
Abstract
Purpose
The fixed-dose dual bronchodilator combination (FDC) of tiotropium and olodaterol showed increased effectiveness regarding lung function and health-related quality of life in patients with chronic obstructive pulmonary disease (COPD) compared with the use of its mono-components. Yet, while effectiveness and safety have been shown, the health economic implication of this treatment is still unknown. The aim of this study was to assess the cost–utility and budget impact of tiotropium–olodaterol FDC in patients with moderate to very severe COPD in the Netherlands.
Patients and methods
A cost–utility study was performed, using an individual-level Markov model. To populate the model, individual patient-level data (age, height, sex, COPD duration, baseline forced expiratory volume in 1 second) were obtained from the tiotropium–olodaterol TOnado trial. In the model, forced expiratory volume in 1 second and patient-level data were extrapolated to utility and survival, and treatment with tiotropium–olodaterol FDC was compared with tiotropium. Cost–utility analysis was performed from the Dutch health care payer’s perspective using a 15-year time horizon in the base-case analysis. The standard Dutch discount rates were applied (costs: 4.0%; effects: 1.5%). Both univariate and probabilistic sensitivity analyses were performed. Budget impact was annually assessed over a 5-year time horizon, taking into account different levels of medication adherence.
Results
As a result of cost increases, combined with quality-adjusted life-year (QALY) gains, results showed that tiotropium–olodaterol FDC had an incremental cost-effectiveness ratio of €7,004/QALY. Without discounting, the incremental cost-effectiveness ratio was €5,981/QALY. Results were robust in univariate and probabilistic sensitivity analyses. Budget impact was estimated at €4.3 million over 5 years assuming 100% medication adherence. Scenarios with 40%, 60%, and 80% adherence resulted in lower 5-year incremental cost increases of €1.7, €2.6, and €3.4 million, respectively.
Conclusion
Tiotropium–olodaterol FDC can be considered a cost-effective treatment under current Dutch cost-effectiveness thresholds.
Introduction
The Global initiative for chronic Obstructive Lung Disease (GOLD) defines chronic obstructive pulmonary disease (COPD) as a common preventable and treatable disease, characterized by persistent airflow limitation that is usually progressive and associated with enhanced chronic inflammatory airway response to noxious particles or gases.Citation1 Exacerbations and comorbidities contribute to the overall severity of COPD. COPD has been projected to become the third largest cause of death by 2030, after cancer and cardiovascular disease.Citation2 While smoking is widely recognized as the major risk factor for COPD, especially in developing countries, biomass smoke and indoor cooking result in an increasing prevalence of COPD.Citation3
Besides nonpharmacologic treatments, several effective pharmacologic inhaled therapies for COPD are available. The main drug class to reduce symptoms and future risk in moderate to very severe COPD is the class of long-acting bronchodilators, that is, long-acting beta-agonists (LABA) and long-acting muscarinic antagonists (LAMA). In patients not sufficiently controlled with a single bronchodilator, a second bronchodilator of a different class may be added according to the GOLD guidelines. There seems a pharmacologic rationale for combining two classes of bronchodilatorsCitation4 and some studies indeed showed the added value compared with the use of a single bronchodilator,Citation5 but full synergistic effects have not been observed.
In addition to bronchodilators, inhaled corticosteroids (ICS) have been commonly used, often in a fixed-dose combination (FDC) with a bronchodilator. Although ICS are considered the cornerstone pharmacologic treatment in asthma patients, the use of ICS in patients with COPD is more controversial.Citation6 ICS can have both systemic and local side effectsCitation7,Citation8 and there seems limited added clinical value as compared with bronchodilators.Citation9 Recently, the WISDOM study showed that ICS could be stepped down safely, that is, without increased exacerbation risk, as long as dual bronchodilators were continued.Citation10
Spiolto Respimat® is a once-daily dual bronchodilator consisting of the FDC of the LAMA tiotropium and the LABA olodaterol delivered through the Respimat® Soft Mist inhaler. Tiotropium has been used for over a decade and is among the most commonly used therapies for patients with COPD. The effectiveness, safety, and cost-effectiveness of tiotropium have been evaluated in several large randomized controlled trials such as the UPLIFT and the POET.Citation11–Citation13 Due to its recent market introduction, so far only few studies have been performed with olodaterol; however, initial results seem beneficial with regard to its efficacy,Citation14,Citation15 and its safety profile is comparable with existing LABAs.Citation1
Recently, the FDC of tiotropium and olodaterol showed increased effectiveness regarding lung function, physical functioning, and health-related quality of life compared with the use of its mono-components.Citation16–Citation18 Yet, while effectiveness and safety have been shown, the cost-effectiveness of the new FDC is still unknown. In times of an increasing burden of chronic diseases on governmental health care budgets, there is an obvious need for economic evaluation of newly available treatments. Therefore, the aim of this study was to assess the cost-effectiveness of tiotropium–olodaterol FDC in patients with moderate to very severe COPD.
