
Abstract
Background
Hospitalization is common for acute exacerbation of COPD, but little is known about its impact on the mental health of caregivers.
Objective
The aim of this study was to determine the rates and predictors of depressive symptoms in caregivers at the time of hospitalization for acute exacerbation of COPD and to identify the probability and predictors of subsequent changes in depressive status 3 months after discharge.
Materials and methods
This was a prospective study. Depression symptoms were measured in 87 caregivers of patients hospitalized for exacerbation at hospitalization and 3 months after discharge. We measured factors from four domains: context of care, caregiving demands, caregiver resources, and patient characteristics. Univariate and multivariate multiple logistic regressions were used to determine the predictors of depression at hospitalization and subsequent changes at 3 months.
Results
A total of 45 caregivers reported depression at the time of hospitalization. After multiple adjustments, spousal relationship, dyspnea, and severe airflow limitation were the strongest independent predictors of depression at hospitalization. Of these 45 caregivers, 40% had a remission of their depression 3 months after discharge. In contrast, 16.7% of caregivers who were not depressive at hospitalization became depressive at 3 months. Caregivers caring >20 hours per week for patients with dependencies had decreased odds of remission, and patients having dependencies after discharge increased the odds of caregivers becoming depressed.
Conclusion
Depressive symptoms are common among caregivers when patients are hospitalized for exacerbation of COPD. Although illness factors are determinants of depression at hospitalization, patient dependence determines fluctuations in the depressive status of caregivers.
Introduction
COPD is a common, preventable and treatable disease that is characterized by peristent respiratory symptoms and airflow limitation. Periods of disease stability are punctuated by acute exacerbations, which often require medical intervention and hospitalization.Citation1 Treatment is aimed at promoting self-management and providing supportive care.Citation2 Most individuals with COPD live in a community in which relatives and friends are the main providers of care for disease management.Citation3 Unfortunately, caregiving can often have serious adverse health and personal consequences for caregivers. Depressive symptoms are commonly reported by caregivers of patients with COPD,Citation4–Citation6 with a frequency similar to that of depressive symptoms among caregivers of patients with mental illness or cancer.Citation4
Previous studies have shown that the patient’s level of dependence and perceived burden are very strong determinants of depression for caregivers of patients with COPD.Citation4,Citation6 Qualitative studies have reported that the occurrence of exacerbations and whether the patient will recover from them are distressing situations for caregivers.Citation7 However, the role of exacerbations in the development of new episodes of depression is not well understood. Also, little is known about how depression persists or remits after hospitalization for acute exacerbation of COPD and factors that may predict remission from depression. Although the existing literature provides some insight into the characteristics of caregivers likely to have depression in the community,Citation4,Citation6,Citation8 factors associated with the occurrence of depression at the time of hospitalization or with its remission after hospitalization could differ.
The present study addressed these questions in a cohort of caregivers of patients hospitalized for exacerbation of COPD. The objectives were to determine the rates and predictors of depressive symptoms at the time of hospitalization for exacerbation of COPD and to identify the probability and predictors of subsequent changes in the caregiver’s depressive status 3 months after discharge.
Materials and methods
Study design and participants
Caregivers of patients hospitalized for exacerbation of their COPD were prospectively recruited at Morales Meseguer Hospital, Murcia, Spain. Participants were included if they were the primary caregiver (ie, the person who, before hospitalization, provided the most physical and/or supportive care without receiving any payment) and 18 years of age or older. Potential participants were excluded if they or their patients had significant cognitive deficits (ie, Mini-Mental State Examination Score of <20), or if patients were younger than 40 years old, had a terminal illness (survival expected to be <4 months), lived outside the hospital’s catchment area, or had a length of stay of >30 days.
On the basis of patient health examinations and a review of the patients’ electronic files, a pulmonary physician identified and recruited a consecutive sample of eligible caregivers during a 1-year period. All study participants provided written informed consent, and the study protocol was approved by The Institutional Review Board of the Morales Meseguer Hospital (EST-35/13).
