
Abstract
Purpose
COPD and coronary artery disease (CAD) are common chronic diseases with shared risk factors. COPD continues to be largely underdiagnosed and undertreated. We aimed to describe the prevalence and predictors of undiagnosed COPD in Jordanian men with CAD.
Patients and methods
In a cross-sectional study conducted at a referral center in Jordan, male patients who underwent coronary angiography for suspected CAD and reported $10 pack-year of cigarette smoking were recruited. Pre- and post-bronchodilator spirometry was undertaken for all participants, and COPD was defined as post-bronchodilator FEV1/FVC <70%. The finding of ≥50% coronary luminal narrowing confirmed the presence of CAD.
Results
Spirometry was undertaken for 376 men with mean age of 56.02±10.55 years, and 72.6% were active cigarettes smokers with a mean pack-year of 55.89±34.25. A CAD diagnosis was confirmed in 300 (79.8%) men. Spirometric criteria for COPD were met in 76 (15.7%) patients, of whom 91.5% were not previously diagnosed. COPD-related symptoms were common: chronic cough (44.4%), dyspnea (66.2%), and wheezes (27.9%). COPD was more common in patients with (18.0%) compared to patients without (6.6%) CAD (P=0.014). Multivariate logistic regression showed that the risk of COPD was higher in patients with CAD (OR 3.16, 95% CI, 1.10–9.09, P=0.033) and in those with chronic bronchitis (OR 13.07, 95% CI, 6.69–25.52, P<0.001).
Conclusion
There was a high prevalence of COPD among male patients with CAD and most were underdiagnosed despite having respiratory symptoms. Male smokers with CAD and respiratory symptoms should be evaluated for airflow limitation and the presence of COPD.
Introduction
COPD is a common and preventable respiratory disease characterized by persistent symptoms and airflow limitation, caused mainly by exposure to tobacco smoking.Citation1 COPD is the fourth leading cause of death in the world and is projected to be the third leading cause of death by 2020;Citation2 it continues to be an important health burden.Citation1
Patients with COPD commonly have comorbidities, including coronary artery disease (CAD), which may complicate treatment and increases the morbidity and mortality of the affected individuals. Furthermore, CAD continues to be the leading cause of disability and death in subjects older than 35 yearsCitation3,Citation4 and accounts for half of all cardiovascular deaths in the United States.Citation3 The coexistence of COPD and CAD is expected, given the shared common risk factor of cigarette smoking and the increased prevalence of both diseases with advancing age. Moreover, systematic inflammation in COPD,Citation5 increased arterial stiffness, and endothelial dysfunction are potential modifiable mechanisms of cardiovascular morbidity and mortality in patients with COPD.Citation6
The reported prevalence of CAD in patients with COPD can be up to 60%, with a relative risk of CAD as high as seven-fold.Citation7 Furthermore, risk factors for CAD are common in individuals with COPD.Citation8 Although the prevalence of COPD in patients with CAD is not widely reported, available reports show that it ranges from 10.5% to 33.6% and most cases of COPD were not previously diagnosed.Citation9–Citation12 Lastly, patients with CAD who have coexisting COPD have increased morbidity and mortality,Citation12,Citation13 whereas cardiovascular disease comorbidity is an important cause of mortality in patients with COPD.Citation14
Prevalence and impact of both CAD and COPD is projected to increase in developing countries due to growing exposure to risk factors and an expected increase in the rate of tobacco consumption.Citation15 Despite the relatively young population, the prevalence of COPD across the Middle East region is 3.6%Citation16 and COPD is still largely underdiagnosed and undertreated.Citation17 Given the scarcity of evidence on the association between COPD and CAD in developing countries and in the Middle East region in particular,Citation18,Citation19 this study was conducted to describe the prevalence and predictors of COPD among male Jordanian smokers with angiographically proven CAD.
Material and methods
A cross-sectional study was conducted at the Prince Muna Cardiac Center, King Abdullah University Hospital in the northern part of Jordan. The hospital is a 600-bed referral center for a population of 2.8 million (one third of the Jordanian population). This study was approved by the Institutional Review Board of Jordan University of Science and Technology, and participants provided written informed consent. All adult male patients who underwent coronary angiography (CATH) for suspected CAD and had a history of cigarette smoking (≥10 pack-year) were recruited for the study. We excluded patients who were 1) unable to undertake spirometry testing (intubated, in shock, acute pulmonary edema, and patient with active angina pain) and 2) patients with a history of bronchial asthma or bronchiectasis.
