
Abstract
The high prevalence of COPD together with its high level of misdiagnosis and late diagnosis dictate the necessity for the development and implementation of clinical practice guidelines (CPGs) in order to improve the management of this disease. High-quality, evidence-based international CPGs need to be adapted to the particular situation of each country or region. A new version of the Russian Respiratory Society guidelines released at the end of 2016 was based on the proposal by Global Initiative for Obstructive Lung Disease but adapted to the characteristics of the Russian health system and included an algorithm of pharmacologic treatment of COPD. The proposed algorithm had to comply with the requirements of the Russian Ministry of Health to be included into the unified electronic rubricator, which required a balance between the level of information and the simplicity of the graphic design. This was achieved by: exclusion of the initial diagnostic process, grouping together the common pharmacologic and nonpharmacologic measures for all patients, and the decision not to use the letters A–D for simplicity and clarity. At all stages of the treatment algorithm, efficacy and safety have to be carefully assessed. Escalation and de-escalation is possible in the case of lack of or insufficient efficacy or safety issues. Bronchodilators should not be discontinued except in the case of significant side effects. At the same time, inhaled corticosteroid (ICS) withdrawal is not represented in the algorithm, because it was agreed that there is insufficient evidence to establish clear criteria for ICSs discontinuation. Finally, based on the Global Initiative for Obstructive Lung Disease statement, the proposed algorithm reflects and summarizes different approaches to the pharmacological treatment of COPD taking into account the reality of health care in the Russian Federation.
Introduction
COPD is an important health care problem due to its high prevalence and impact in terms of morbidity and mortality. A recent study conducted in 12 regions of the Russian Federation observed a prevalence of COPD of 15.3% related to the high rates of smoking in the Russian population.Citation1 In addition, other studies have demonstrated the magnitude of the misdiagnosis of COPD in Russia and the particular characteristics of the COPD patients in this country. In a study of more than 1,500 Russian COPD patients, 53% had a forced expiratory volume in one second (% predicted) below 50% and up to 51% were frequent exacerbators.Citation2 In a large survey in middle and Eastern Europe, the Russian patients with COPD were among those with the highest prevalence of frequent exacerbators.Citation3 The high prevalence of the disease, the high rates of misdiagnosis, and the level of severity of the patients attended in Russian centers indicate the need for the development and implementation of a national clinical practice guideline (CPG) to improve the management of this disease.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has published statements about the diagnosis and treatment of COPD;Citation4 similarly, international scientific societies such as the European Respiratory Society and the American Thoracic Society have produced high-quality, evidence-based CPG.Citation5 However, these GOLD recommendations need to be adapted to the particular situation of each country or region,Citation6 taking into account the characteristics of the patients, the health care system, and the availability of treatments.
Russian guidelines for the management of COPD
The first national Russian guidelines on the diagnosis and management of COPD were developed and published in 1999 and have been updated several times thereafter. The most important update was published in 2014, when the Ministry of Health (MOH) of the Russian Federation proposed a standardized model for the development of CPG for all specialties and diseases according to the “International Statistical Classification of Diseases and Related Health Problems.”Citation7 It was intended that CPGs had to become the key documents to determine different aspects of disease management, including legal and disability issues. The definition of a CPG by the Russian MOH was an “… evidence-based document representing physician activity in terms of diagnosis, treatment, rehabilitation and prophylaxis of the disease which helps to choose the right clinical decision.”Citation7
Russian guidelines may serve as an example of revolutionary approach to guidelines, closing the gap between professional societies and regulatory authorities.
The new attitude of the Russian MOH to guidelines was based on the understanding that CPGs could not effectively function as an independent isolated document of any professional society with no connection to the reality and complexity of real clinical practice and health care (which is regulated by the number of laws, by-laws, and subordinate acts) and not complying with other regulating documents.
Initially, the MOH built the conception that a CPG should be a major document regulating not only clinical practice but also expert evaluation of medical service quality and occupational disability. The electronic rubricator proposed by the MOH makes it possible to standardize guidelines in several terms (size, parts and sections, algorithms, etc.) and integrate these with all regulatory documents and other guidelines by cross-links and cross-references.