Materials and methods
Study design
A cost–utility analysis was performed, using an individual-level Markov model. A cost–utility analysis is a special type of cost-effectiveness analysis that uses the quality-adjusted life-year (QALY) as outcome measure.
Type of model
A deterministic individual-level Markov model was used in which patients were tracked over time rather than placed in fixed health states (such as GOLD 1, 2, 3, and 4). To populate the model, individual patient-level data (age, height, sex, COPD duration, baseline forced expiratory volume in 1 second value [FEV1]) were obtained from the tiotropium–olodaterol clinical TOnado trial.Citation16 As patient’s lung function declines, increased mortality risk, management costs, and exacerbation risk are seen, while quality of life decreases. These phenomena form the basis of the individual-based Markov model.Citation19
Note that an advantage of the current model from typical cohort models is that it is not “memory-less”, a common feature of Markov models in which the risk of future events is not affected by what has occurred in previous cycles. For example, the risk of exacerbation in future cycles increases based on the incidence of an exacerbation in the previous year, in line with observations in clinical studies.Citation20
Perspective
The cost–utility analysis was performed from the Dutch health care payer’s perspective. Applying a health care payer’s perspective implicates that only direct medical costs, such as medication, hospitalization, and primary care visits, were included. Indirect costs, such as work productivity losses,Citation21 were neglected as differences in these costs were not measured. In addition, as the vast majority of COPD patients were older than the legal retirement age, the relative contribution of these costs seems limited in this population.
Comparison
In the Markov model, treatment with tiotropium–olodaterol FDC was compared with treatment with tiotropium. Tiotropium is one of the most widely used drugs for COPD and is considered a suitable comparator to represent usual care in the Netherlands.Citation22 In addition, tiotropium has been used as comparator in a previous economic study that evaluated the cost-effectiveness of another FDC LABA–LAMA.Citation23
Cycle length
The cycle length of the model was 1 month in order to minimize the probability of patients experiencing multiple exacerbations in a given cycle and to fully capture the impact of exacerbations on costs and outcomes. Using a longer cycle length would not allow modeling of those patients who may suffer from exacerbations in consecutive months, which could be the case for COPD patients with the frequent exacerbator phenotype.Citation20 Shorter than 1-month cycle lengths would not be necessary in the current model as it is unlikely that a patient would experience more than one moderate or severe exacerbation within this time frame.Citation24 The cycle length was 1 month, however, the cycles through 52 weeks corresponded to the clinical trial visits and ranged from 2 to 12 weeks in duration.Citation16
Time horizon
The time horizon of the analysis was 15 years. As COPD is a chronic condition and according to the Dutch pharmacoeconomics guidelines, the model allowed patients to be followed over their lifetime, defined as a maximum period of 60 years, or a maximum age of 100 years given the minimum age of 40 years in the tiotropium–olodaterol FDC clinical trial. A 5-year time horizon may be considered the most comparable to published long-term trials in COPD considering that the studies providing clinical inputs (ie, lung function decline, exacerbation rates, mortality) all included follow-up times of <5 years. However, given the mean age of 64 years in the trial,Citation16 and the high rates of mortality in COPD patients compared with the general population, a 15-year time horizon was considered most appropriate.
Model assumptions
No adverse events related to treatment with bronchodilators were considered. This was justified given that side effects from bronchodilators are comparable across products and do not contribute significantly to either costs or outcomes of treatment. The model did not account for the possibility of differential rates of treatment switch. Differential add-on treatment and treatment discontinuation were not considered. All surviving patients died at an age of 100 years. These assumptions have been chosen as there is no indication from clinical trials that any of the available bronchodilator combinations differ in these aspects. Accounting for these aspects would therefore not directly bias the analysis in favor or against tiotropium–olodaterol FDC.
Model inputs
Lung function decline
Following treatment initiation, improvement in FEV1 was tracked in clinical visits in the clinical trial up to 52 weeks for the assessment of tiotropium–olodaterol FDC versus tiotropium.Citation16 Classification of patients according to severity level was done using postbronchodilator trough FEV1 values so that patients were classified by their potential to achieve a given level of lung function. Patients were classified into GOLD stages based on FEV1 using the GOLD 2007 criteria (GOLD stage II: 50%≤ FEV1 predicted <80%, stage III: 30%≤ FEV1 predicted <50%, stage IV: FEV1 predicted <30%) (Table S1).
