

Abstract
Purpose
DINO and DACOTA were prospective, noninterventional studies assessing the health status and quality of life of patients with COPD newly treated with roflumilast 500 μg once-daily add-on therapy.
Patients and methods
Patients were evaluated over 6 months. Clinical COPD questionnaire (CCQ) and COPD assessment test (CAT) scores were recorded at baseline and after 3 and 6 months. In DACOTA, post-bronchodilator FEV1 was recorded at each time point.
Results
Of 5,462 and 3,645 patients recruited into DINO and DACOTA, respectively, 3,274 patients in DINO and 916 patients in DACOTA completed the 6-month visit. Almost all patients had severe or very severe airway obstruction; mean baseline CCQ total score was 3.9 in DINO and 3.7 in DACOTA. Overall, 33.8% of patients in DACOTA and 30.6% in DINO discontinued treatment prematurely. Significant and clinically relevant improvements in CCQ total scores were observed in both studies (mean change from baseline of 1.36 in DINO and 0.91 in DACOTA at Month 6 [all P<0.001]). Changes in CAT total score from baseline to Month 6 indicated that the average clinical impact of COPD was reduced from a severe (score: 21–30) to a moderate (score: 11–20) impairment. In DACOTA, mean change in post-bronchodilator FEV1 was 202 mL (P<0.001). Diarrhea, nausea, and weight decrease were the most frequently reported adverse drug reactions.
Conclusion
In real-life clinical practice, roflumilast treatment as an add-on therapy is associated with clinically relevant improvements in health status and quality of life.
Supplementary materials
Effectiveness set criteria
In both DINO and DACOTA, the effectiveness set was defined as a population that was more compliant with the label and the study protocol and had complete data available for the assessment of the primary endpoint. The effectiveness set was based on patients in the treated set who met the following criteria:
Treatment with roflumilast for ≥5 months.
No simultaneous initiation of any other long-term (≥3 months) COPD-specific maintenance treatments/therapies; short-acting beta-agonists (SABA) and/or short-acting anticholinergic (SAMA) were allowed.
Post-bronchodilator FEV1<50% predicted.
Evaluable assessments of clinical COPD questionnaire at baseline and after 6 months.
No simultaneous initiation of short-term (≤14 days) treatment with oral corticosteroids, antibiotics, or theophylline.
Start date of roflumilast treatment not >7 days prior to Visit 1 (baseline; DACOTA only).
Figure S1 Patient disposition (treated sets) in (A) DINO and (B) DACOTA.
Notes: *Duration of roflumilast treatment <5 months, as reason for premature discontinuation, was not available as a check box in the CRF but was included for the purpose of the analysis. N=total number of patients. n=number of patients with an event.
Abbreviations: ADR, adverse drug reaction; CRF, case report form.
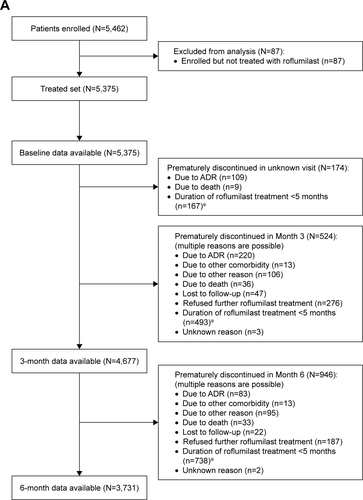
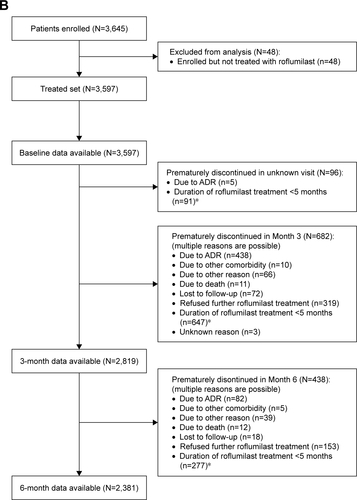
Figure S2 Change in CCQ total scores from baseline to Months 3 and 6 (treated sets) in the overall population (primary analysis), and in the frequent and nonfrequent exacerbator subgroups (post-hoc analysis) in (A) DINO and (B) DACOTA.
Notes: Data are mean ± standard error. n=number of patients with data available. All P<0.001 for the changes in CCQ total score from baseline to months 3 and 6.
*P<0.001 for exacerbation group comparisons.
Abbreviation: CCQ, clinical COPD questionnaire.
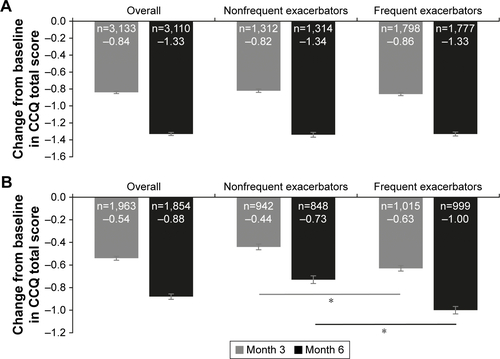
Figure S3 Change in CAT total scores from baseline to months 3 and 6 (treated sets) in the overall population (primary analysis), and in the nonfrequent and frequent exacerbator subgroups (post-hoc analysis) in (A) DINO and (B) DACOTA.
Notes: Data are mean ± standard error. All P<0.001 for the changes in CAT total score from baseline to Months 3 and 6.
*P<0.001 for exacerbation group comparisons.
Abbreviation: CAT, COPD assessment test.
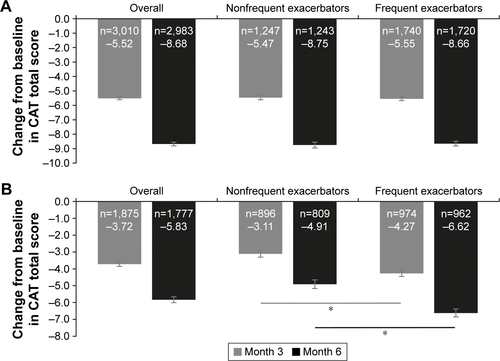
Table S1 Patient demographics and baseline characteristics (effectiveness sets)
Acknowledgments
DINO and DACOTA were sponsored by Takeda; AstraZeneca is the current study sponsor. Rebecca Birch, PhD, provided medical writing support, under guidance from the authors, on behalf of Synergy Vision, London, UK, funded by AstraZeneca, UK, in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). Kushal Banerjee, PhD, provided medical writing support in addressing the peer reviewer comments, under guidance from the authors, on behalf of Cactus Communications, Mumbai, India, funded by AstraZeneca, UK, in accordance with GPP3 guidelines.
Disclosure
IM is a former employee of Takeda and a current employee of AstraZeneca. PK reports personal fees from Takeda during the conduct of the study; personal fees from AstraZeneca, Chiesi, GSK, Novartis, Menarini, Teva, and Mundipharma outside the submitted work. CV reports no relevant conflicts of interest in the current study, and the following relevant financial activities outside of the submitted work: personal fees from Almirall, Cipla, Berlin Chemie/Menarini, CSL Behring, and Teva; grants and personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Grifols, Mundipharma, Novartis, and Takeda; grants from German Federal Ministry of Education and Research (BMBF) Competence Network Asthma and COPD (ASCONET), Bayer Schering Pharma AG, MSD, and Pfizer. RS reports no conflicts of interest in this work. The authors report no other conflicts of interest in this work.