According to MOH definition, the unified electronic rubricator is a universally hierarchically structured integrated database for all CPG which is systematically updated. The unified electronic rubricator initially was designed to include all available approved guidelines in a single format and structure. According to MOH policy, before final placement of newly developed CPG into the unified electronic rubricator they need two-stage approval: by national professional society and MOH itself.
All parts and chapters are typed in by completing special prespecified forms which allow to keep the size and structure of the final document. Only documents complying with the structure, style, and other features can be placed into the rubricator. The whole database is equipped by search engine and cross-references.
The electronic rubricator also meant that the CPG must have a unified structure with the list of necessarily required and recommended sections. Among mandatory parts which seem to be important for COPD implementation in real life but which are not present in other available COPD guidelines are “COPD patient follow-up” and “criteria for evaluation of medical care quality.” In the first section, follow-up is specified according to severity and the level of the medical institution or health care provider (eg, 1st – local or 2nd – intermunicipal center) responsible for the follow-up of COPD patients with the number of visits per year and the list of examinations necessarily provided at any level in these medical institutions. In the medical care quality control section, evaluation criteria are listed for diagnostic and management procedures according to the severity of the disease and phase (stable condition or exacerbation).
Taking into account all these requirements and in concordance with them, an expert committee of the Russian Respiratory Society released a new version of the national COPD guidelines at the end of 2016.Citation8 This update was based on the proposal by GOLD but adapted to the characteristics of the Russian health system and included an algorithm of pharmacologic treatment following recently published algorithms for the treatment of COPD.Citation9–Citation11 We believe that this proposal will contribute to the debate of the optimal treatment algorithm that combines strong scientific evidence with the reality of clinical practice for the treatment of COPD.
Algorithm of pharmacologic treatment
The algorithm proposed had to comply with the requirements of the Russian MOH to be included in the electronic rubricator.Citation7 Therefore, a balance was sought between the level of information and the simplicity of the graphic design. First, the diagnostic process was excluded from the algorithm and it was assumed that patients already fulfilled the internationally accepted diagnostic criteria for COPD.Citation4 Second, although the decision tree included the characteristics proposed by GOLD – ie, evaluation of symptoms and risksCitation4 – it was decided not to use the letters A–D for simplicity and clarity. Third, an initial group of common pharmacologic and nonpharmacologic measures was excluded from the algorithm and placed before the decision tree, because these measures apply to all patients, irrespective of the level of symptoms or risk ().
Figure 1 Pharmacologic treatment of COPD.
Abbreviations: LTOT, long-term oxygen therapy; NIV, noninvasive ventilation; mMRC, modified Medical Research Council; CAT, COPD Assessment Test; LABA, long-acting beta-adrenergic; LAMA, long-acting antimuscarinic; ICS, inhaled corticosteroid; ACO, asthma–COPD overlap.