Measures
Data were collected in face-to-face interviews separately with caregivers and their patients 48–96 hours after hospital admission and in phone interviews 3 months after hospital discharge. Patients were interviewed for measuring potential predictor variables (eg, dyspnea, frailty, and level of dependence). When patients were unable to be interviewed or contacted at home, the primary caregiver was interviewed as a surrogate because they may also provide accurate information.
We used the depression subscale of the Goldberg test to highlight the presence or absence of depressive symptoms.Citation9,Citation10 This scale includes nine items that ask respondents to rate the presence of symptoms using binary response categories (yes/no). Scores range from 0 to 9, and a cutoff of 2 is used to discriminate patients with depressive symptoms (≥2) from those without symptoms (<2).Citation9 This instrument was administered at the hospital at admission and at home 3 months after discharge.
Potential predictor variables
Variables were chosen based on their potential association with depression as indicated throughout the literature and conceptual framework.Citation6,Citation11 These variables were classified into four domains that may contribute to depression: context of care, caregiving demands, caregiver resources, and patient characteristics.
The context of care included the caregiver’s age and gender, cohabitation (yes/no), and kin relationship (spouse-partner/other) with the patient. Caregiving demands were related to the caregiving period (months), hours per week, and caregiver’s burden. Caregiving period and hours per week were measured at the hospital regarding the patient’s pre-exacerbation status and dichotomized as described elsewhere.Citation5,Citation6 Burden was measured at the hospital and again 3 months after discharge by the Zarit Caregiver Burden Interview (ZBI),Citation12 which has already been used to measure caregiver burden of patients with COPD.Citation13 The ZBI included 22 items using a 5-point response scale ranging from “never” to “almost always”. Its summative score was categorized into low, moderate, or high burden.
Caregiver resources were help from another caregiver (yes/no) and perceived social support. The latter was measured by the Duke UNC questionnaire, which includes 11 items for measuring two subscales: affective (receiving tokens of affection) and confidential (having someone to discuss concerns) support. These items asked respondents to indicate how they felt using a 5-point response scale ranging from “much less than what I want” to “much as I want”. A summative score was obtained per subscale and categorized as scarce or normal support.Citation14,Citation15
Patient characteristics included airflow limitation, the modified Medical Research Council Dyspnea Scale, frailty, and level of dependence. Airflow limitation was extracted from electronic files on the patient’s last control visit for COPD before hospitalization. Frailty was measured at the hospital by means of the Reported Edmonton Frail Scale based on a scale from 0 to 18, where higher scores indicate more severe frailty.Citation16 Dyspnea and dependence were measured at the hospital and again 3 months after discharge. Dependence was measured by a scale of six activities of daily living (ADLs: toileting, bathing, transferring, eating, dressing, and walking across a small room) as described elsewhere.Citation17 Dependence was defined as self-reporting being unable to perform an ADL or requiring the help of another person for any ADL. The score range for this scale (0–6) was based on the number of dependencies, with a score of 6 representing dependencies in all ADLs.
Statistical analysis
We used descriptive statistics, including Pearson χ2 and independent t-tests, to summarize variables regarding the four domains between caregivers with and without depressive symptoms. Multivariate logistic regression analyses were used to assess the possible factors associated with depression at baseline. Separate multivariate models were fit for each of the four domains by including all their variables as independent variables. A final multivariate logistic regression model was chosen by including the most strongly predictive factors from each of the individual models, as well as variables significant at the 0.10 level. All multivariate models were produced using the back-step method. Goodness-of-fit and regression diagnostics were assessed as described elsewhere.Citation18
Caregivers who had depressive symptoms at baseline and did not have symptoms at the end of study were classified as having remission (yes/no). Caregivers who were depression-free at the hospital and became depressive were classified as having a new episode of depression (yes/no).
Univariate and multivariate logistic regression analyses were used to assess the possible factors associated with both having remission and a new episode after hospital discharge, which were used as dependent variables. In the univariate analyses, all potential predictors were tested for a significant relationship (P<0.10). Two multivariable analyses were then performed using the relative factors with significant contributions (P<0.10) in the univariate analyses. All univariate models used the enter method, and the multivariate models were produced using the back-step method. Goodness-of-fit and regression diagnostics for the models were assessed as described elsewhere.Citation19
The sample size calculation was based on the rule of thumb that 15 subjects are needed per predictor for a reliable equation.Citation19 We recruited a minimum of 75 participants assuming a maximum of five predictors. All analyses were performed using the Statistical Package for the Social Sciences (SPSS) statistical software program (SPSS version 19.0; IBM SPSS, Chicago, IL, USA).
