm J Respir Crit Care Med2007175545846317158282
- ManninoDMHiguchiKYuTCEconomic burden of COPD in the presence of comorbiditiesChest2015148113815025675282
- GershonASMecredyGCGuanJVictorJCGoldsteinRToTQuantifying comorbidity in individuals with COPD: a population studyEur Respir J2015451515925142481
- WackerMEJörresRASchulzHfor COSYCONET-consortiumDirect and indirect costs of COPD and its comorbidities: results from the German COSYCONET studyRespir Med2016111394626725462
- TsiligianniIGKosmasEVan der MolenTTzanakisNManaging comorbidity in COPD: a difficult taskCurr Drug Targets201314215817623256716
- AnecchinoCRossiEFanizzaCDe RosaMTognoniGRomeroMWorking Group ARNO projectPrevalence of chronic obstructive pulmonary disease and pattern of comorbidities in a general populationInt J Chron Obstruct Pulmon Dis20072456757418268930
- SodeBFDahlMNordestgaardBGMyocardial infarction and other co-morbidities in patients with chronic obstructive pulmonary disease: a Danish Nationwide Study of 7.4 million individualsEur Heart J201132192365237521875856
- FearyJRRodriguesLCSmithCJHubbardRBGibsonJEPrevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary careThorax2010651195696220871122
- Dal NegroRWBonadimanLTurcoPPrevalence of different comorbidities in COPD patients by gender and GOLD stageMultidiscip Respir Med20151012426246895
- MahboubBAlzaabiAIqbalMNComorbidities associated with COPD in the Middle East and North Africa region: association with severity and exacerbationsInt J Chron Obstruct Pulmon Dis20161127328026917957
- PellegrinoRViegiGBrusascoVInterpretative strategies for lung function testsEur Respir J200526594896816264058
- WatzHWaschkiBKirstenAThe metabolic syndrome in patients with chronic bronchitis and COPD: frequency and associated consequences for systemic inflammation and physical inactivityChest200913641039104619542257
- PoulainMDoucetMDrapeauVMetabolic and inflammatory profile in obese patients with chronic obstructive pulmonary diseaseChron Respir Dis200851354118303100
- SongDFangGGreenbergHLiuSFChronic intermittent hypoxia exposure-induced atherosclerosis: a brief reviewImmunol Res2015631–312113026407987
- BernardoIBozinovskiSVlahosRTargeting oxidant dependent mechanisms for the treatment of COPD and its comorbiditiesPharmacol Ther2015155607926297673
- OkurHKPelinZYukselMYosunkayaSLipid peroxidation and paraoxonase activity in nocturnal cyclic and sustained intermittent hypoxiaSleep Breath201317136537122528954
- McNicholasWVerbraeckenJMarinJMSleep disorders in COPD: the forgotten dimensionEur Respir Rev20132212936537523997063
- JebouckABoonenSDecramerMJanssensWCOPD, bone metabolism and osteoporosisChest2011139364865721362651
- LindBFengYThe association of low bone mineral density with systemic inflammation in clinically stable COPDEndocrine201242119019522198912
- KiyokawaHMuroSOgumaTImpact of COPD exacerbations on osteoporosis assessed by chest CT scanCOPD20129323524222360380
- MineoTCAmbrogiVMineoDFabbriAFabbriniEMassoudRBone mineral density improvement after lung volume reduction surgery for severe emphysemaChest200512761960196615947308
- ManninoDMThornDSwensenAHolguinFPrevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPDEur Respir J200832496296918579551
- JohnstonAKManninoDMHaganGWDavisKJKiriVARelationship between lung function impairment and incidence or recurrence of cardiovascular events in a middle-aged cohortThorax200863759960518245145
- MethvinJNManninoDMCaseyBRCOPD prevalence in Southeastern Kentucky: the burden of lung disease studyChest2009135110210718689574
- VanfleterenLESpruitMAGroenenMClusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2013187772873523392440
- CelliBRRecommendation for the early diagnosis of COPD: The AIMAR viewMultidiscip Respir Med2015101625729573
- WelteTVogelmeierCPapiACOPD: early diagnosis and treatment to slow disease progressionInt J Clin Pract201569333634925363328
- BrownJPMartinezCHChronic obstructive pulmonary disease comorbiditiesCurr Opin Pulm Med201622211311826814720