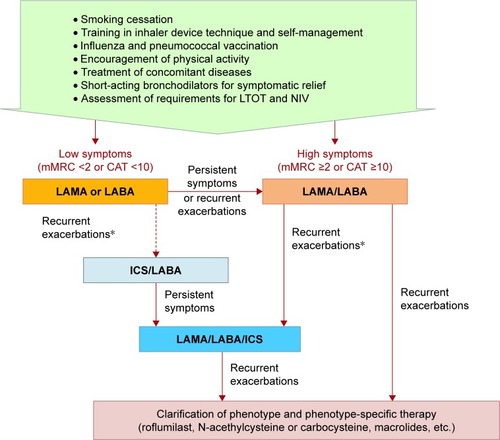
The treatment algorithm initiates with the evaluation of symptoms with the modified Medical Research Council dyspnea scale or COPD Assessment Test questionnaire, as suggested by GOLD, and using the same thresholds.Citation4 However, long-acting bronchodilators (instead of short-acting) are suggested as the preferred therapeutic option. This decision was based on the higher efficacy of long-acting drugsCitation12 and the possibility of underrecognition or underreporting of symptoms in patients with COPD.Citation13,Citation14
Although it is recognized that initial therapy with a long-acting antimuscarinic agent (LAMA) or long-acting β-2 agonist (LABA) is indicated in less symptomatic patients, the majority of COPD patients in Russia initially visit a doctor with a high level of symptoms and exercise intolerance.Citation2 In the case of high symptom level (modified Medical Research Council ≥2 or COPD Assessment Test >10 units), a combined LABA/LAMA is recommended after establishing the diagnosis of COPD. The LABA/LAMA combination is more effective than monotherapies in dyspnea relief, increasing exercise tolerance and improving patients’ quality of life.Citation15 LABA/LAMA is also the preferred option when patients on bronchodilator monotherapy have recurrent exacerbations due to the superiority of the LABA/LAMA versus long-acting bronchodilators in monotherapyCitation16 and especially versus the LABA/inhaled corticosteroid (ICS) combination in the prevention of exacerbations.Citation17
Combinations including ICS should not be used as first-line therapy in COPD. ICS as a component of a double (LABA/ICS) or triple (LAMA/LABA/ICS) therapy can be administered in situations when recurrent exacerbations occur during first-line therapy with long-acting bronchodilators and especially in patients who have concomitant asthma, based on internationally accepted criteria,Citation18 or eosinophilic inflammation.Citation4,Citation6,Citation9–Citation11,Citation19 However, there is no consensus yet on the threshold level of blood eosinophils, which predicts response to ICS in COPD.
In patients presenting recurrent exacerbations in spite of receiving LABA/LAMA or triple therapy, it is necessary to investigate the phenotype and consider the possibility of administering phenotype-specific therapy. This therapy may include roflumilast in the case of severe airflow limitation, chronic bronchitis, and previous hospitalization;Citation20 mucolytic agents particularly in chronic bronchitic patients with frequent exacerbations;Citation21 and/or macrolides in the case of frequent infective exacerbations,Citation22 especially in the presence of associated bronchiectasis.Citation4,Citation6,Citation9–Citation11
At all stages of treatment, the efficacy and safety have to be carefully assessed, and escalation and de-escalation is possible in the case of lack of or insufficient efficacy of safety issues. Since COPD is a progressive disease and bronchodilators are only effective during administration, they should not be discontinued except in the case of significant side effects. In contrast, there is evidence of excessive and inadequate use of ICS in COPD,Citation2,Citation3,Citation23 which may be associated with short- and long-term side effects. In fact, in a recent study conducted in Russia up to 19% of GOLD B patients were on LABA/ICS and 12% on triple therapy.Citation2 However, ICS withdrawal is not represented in the algorithm, because it was agreed by the panel that there is insufficient evidence to establish clear criteria as to when and how to discontinue ICS in patients with COPD.Citation24
Conclusion
Although based on the GOLD statement, the algorithm proposed reflects and summarizes different approaches to the pharmacological treatment of COPD. It is well recognized that long-acting bronchodilators are the bases of treatment, but the most severe patients require a more personalized approach taking into account their particular phenotype in order to select the most appropriate treatment that achieves the best balance between high efficacy and low risk of side effects. In addition, the treatment algorithm must be simple to permit implementation in the electronic clinical records, and it should be easy to remember and use by clinicians in order to reduce the gaps in the application of COPD-treatment recommendations.Citation25,Citation26
Disclosure
The authors report no conflicts of interest in this work.