Results
A total of 107 patients were hospitalized for acute exacerbation of COPD during the study period. Of these patients, 90 reported having a usual caregiver at home. All caregivers agreed to participate in the study, but three were excluded because their patients had a length of stay longer than 30 days. Therefore, 87 caregivers were finally included at baseline. Eighty-four of the caregivers participated again 3 months after hospital discharge. Of the three caregivers lost to follow-up, two died and one dropped out of the study because the patient died.
Forty-five caregivers of patients (51.7%) in our sample reported depressive symptoms at baseline. Data on the context and demands of care, caregiver resources, and patient characteristics are provided in for caregivers with and without depression. A higher percentage of caregivers with depressive symptoms had a moderate-to-high level of perceived burden and scarce levels of social support compared to those without symptoms.
Table 1 Baseline characteristics of caregivers with and without depressive symptoms
The results of the multivariate models of predictors of caregiver depression at the time of hospitalization for COPD are shown in . Model 1, which included context of care, suggests that spousal caregiving may be associated with higher odds of caregiver depression. The model of caregiving demands (Model 2) suggested that a moderate and high burden of care is associated with greater odds of caregiver depression. Model 3 examined caregiver resources but did not identify any relevant factor. More relevant Patient characteristics (Model 4) were severity of airflow limitation and dyspnea. In the final model, spousal caregiving, having dyspnea, and severe airflow limitation were the strongest independent predictors of caregiver depression at the time of hospitalization of COPD.
Table 2 Predictors of caregiver depression during hospitalization of their patients
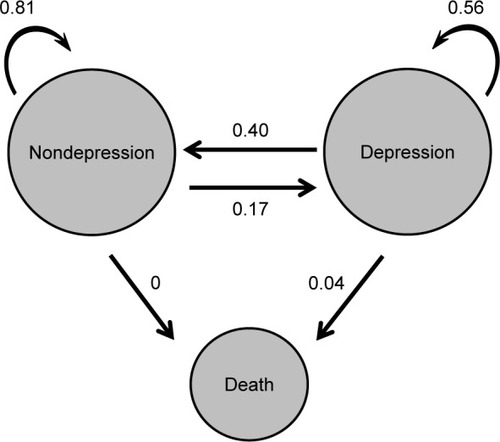
shows the probability of change between the states of depression, nondepression, and death 3 months after hospital discharge. The arrows represent the likelihood that a subject who started depressed or not depressed remains in that state or changes to another state 3 months later. Of the 45 caregivers who reported depression at hospitalization, 18 (40%) were depression-free 3 months after hospital discharge, 25 (55.6%) continued to report depressive symptoms, and 2 (4.4%) died. In contrast, 34 (80.9%) of the caregivers who were not depressed at hospitalization remained depression-free at 3 months, 7 (16.7%) became depressive, and 1 (2.3%) dropped out. At 3 months, a total of 32 caregivers (38% of the 84 participants) had depression.
Figure 1 Probabilities of change between the states of depression, nondepression, and death.
The results of multivariate models for predictors of remission and new episodes of caregiver depression 3 months after hospital discharge are shown in . In the univariate logistic regression analyses (not shown), only the number of dependencies (P=0.06) and hours per week (P=0.01) were associated with remission (although the first was considered trend and not statistically significant), and only perceived burden (P=0.03) and number of dependencies (P=0.01) were associated with new episodes. According to the first multivariate model, providing care >20 hours per week and dependence at home in three or more daily activities decreased the odds of remission. In addition, the patient having this level of dependence at home increased the odds of the caregiver becoming depressed after hospital discharge. Perceived burden was excluded (P>0.10) from this model.