After the trial period of 52 weeks, a constant linear decline in FEV1 was applied over time, not differentiated by treatment, but by the GOLD severity stage. As of its long-term follow-up (4 years), the rates of decline by severity stage observed in the tiotropium arm of the UPLIFT trial are currently used in the model, with greater declines in the less severe stages (Table S2). These differential rates of decline obtained from the UPLIFT trialCitation25 are consistent with the findings of a review that concluded that lung function decline is more prominent earlier in the disease.Citation26 Given that UPLIFT is one of the longest recent clinical trials on tiotropium in COPD, with published rates of decline that vary by GOLD stage, this was chosen as the best data source of lung function decline.Citation25 The study was exempted from IRB approval because of the use of anonymized data. Written informed consent was also therefore not sought.
Exacerbation risk
Exacerbation risk in the base case was estimated based on a random-effects logistic regression analysis of patient-level data of exacerbations from the 4-year UPLIFT trial comparing treatment with tiotropium to placebo. Using data from the tiotropium treatment group only, the risks regarding the dichotomous outcomes of moderate exacerbation (nonsevere) and hospitalization due to severe exacerbation within a month were estimated. The explanatory variables in the regression analyses (Tables S3 and S4) included exacerbations in previous year, FEV1% predicted, hospitalizations in previous year, and patients’ age in months. There was no direct effect of tiotropium–olodaterol on exacerbation risk modeled. However, exacerbation was indirectly influenced as a result of improved lung function in the tiotropium–olodaterol FDC arm in the first 52 weeks, compared with tiotropium.Citation16
Mortality
Patients faced a mortality risk in every cycle in the model and the exact risk was calculated as a function of COPD severity stage. Excess mortality due to COPD was obtained by comparing mortality with GOLD stage in the clinical trial versus the general population mortality adjusted by age and sex. The mortality rate applied in each cycle was obtained from two sources. The first source was a study of a large cohort of COPD patients in which mortality was a primary outcome that was used to estimate the excess mortality in COPD patients.Citation27,Citation28
Mortality in the general population by age and sex was obtained from the Dutch Bureau of Statistics. Mortality risk was not impacted by the incidence of exacerbations given that it would be double counting the risk. Previous published models used similar approaches to calculate mortality, differing mainly in the data source used to obtain the mortality risk.Citation29
Utilities
In order to reflect the impaired quality of life in patients with COPD, utility weights were assigned independently to each disease state, and to each exacerbation event.
In the base case, previously published utility values were used.Citation30 Utility weights by disease state (Table S2) had been derived from a representative subset of patients enrolled in the UPLIFT trial.
Consistent with previous cost-effectiveness models of bronchodilator treatment in COPD, patients experienced a temporary decrement in utility during an exacerbation, lasting the duration of one cycle before returning to their previous utility level, assigned by severity stage.Citation31 The magnitude of the utility decrement varied by whether the patient experienced a severe or nonsevere exacerbation. The utility decrement multipliers for each type of exacerbation obtained from the published literature were applied in the same way regardless of which data source for baseline utility values was used. Utility decrements following nonsevere and severe exacerbation were 0.85 and 0.50, respectively.Citation32,Citation33
Costs
Since the perspective adopted for the base-case analysis was that of the Dutch health care payer, the model reflected direct medical expenditures associated with bronchodilator therapy and other COPD treatments. All health care costs were expressed in 2014 Euros. An overview of the costs is provided in .
Table 1 Cost parameters
Discounting
For costs occurring after 1 year, a discount rate of 4% was applied in line with the Dutch guidelines. For effects occurring after 1 year, a discount rate of 1.5% was applied in line with the Dutch guidelines.Citation34
Outcomes
Clinical outcomes included life years, exacerbation free months per patient per year, annual nonsevere exacerbations, and annual severe exacerbations. In addition, an incremental cost-effectiveness ratio (ICER) was calculated with the formula Δcosts/Δeffects, with effects expressed as QALYs gained.
Model validation
The model has been used in a previous study and has been compared with existing COPD models.Citation19 In addition, the model has been validated against results from the TOnado trial. It was found that total exacerbations were similar to the numbers observed in the trial, while modeled mortality was slightly higher.Citation19
Sensitivity analyses
Both univariate and probabilistic sensitivity analyses were conducted.