References
- ChuchalinAGKhaltaevNAntonovNSChronic respiratory diseases and risk factors in 12 regions of the Russian FederationInt J Chron Obstruct Pulmon Dis2014996397425246783
- ArkhipovVArkhipovaDMiravitllesMLazarevAStukalinaECharacteristics of COPD patients according to GOLD classification and clinical phenotypes in the Russian federation: the SUPPORT trialInt J Chron Obstruct Pulmon Dis2017123255326229138554
- KoblizekVMilenkovicBBarczykAPhenotypes of COPD patients with a smoking history in Central and Eastern Europe: the POPE StudyEur Respir J201749160144628495687
- VogelmeierCFCrinerGJMartínezFJGlobal strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summaryArch Bronconeumol20175312814928274597
- WedzichaJCalverleyPAlbertRPrevention of COPD exacerbations: an European Respiratory Society/American Thoracic Society (ERS/ATS) guidelineEur Respir J201750160226528889106
- MiravitllesMVogelmeierCRocheNA review of national guidelines for management of COPD in EuropeEur Respir J20164762563726797035
- Russian Respiratory SocietyChronic obstructive pulmonary diseaseClinical guidelines Available from: http://www.spulmo.ru/obra-zovatelnyeresursy/federalnyeklinicheskierekomendatsiiAccessed August 18, 2017
- Ministry of Health of Russian FederationRequirements for the figuration of clinical recommendations for placement in the Rubricator Available from: http://nasci.ru/_resources/directory/196/common/Pismo_01.09.pdfAccessed August 18, 2017
- MiravitllesMSoler-CataluñaJJCalleMSpanish COPD guidelines (GesEPOC) 2017. Pharmacological treatment of stable chronic obstructive pulmonary diseaseArch Bronconeumol20175332433528477954
- ZykovKAOvcharenkoSIApproaches to drug therapy for COPD in Russia: a proposed therapeutic algorithmInt J Chron Obstruct Pulmon Dis2017121125113328442899
- MiravitllesMAnzuetoAA new two-step algorithm for the treatment of COPDEur Respir J201749160220028179443
- TashkinDPCooperCBThe role of long-acting bronchodilators in the management of stable COPDChest200412524925914718448
- MiravitllesMRiberaAUnderstanding the impact of symptoms on the burden of COPDRespir Res2017186728431503
- GruenbergerJBVietriJKeiningerDLMahlerDAGreater dyspnea is associated with lower health-related quality of life among European patients with COPDInt J Chron Obstruct Pulmon Dis20171293794428360517
- ThomasMHalpinDMiravitllesMWhen is dual bronchodilation indicated in COPD?Int J Chron Obst Pulm Dis20171222912305
- WedzichaJADecramerMFickerJHAnalysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomised, double-blind, parallel-group studyLancet Respir Med2013119920924429126
- WedzichaJABanerjiDChapmanKRIndacaterol–glycopyrronium versus salmeterol–fluticasone for COPDN Engl J Med20163742222223427181606
- 2017 GINA Report, Global Strategy for Asthma Management and Prevention Available from: http://ginasthma.org/2017-gina-report-global-strategy-for-asthma-management-and-prevention/Accessed November 18, 2017
- SinDDMiravitllesMManninoDMWhat is asthma-COPD overlap syndrome (ACOS)? Towards a consensus definition from a roundtable discussionEur Respir J20164866467327338195
- RabeKFCalverleyPMAMartinezFJFabbriLMEffect of roflumilast in patients with severe COPD and a history of hospitalisationEur Respir J201750170015828679611
- CazzolaMRoglianiPCalzettaLHananiaNAMateraMGImpact of mucolytic agents on COPD exacerbations: a pair-wise and network meta-analysisCOPD20171455256328753070
- UzunSDjaminRSKluytmansJAAzithromycin maintenance treatment in patients with frequent exacerbations of chronic obstructive pulmonary disease (COLUMBUS): a randomised, double-blind, placebo-controlled trialLancet Respir Med2014236136824746000
- BarrechegurenMMonteagudoMFerrerJTreatment patterns in COPD patients newly diagnosed in primary care. A population-based studyRespir Med2016111475326758585
- TariqSMThomasECMaintenance therapy in COPD: time to phase out ICS and switch to the new LAMA/LABA inhalers?Int J Chron Obstruct Pulmon Dis2017121877188228694698
- Calle RubioMAlcázar NavarreteBSorianoJBClinical audit of COPD in outpatient respiratory clinics in Spain: the EPOCONSUL studyInt J Chron Obstruct Pulmon Dis20171241742628182155
- DavisKJLandisSHOhYMContinuing to Confront COPD International Physician Survey: physician knowledge and application of COPD management guidelines in 12 countriesInt J Chron Obstruct Pulmon Dis201410395525565799