Table 3 Predictors of remission and new episodes of depression after hospital discharge
Discussion
Depression was very common among caregivers of COPD patients at the time of hospitalization for acute exacerbation, but the findings of the current study indicate that depressive symptoms often remit after discharge. However, our results also showed that some caregivers who originally reported being depression-free had depression 3 months after the patients they care for were discharged from the hospital. The percentage of caregivers with depressive symptoms after 3 months at home was consistent with previous studies of caregivers of patients with stable COPDCitation5,Citation6 and other chronic conditions.Citation20
Spousal caregiving, dyspnea, and severity of airflow limitation were independent factors associated with caregiver depression at the time of hospitalization. The higher odds of depression for spouses/partners may indicate that acute exacerbations are very stressful for them.Citation7 In a previous meta-analysis of caregivers of patients with chronic diseases, researchers found that spouses have higher levels of depression and stress than other caregivers and noncaregivers.Citation21 The relevance of both dyspnea and severe/very severe COPD is also consistent with previous studies of caregivers of patients with COPD.Citation5,Citation6 These results were expected because, as the disease progresses, the burden and responsibilities also tend to increase (eg, monitoring breathlessness, medications, and oxygen therapy).Citation22 Illness factors associated with depressive symptoms at the time of hospitalization for acute exacerbation of COPD (severity and dyspnea) were not strong predictors of remission or new episodes of depression after hospital discharge. A possible reason for this finding could be the severity of disease being more stressful for caregivers during acute exacerbation than at home.
Our findings on patients’ dependence as a determinant of fluctuations in the depressive status of caregivers after hospital discharge are particularly important in light of the known relevance of hospitalization on the progression of disability.Citation23,Citation24
Limitations of this study
Our findings should be interpreted in light of our study’s methodological limitations. We compared caregivers’ depression status in two environments: hospital and home. Nevertheless, data were initially collected at the time of hospitalization and it was not possible to know the magnitude of the impact of the hospitalization on the caregivers’ depression. Longitudinal studies that assess depression and premorbid health status before hospitalization would be desirable. Depression status after hospital discharge was measured only once at 3 months, and it is likely that there were additional fluctuations between these time points. Moreover, it is possible that the recovery time may be longer; consequently, our results likely underestimate the recovery rates. Third, patients with survival expected to be <4 months may determine more depression in caregivers and their exclusion may bias the results. Our decision to exclude them was based on the fact that a 3-month follow-up was planned. Finally, because of the small number of men in the cohort, the results should be generalized to men with caution.
Implications for practice and research
To the best of our knowledge, this is the first study to provide evidence that the frequency of depression at home is substantially lower than at the time of hospitalization for exacerbation. This was an expected result because studies of other conditions have indicated that hospital admission is stressful for caregivers.Citation21 Although dependence to perform several ADLs was not associated with depression at hospitalization, it was the more relevant factor for fluctuations in depressive symptoms after hospital discharge. In our opinion, these two findings are not contradictory. Dependence is not a supplementary workload or source of distress for caregivers during hospitalization because their responsibilities are surrogated by staff assistance. In contrast, the patient being dependent after hospitalization is a more distressing situation for caregivers due to increasing care demands or sadness associated with the loss of independence by a family member. Identifying patients with severe dependence who could be targeted for rehabilitation programs prior to or after hospitalization could reduce the very high rates of depression in caregivers seen after hospitalization.
Conclusion
This study advances current knowledge on the presence of depressive symptoms among caregivers at the time of hospitalization for exacerbation of COPD and their related change 3 months after the patients they care for return home. Although depression is more common at hospitalization for caregivers who are the spouses of patients with severe illness, the perception of depressive symptoms is dynamic, and many caregivers will not experience depressive symptoms in the middle term. Caregivers are more likely to recover from depression when their patients have few dependencies after hospital discharge. Dependence after discharge is also a strong determinant of new episodes of depression among caregivers. Further research should address caregivers’ needs, especially regarding the effectiveness of supportive interventions for dependence and prevention of distress at the time of hospitalization.
Acknowledgments
The authors wish to thank the patients and personnel of the hospital unit for their cooperation during the course of this study. The study was supported by medical manager of AstraZeneca Pharmaceutical Spain, S.A. and Maite Pérez Hernández.