Univariate sensitivity analysis allows the investigator to determine the impact of uncertainty around one model input on the cost-effectiveness results, while probabilistic analysis is conducted by taking values from statistical distributions (often based on confidence intervals or fixed deviations from the best estimate) for several parameters at the same time. When confidence intervals were not specified in a given data source, it was by authors’ consensus decided to modify inputs relating to costs and utilities by ±15%, in line with a previous COPD cost-effectiveness study.Citation35
The probabilistic sensitivity analysis (PSA) was based on a Monte Carlo simulation, where the model was run a large number of times (ie, 100 times) with different sets of inputs simulated according to statistical distributions (Table S5) that were assigned for all parameters, surrounded by uncertainty likely to have a significant impact on the cost-effectiveness results. The choice of statistical distribution used for each parameter included in the PSA was based on published recommendations for economic evaluation in health care.Citation36
For each simulation, inputs were randomly selected from their statistical distributions, and pairs of data points for costs and effectiveness for each treatment were obtained. At the end of the simulation process, the joint statistical distribution for costs and effectiveness was represented as a cloud of points on a cost-effectiveness plane. Cost-effectiveness acceptability curves were generated, representing the probability of each treatment being the most cost-effective for a range of cost-effectiveness thresholds.
Budget impact
Analytical framework
In a linked model, budget impact was assessed using a COPD patient-level model approach in Microsoft Excel. A Dutch health care payer’s perspective was adopted. Treatment-specific lung function improvements after 2 weeks were applied to baseline FEV1 distributions as found in the Netherlands and tracked over 5 years assuming a fixed 30 mL annual decline. Calculations were performed for an incident and a prevalent cohort, including only direct health care costs (). Given that health insurance bodies work with yearly budgets, budget impact was calculated per year with a maximum time horizon of 5 years. All inputs and assumptions were similar to the cost-effectiveness model. Costs are provided in their undiscounted form and no mortality was assumed.
Size of the eligible population
The COPD incidence and prevalence were based on the Dutch national data sources.Citation37 The GOLD distributions for the incidentCitation38 and prevalentCitation39 COPD population were based on the Dutch and, in case of absent Dutch data, international population estimates.
Current mix of treatments and alternative scenarios
Medication distributions over 5 years were based on the manufacturer’s projections of market share within a group of (combined) bronchodilators, including tiotropium, indacaterol–glycopyrronium, umeclidinium–vilanterol, aclidinium–formoterol, tiotropium–salmeterol (separate inhalers), vilanterol–fluticasone furoate (Table S6). Scenarios with and without tiotropium–olodaterol FDC over 1, 2, 3, 4, and 5 years, respectively were compared. Costs of these treatments were based on the Dutch costs prices (www.medicijnkosten.nl).
Uncertainty and scenario analyses
To account for lower medication uptake as seen in real-life practice, shown in the Dutch national adherence monitor,Citation40 scenarios with different extents of medication adherence were assessed, including scenarios with 40%, 60%, 80%, and 100% medication adherence.
Results
Cost-effectiveness
Base-case analyses, using our best estimates for each input variable, were performed first. In , the per-patient results of the base-case cost-effectiveness analysis are shown, based on the 15-year time horizon. Patients on tiotropium–olodaterol FDC gained 8.38 QALYs at an expense of €32,423. Patients on tiotropium gained 8.31 QALYs at an expense of €31,989.
Table 2 Cost-effectiveness results for the Netherlands (15-year time horizon)
Taking into account discounting over this 15-year time horizon, an ICER of €7,004/QALY results; without discounting the ICER is €5,981/QALY.
In , the clinical outcomes are shown. Over a 15-year time horizon, treatment with tiotropium–olodaterol FDC resulted in slightly better clinical outcomes including life-years gained and prevented exacerbations of all types. Annually, treatment with tiotropium–olodaterol FDC resulted in the prevention of 0.035 exacerbations (0.03 severe and 0.006 nonsevere) per patient.
Table 3 Clinical outcomes
Sensitivity analyses
In , univariate sensitivity analyses are shown for extreme values of the model. Results seem robust in several sensitivity analyses.
Table 4 Sensitivity analyses
In , the PSA is shown. Treatment with tiotropium–olodaterol, as well as tiotropium alone, resulted in both cost increases and QALY gains, although differences were marginal. Additionally, a cost-effectiveness acceptability curve was constructed ().
Figure 1 Probabilistic sensitivity analysis (100 iterations).
Abbreviations: QALYs, quality-adjusted life-year; Tio, Tiotropium; Olo, Olodaterol.
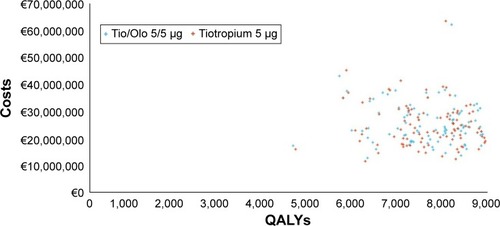
Figure 2 Cost-effectiveness acceptability curves.