During a single face-to-face encounter, sociodemographic data, smoking history, previous diagnosis of COPD, and risk factors for CAD were obtained. COPD-related symptoms were derived from the Arabic version of the Clinical COPD Questionnaire.Citation20 Pre- and post-bronchodilator spirometry using a portable spirometer (FlowScreen® CT; eResearch Technology GmbH, Höchberg, Germany) was conducted during the same session. Spirometry was undertaken by trained study coordinators and the results were interpreted by a staff pulmonologist according to standard guidelines.Citation21,Citation22 The device was calibrated on each testing day, according to the manufacturers’ instructions. The test was clearly explained and demonstrated to each participant. Forced expiratory maneuvers were repeated until three reproducible acceptable readings were obtained and the best FEV1, FVC, and FEV1/FVC ratios were used. The post-bronchodilator test was conducted during the same session for patients with a pre-bronchodilator FEV1/FVC ratio of less than 70% and 15 minutes after the inhalation of 400 µg salbutamol from a metered-dose inhaler (Ventolin®; GlaxoSmithKline plc, London, UK). COPD was defined as the presence of post-bronchodilator FEV1/FVC of less than 70%. Airflow limitation was graded according to the Global Initiative for Obstructive pulmonary Disease (GOLD) classification into GOLD 1 (FEV1≥80%), GOLD 2 (80%. FEV1≥50%), GOLD 3 (50%. FEV1≥30%), and GOLD 4 (FEV1<30%) stages. Chronic bronchitis was defined as having cough and sputum production for at least 3 months in each of two consecutive years. CATH procedures were carried out and reported by a staff cardiologist using a Philips coronary angiography device (Allura Xper FD10\10 Clarity, Phillips, Amsterdam, the Netherlands). Patients with luminal coronary vessel narrowing ≥50% were considered to have CAD.
Statistical analysis
The IBM Statistical Package for Social Sciences software (SPSS) for Windows, Version 24.0 (IBM Corp, Armonk, NY, USA) was used for data processing and analysis. Characteristics of the subjects’ variables were described using frequency distribution for categorical variables and mean and SD for continuous variables. Tests of significance between groups were carried out using the chi-squared test or Fisher’s exact test for categorical variables, whereas continuous variables were first examined for deviation from normality at P<0.01 (Levene’s test) and, after demonstrating a normal distribution, the Student’s t-test or ANOVA were conducted. Post hoc comparative analysis was conducted between different treatment groups of CAD and in those without CAD using Tukey’s HSD test. Multivariate logistic regression analysis with backward elimination was conducted (OR, elimination threshold P>0.1) to determine the predictors of COPD, including age, active smoking vs ex-smoking, presence of CAD, chronic bronchitis, and symptoms of chough, dyspnea, and wheezes. The results of the logistic regression analysis were presented as ORs and their 95% CIs. A P-value of <0.05 was considered statistically significant for all analyses conducted.
Results
Participants
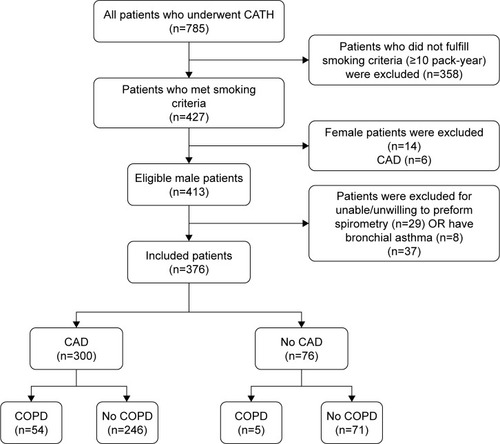
Between July and December 2017, a total of 785 patients underwent CATH, 427 (54.4%) met our cigarette-smoking criteria, and 413 (96.7%) were males. Thirty-seven patients were excluded for being unable/unwilling to complete spirometry (n=29) or for having bronchial asthma (n=8). Clinical data and spirometry were completed for 376 participants (91.0%) and were included in the analysis ().
Figure 1 Flow chart of study participants showing excluded patients at different stages of the study.