Disclosure
The authors report no conflicts of interest in this work.
References
- KoFWChanKPHuiDSAcute exacerbation of COPDRespirology20162171152116527028990
- ZwerinkMBrusse-KeizerMvan der ValkPDSelf-management for patients with chronic obstructive pulmonary diseaseCochrane Database Syst Rev20143CD002990
- CaressALLukerKAChalmersKISalmonMPA review of the information and support needs of family carers of patients with chronic obstructive pulmonary diseaseJ Clin Nurs200918447949119191997
- MiravitllesMPeña-LongobardoLMOliva-MorenoJHidalgo-VegaACaregivers’ burden in patients with COPDInt J Chron Obstruct Pulmon Dis20151034735625709429
- FigueiredoDGabrielRJácomeCCruzJMarquesACaring for relatives with chronic obstructive pulmonary disease: how does the disease severity impact on family carers?Aging Ment Health201418338539324053489
- JácomeCFigueiredoDGabrielRCruzJMarquesAPredicting anxiety and depression among family carers of people with chronic obstructive pulmonary diseaseInt Psychogeriatr20142671191119924621411
- GrantMCavanaghAYorkeJThe impact of caring for those with chronic obstructive pulmonary disease (COPD) on carers’ psychological well-being: a narrative reviewInt J Nurs Stud201249111459147122386988
- NakkenNJanssenDJvan den BogaartEHInformal caregivers of patients with COPD: home sweet home?Eur Respir Rev20152413749850426324811
- GoldbergDBridgesKDuncan-JonesPGraysonDDetecting anxiety and depression in general medical settingsBMJ198829766538978993140969
- MontónCPérez-EchevarríaMJCamposRGarcía CampayoJLoboAAnxiety scales and Goldberg’s depression: an efficient interview guide for the detection of psychologic distressAten Primaria19931263453498218816
- PearlinLIMullanJTSempleSJSkaffMMCaregiving and the stress process: an overview of concepts and their measuresGerontologist19903055835942276631
- ZaritSHToddPAZaritJMSubjective burden of husbands and wives as caregivers: a longitudinal studyGerontologist19862632602663721233
- GarloKO’LearyJRVan NessPHFriedTRBurden in caregivers of older adults with advanced illnessJ Am Geriatr Soc201058122315232221087225
- BroadheadWEGehlbachSHde GruyFVKaplanBHThe Duke-UNK Functional Social Support Questionnaire. Measurement of social support in family medicine patientsMed Care19882677097233393031
- Bellón SaameñoJADelgado SánchezALuna del CastilloJDLardelli ClaretPValidity and reliability of the Duke-UNC-11 questionnaire of functional social supportAten Primaria19961841531638962994
- HilmerSNPereraVMitchellSThe assessment of frailty in older people in acute careAustralas J Ageing200928418218819951339
- BoydCMRicksMFriedLPFunctional decline and recovery of activities of daily living in hospitalizated, disabled older women: the Women’s Health and Aging Study IJ Am Geriatr Soc200957101757176619694869
- HosmerDWLemeshowSApplied Logistic Regression2nd edHoboken, NJJohn Wiley & Sons2000
- TabachnickBGFidellLSUsing Multivariate Statistics6th edBoston, MAPearson Education2013
- GrovEKDahlAAMoumTFossåSDAnxiety, depression, and quality of life in caregivers of patients with cancer in late palliative phaseAnn Oncol20051671185119115849218
- PinquartMSorensenSDifferences between caregivers and non-caregivers in psychological health and physical health: a meta-analysisPsychol Aging200318225026712825775
- SimpsonACYoungJDonahueMRockerGA day at a time: caregiving on the edge in advanced COPDInt J Chron Obstruct Pulmon Dis20105114115120631814
- ConnorsAFJrDawsonNVThomasCOutcomes following acute exacerbation of severe chronic obstructive lung diseaseAm J Respir Crit Care Med19961544 Pt 19599678887592
- LenzEHPerkinsSCoronary artery bypass graft surgery patients and their family member caregivers: outcomes of a family-focused staged psychoeducational interventionAppl Nurs Res200013314215010960998