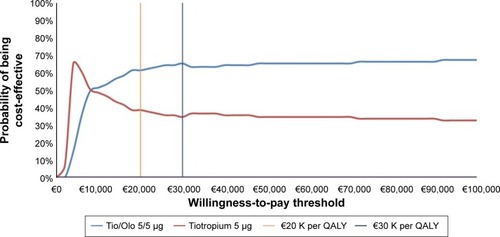
As shown, tiotropium–olodaterol FDC is cost-effective at the lowest – so far – suggested Dutch cost-effectiveness threshold of €20,000.Citation41 The probability of being cost-effective at that threshold is 61.4%. The probability would slightly increase to 65.3% at higher thresholds such as at €30,000,Citation22 but remains stable despite higher thresholds.
Budget impact
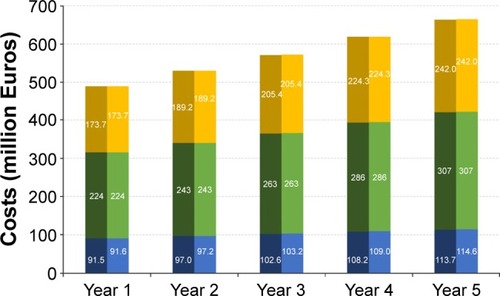
In , the total yearly national Dutch costs of COPD treatment over a time horizon up to 5 years is presented for a scenario without (left part of each column) and with (right part of each column) tiotropium–olodaterol, assuming 60% medication adherence. Mainly due to expected rise in number of COPD patients, total COPD costs are increasing from €489.1 million without tiotropium–olodaterol (€489.2 with) in 2015 to €663.2 without tiotropium–olodaterol (€664.1 with) million in 2019. As shown, introducing tiotropium–olodaterol will be responsible for less than 1% of the total increase in COPD expenses.
Figure 3 Total Dutch COPD health care costs with and without tiotropium–olodaterol FDC (in million Euros).
Abbreviations: COPD, chronic obstructive pulmonary disease; FDC, fixed-dose dual bronchodilator combination.
In , the incremental budget impact of introducing tiotropium–olodaterol FDC over a time horizon of 5 years is presented. Due to expected rise in number of COPD patients and increased market share projections (ranging from 0.6% of COPD patients that require long-acting bronchodilators on tiotropium–olodaterol in year 1 to 7.7% in year 5, see Table S4), incremental costs are increasing from €55,288 in 2015 to €877,641 in 2019 (summing up to €2.6 million over 5 years).
Figure 4 Budget impact of introducing tiotropium–olodaterol FDC (in million Euros).
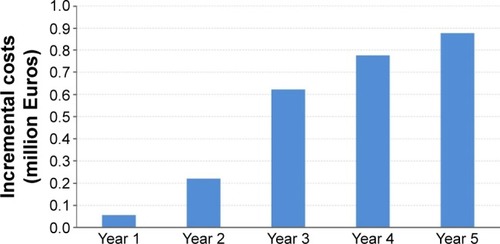
Scenarios with 40%, 80%, and 100% medication adherence resulted in lower or higher 5-year incremental cost increases of €1.7, €3.4, and €4.3 million, respectively.
Discussion
As a result of cost increases, combined with QALY gains, results showed that tiotropium–olodaterol FDC had an ICER of €7,004 per QALY. Without discounting, the ICER was €5,981 per QALY. Results were robust in univariate and probabilistic sensitivity analyses. Budget impact was estimated at €2.6 million over 5 years, assuming 60% adherence. Scenarios with 40%, 80%, and 100% adherence resulted in lower or higher 5-year incremental cost increases of €1.7, €3.4, and €4.3 million, respectively.
In a previous study, the cost-effectiveness of the mono-component tiotropium was favorable.Citation12 In addition, a more recent economic evaluation of another fixed-dose LABA–LAMA (umeclidinium–vilanterol), with tiotropium as comparator, concluded that the new treatment was considered cost-effective in the Spanish setting with an estimated ICER of €21,475.Citation22 This ICER was higher than in our study, but note that a shorter time horizon of 3 years was used and indeed shorter time horizons may not capture the full economic benefits, as shown in our sensitivity analyses. In a cost-effectiveness analysis of another dual bronchodilator, indacaterol–glycopyrronium FDC was not compared with tiotropium, but with both its mono-components and with salmeterol–fluticasone, and was found cost-saving in the Swedish health care setting.Citation42 Yet, due to the choice of these different comparators, which may not be considered usual care, and the inclusion of pneumonia as side effect of ICS use, results are not directly comparable to our study.
In 2007, the Dutch report of the National Institute of Public Health (RIVM)Citation43 reported that €415 million was spent on COPD treatment and 36% comprised medication. The estimated total burden of COPD in our model was €550 million in 2014 and 28% comprised medication. Hence, our burden estimate was slightly higher, while the part due to medication was somewhat lower. Differences in total expenses are likely due to methodological differences and the year of calculation. Indeed, the RIVM expects an increase in number of COPD patients from about 350,000 currently to 600,000 in 2032 and then our expenses are in line with future projections.Citation43 In addition, RIVM calculations were based on prescription data, while up to 10%–15% of respiratory medication was actually never dispensed.Citation44 Notably, when real-world medication adherence measures were applied in our study, medication expenses were considerably lower. The assumption of 60% adherence is well in line with adherence reported in Dutch national data over the period 2007–2014 (60%–64%),Citation40 confirming the validity of our base-case budget impact assumption on adherence.
This is the first full economic evaluation of tiotropium–olodaterol FDC for the Netherlands. It is based on the best currently available evidence, a validated model, and includes extensive uncertainty analyses. In addition, exacerbation risk, a main cost driver, was calculated using a real-life approach. While some previously published models in COPD have estimated the risk of both severe and moderate exacerbations by treatment as well as by GOLD stage,Citation29,Citation45 other economic evaluations have estimated overall exacerbation risk by treatment onlyCitation46 or estimated the proportion of severe to nonsevere exacerbations by GOLD stage.Citation47 These approaches have limitations in that the probability of exacerbations is not affected by having experienced a previous exacerbation, while a history of exacerbations has been shown to be the most reliable predictor for future exacerbations.Citation19,Citation23 Yet, some potential limitations have to be noted. In the cost-effectiveness analyses, adverse events from bronchodilators were not incorporated, although these side effects are considered of only minor importance and likely to be equally prevalent among comparators. In addition, differential rates of treatment switch or add-on treatments were not considered; however, these were assumed equally plausible. The same goes for the extent of treatment discontinuation. Finally, relatively long-term projections of 15 years are naturally surrounded by uncertainty regarding new treatments and health care policies.
Based on current Dutch thresholds, the cost-effectiveness ratio of tiotropium–olodaterol FDC in the Netherlands is generally favorable. However, other factors than solely cost-effectiveness ratios may play a role in recommendations regarding reimbursement and implementation in clinical guidelines. From a clinical perspective, one should take into account that once-daily therapies are associated with increased adherenceCitation48,Citation49 and that nonadherence to COPD medication is associated with decreased clinical and economic outcomes.Citation50 Moreover, when two inhaled drugs are indicated, the use of a single inhaler is recommended in order to avoid confusion and inhalation technique errors.Citation51 In choosing the optimal inhaler, patient’s needs and preferences should not be overlooked.
Regarding future research, it is recommended to assess the effectiveness and cost-effectiveness of tiotropium–olodaterol and other FDC LAMA–LABAs in real-life studies, including their effects on patient-reported outcomes.
Conclusion
Tiotropium–olodaterol FDC can be considered a cost-effective treatment under currently suggested Dutch cost-effectiveness thresholds.
Disclosure
This study was funded by Boehringer Ingelheim. The institutions of JVB, JWK, and MJP (University of Groningen) has received research grants from Boehringer Ingelheim, AstraZeneca, GlaxoSmithKline, and Novartis, all manufacturers of respiratory drugs. JVB received consultancy fees from AstraZeneca and travel support from the Respiratory Effectiveness Group and the European COPD Coalition. JWK received several research grants and has been paid for consultancy services by AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Novartis. MJP received grants and honoraria from various pharmaceutical companies, including those developing, producing, and marketing COPD drugs. The authors report no other conflicts of interest in this work.
References
- Global strategy for the diagnosis, management and prevention of COPD, Global Initiative for chronic Obstructive Lung Disease (GOLD)2015 Available from: http://www.goldcopd.org/Accessed December 22, 2015
- MurrayCJLopezADAlternative projections of mortality and disability by cause 1990–2020: global burden of disease studyLancet19973499064149815049167458
- van GemertFKirengaBChavannesNPrevalence of chronic obstructive pulmonary disease and associated risk factors in Uganda (FRESH AIR Uganda): a prospective cross-sectional observational studyLancet Glob Health201531e44e5125539969
- DalePRCerneckaHSchmidtMThe pharmacological rationale for combining muscarinic receptor antagonists and beta-adrenoceptor agonists in the treatment of airway and bladder diseaseCurr Opin Pharmacol201416314224682092
- ZuWallackRAllenLHernandezGTingNAbrahamsREfficacy and safety of combining olodaterol Respimat((R)) and tiotropium HandiHaler((R)) in patients with COPD: results of two randomized, double-blind, active-controlled studiesInt J Chron Obstruct Pulmon Dis201491133114425342898
- BarnesPJInhaled corticosteroids in COPD: a controversyRespiration2010802899520501985
- NanniniLJLassersonTJPoolePCombined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary diseaseCochrane Database Syst Rev20129CD00682922972099
- van BovenJFde Jong-van den BergLTVegterSInhaled corticosteroids and the occurrence of oral candidiasis: a prescription sequence symmetry analysisDrug Saf201336423123623516006
- PriceDYawnBBrusselleGRossiARisk-to-benefit ratio of inhaled corticosteroids in patients with COPDPrim Care Respir J20132219210023135217
- MagnussenHDisseBRodriguez-RoisinRWithdrawal of inhaled glucocorticoids and exacerbations of COPDN Engl J Med2014371141285129425196117
- DecramerMCelliBKestenSLystigTMehraSTashkinDPUPLIFT investigatorsEffect of tiotropium on outcomes in patients with moderate chronic obstructive pulmonary disease (UPLIFT): a prespecified subgroup analysis of a randomised controlled trialLancet200937496961171117819716598
- HoogendoornMAlMJBeehKMCost-effectiveness of tiotropium versus salmeterol: the POET-COPD trialEur Respir J201341355656422700844
- VogelmeierCHedererBGlaabTPOET-COPD InvestigatorsTiotropium versus salmeterol for the prevention of exacerbations of COPDN Engl J Med2011364121093110321428765
- KochAPizzichiniEHamiltonALung function efficacy and symptomatic benefit of olodaterol once daily delivered via Respimat(R) versus placebo and formoterol twice daily in patients with GOLD 2–4 COPD: results from two replicate 48-week studiesInt J Chron Obstruct Pulmon Dis2014969771425045258
- FergusonGTFeldmanGJHofbauerPEfficacy and safety of olodaterol once daily delivered via Respimat(R) in patients with GOLD 2–4 COPD: results from two replicate 48-week studiesInt J Chron Obstruct Pulmon Dis2014962964524966672
- BuhlRMaltaisFAbrahamsRTiotropium and olodaterol fixed-dose combination versus mono-components in COPD (GOLD 2–4)Eur Respir J201545496997925573406
- SauerRHanselMBuhlRRubinRAFreyMGlaabTImpact of tiotropium + olodaterol on physical functioning in COPD: results of an open-label observational studyInt J Chron Obstruct Pulmon Dis20161189189827217742
- SinghDFergusonGTBolitschekJTiotropium + olodaterol shows clinically meaningful improvements in quality of lifeRespir Med2015109101312131926320402
- Selya-HammerCGonzalez-Rojas GuixNBaldwinMDevelopment of an enhanced health-economic model and cost-effectiveness analysis of tiotropium + olodaterol Respimat® fixed-dose combination for chronic obstructive pulmonary disease patients in ItalyTher Adv Respir Dis Epub2016712
- HurstJRVestboJAnzuetoASusceptibility to exacerbation in chronic obstructive pulmonary diseaseN Engl J Med2010363121128113820843247
- van BovenJFVegterSvan der MolenTPostmaMJCOPD in the working age population: the economic impact on both patients and governmentCOPD201310662963923845002
- GeijerRMTuutMKin’t VeenJCBroekhuizenBDChavannesNHSmeeleIJThe NHG guidelines “Adult asthma” and “COPD”Ned Tijdschr Geneeskd2015159A907625990339
- MiravitllesMGaldizJBHuertaAVillacampaACarcedoDGarcia-RioFCost-effectiveness of combination therapy umeclidinium/vilanterol versus tiotropium in symptomatic COPD Spanish patientsInt J Chron Obstruct Pulmon Dis20161112313226848262
- DonaldsonGCWedzichaJACOPD exacerbations. 1. EpidemiologyThorax200661216416816443707
- TashkinDPLiNHalpinDAnnual rates of change in pre-vs. post-bronchodilator FEV1 and FVC over 4 years in moderate to very severe COPDRespir Med2013107121904191123972968
- TashkinDPVariations in FEV(1) decline over time in chronic obstructive pulmonary disease and its implicationsCurr Opin Pulm Med201319211612423287286
- WiseRAAnzuetoACalverleyPThe Tiotropium Safety and Performance in Respimat Trial (TIOSPIR), a large scale, randomized, controlled, parallel-group trial-design and rationaleRespir Res2013144023547660
- WiseRAAnzuetoACottonDTiotropium Respimat inhaler and the risk of death in COPDN Engl J Med2013369161491150123992515
- van BovenJFTommeleinEBousseryKImproving inhaler adherence in patients with chronic obstructive pulmonary disease: a cost-effectiveness analysisRespir Res2014156624929799
- Rutten-van MolkenMPOostenbrinkJBMiravitllesMMonzBUModelling the 5-year cost effectiveness of tiotropium, salmeterol and ipratropium for the treatment of chronic obstructive pulmonary disease in SpainEur J Health Econ20078212313517370096
- Rutten-van MolkenMPOostenbrinkJBTashkinDPBurkhartDMonzBUDoes quality of life of COPD patients as measured by the generic EuroQol five-dimension questionnaire differentiate between COPD severity stages?Chest200613041117112817035446
- SpencerSJonesPWGLOBE Study GroupTime course of recovery of health status following an infective exacerbation of chronic bronchitisThorax200358758959312832673
- PatersonCLanganCEMcKaigGAAssessing patient outcomes in acute exacerbations of chronic bronchitis: the measure your medical outcome profile (MYMOP), medical outcomes study 6-item general health survey (MOS-6A) and EuroQol (EQ-5D)Qual Life Res20009552152711190007
- Health Care Insurance BoardDutch Pharmacoeconomic Guidelines [in Dutch] Available from: http://www.zorginstituutnederland.nl/binaries/content/documents/zinl-www/documenten/publicaties/publications-in-english/2006/0604-guidelines-for-pharmacoeconomic-research/0604-guidelines-for-pharmacoeconomic-research/Guidelines+for+pharmacoeconomic+research.pdfAccessed July 24, 2015
- Costa-ScharplatzMStallbergBGoyalPAsukaiYGruenbergerJBPriceDCost-effectiveness of glycopyrronium bromide compared with tiotropium in patients with chronic obstructive pulmonary disease in SwedenAppl Health Econ Health Policy201513663764526324401
- BriggsAHClaxtonKSculpherMJDecision Modelling for Health Economic EvaluationNew YorkOxford University Press2006
- Dutch National Health Compass Available from: http://www.natio-naalkompas.nl/object_binary/o20019_RP-COPD-2013.xls Accessed February 22, 2016
- MinasMHatzoglouCKaretsiECOPD prevalence and the differences between newly and previously diagnosed COPD patients in a spirometry programPrim Care Respir J201019436337020532466
- HoogendoornMFeenstraTLSchermerTRHesselinkAERutten-van MolkenMPSeverity distribution of chronic obstructive pulmonary disease (COPD) in Dutch general practiceRespir Med20061001838615894477
- Dutch medication adherence monitor Available from: http://www.therapietrouwmonitor.nl/cijfers/astmacopd-7Accessed January 26, 2016
- AtthobariJAsselbergsFWBoersmaCCost-effectiveness of screening for albuminuria with subsequent fosinopril treatment to prevent cardiovascular events: A pharmacoeconomic analysis linked to the prevention of renal and vascular endstage disease (PREVEND) study and the prevention of renal and vascular endstage disease intervention trial (PREVEND IT)Clin Ther200628343244416750458
- PriceDKeiningerDCosta-ScharplatzMCost-effectiveness of the LABA/LAMA dual bronchodilator indacaterol/glycopyrronium in a Swedish healthcare settingRespir Med2014108121786179325307414
- SuijkerbuijkAWde WitGAWijgaAHSocietal costs of asthma, COPD and respiratory allergyNed Tijdschr Geneeskd201315746A656224220178
- EkedahlAManssonNUnclaimed prescriptions after automated prescription transmittals to pharmaciesPharm World Sci2004261263115018256
- OostenbrinkJBRutten-van MolkenMPMonzBUFitzGeraldJMProbabilistic Markov model to assess the cost-effectiveness of bronchodilator therapy in COPD patients in different countriesValue Health200581324615841892
- PriceDGrayAGaleRCost-utility analysis of indacaterol in Germany: a once-daily maintenance bronchodilator for patients with COPDRespir Med2011105111635164721764277
- PriceDAsukaiYAnanthapavanJMalcolmBRadwanAKeyzorIA UK-based cost-utility analysis of indacaterol, a once-daily maintenance bronchodilator for patients with COPD, using real world evidence on resource useAppl Health Econ Health Policy201311325927423529714
- ClaxtonAJCramerJPierceCA systematic review of the associations between dose regimens and medication complianceClin Ther20012381296131011558866
- ToyELBeaulieuNUMcHaleJMTreatment of COPD: relationships between daily dosing frequency, adherence, resource use, and costsRespir Med2011105343544120880687
- van BovenJFChavannesNHvan der MolenTRutten-van MolkenMPPostmaMJVegterSClinical and economic impact of non-adherence in COPD: a systematic reviewRespir Med2014108110311324070566
- van der PalenJKleinJJvan HerwaardenCLZielhuisGASeydelERMultiple inhalers confuse asthma patientsEur Respir J19991451034103710596686
- HettleRWoutersHAyresJCost-utility analysis of tiotropium versus usual care in patients with COPD in the UK and BelgiumRespir Med2012106121722173323040833