Mean age of all participants was 56.02±10.55 years (range 21–85 years) and most were active cigarette smokers (273; 72.6%) with a mean pack-year of 55.89±34.25 (range 10–240). Symptoms of COPD were common; 167 (44.4%) patients with chronic cough, 249 (66.2%) with dyspnea, 105 (27.9%) with wheezing, and 89 (23.7%) met the clinical criteria of chronic bronchitis. CATH results showed that 300 (79.8%) had coronary angiographic evidence of CAD – 249 (83.0%) were treated with percutaneous coronary angioplasty (PCI), 33 (11.0%) were referred for coronary artery bypass surgery (CABG), and 18 (6.0%) received medical therapy. Patients with CAD were older (P=0.008), had more diabetes mellitus (P=0.037) and hypertension (P=0.028), and had greater airflow limitation with lower FEV1 (P=0.034) and lower FEV1/FVC ratio (P=0.038). There was no difference in smoking habits, presence of hyperlipidemia, frequency of respiratory symptoms, or body mass index (BMI) between those with and without CAD ().
Table 1 Characteristics of the participants according to the coronary artery disease status
Chronic obstructive lung disease
describe the demographics, symptoms, and spirometry findings in patients with and without COPD. Fifty-nine patients (15.7%) met the GOLD criteria of COPD and 12 (20.3%) had GOLD 1, 40 (67.8%) had GOLD 2, and 7 (11.9%) had GOLD 3. The majority of patients with COPD (54; 91.5%) were not previously diagnosed. Patient with COPD were older (P<0.001), had higher smoking intensity (P=0.009), had lower BMI (P=0.001), and had more COPD-related symptoms (P<0.001) than those who did not have COPD. The prevalence of COPD increased with age from 6.5% in patients <50 years old to 37.5% in those ≥70 years, P<0.001. The pre-bronchodilator mean FEV1, % predicted was 65.64±15.61 (range 31%–118%) and the mean FEV1/FVC ratio was 63.46±6.98 (range 39.0%–76.0%) whereas the post-bronchodilator mean FEV1, % predicted was 68.25±15.82 (range 45%–102%) and the mean post-bronchodilator FEV1/FVC ratio was 63.98±6.58 (range 37.0%–69.7%).
Table 2 Characteristics and spirometry findings of participants with chronic obstructive lung disease
Multivariate logistic regression with backward elimination was conducted to identify independent predictors of COPD among patients who underwent CATH (). In addition to coexisting CAD (OR=3.16, 95% CI 1.10–9.09, P=0.033), increasing age (OR=1.07, 95% CI 1.03–1.10, P<0.001) and having chronic bronchitis (OR=13.07, 95% CI 6.691–25.52, P<0.001) were independent predictors of COPD.
Table 3 Multivariate logistic regression model for the predictors of COPD
COPD and CAD
COPD was more common in patients with CAD (54/300; 18.0%) compared to those without CAD (5/76; 6.6%) (P=0.014). The prevalence of COPD was 16.1% in the medical therapy group, 16.9% in the PCI group, and 27.3% in the CABG group (P=0.340). Similarly, the prevalence of COPD was not different between those who had single-vessel (17.1%), two-vessel (17.1%), or ≥3-vessel (19.1%) disease (P=0.191). ANOVA combined with post hoc analysis () showed that airflow limitation (FEV1 and FEV1, %) was more prominent in patients who required CABG compared with patients without CAD (P=0.006 and P=0.018), respectively. However, there was no difference in airflow limitation among different groups of CAD treatment (P>0.05).
Table 4 Spirometry findings according to therapeutic strategy of patients with coronary artery disease compared to patients without coronary artery disease
Discussion
This study described the prevalence of COPD in a population of male smokers with angiographically proven CAD in a developing country. Our main findings showed high prevalence of undiagnosed COPD in patients with CAD, and that the risk of COPD was higher in older patients with respiratory symptoms.
Our results were consistent with previous reports on the increased prevalence of COPD in patients with CAD.Citation9–Citation12 A large multicenter study in Europe examined the prevalence of airflow limitation consistent with COPD in current and ex-smokers with ischemic heart disease. The prevalence of COPD ranged from 18.3% to 41.3%, whereas 70.6% of all patients and one third of those with severe airflow limitation were underdiagnosed. In a study from Spain, 33.6% of patients with CAD had air flow limitation consistent with COPD. Although they reported higher prevalence than this study, their patients were mostly older males, and those without CAD had a high prevalence of COPD (17.5%).Citation9 In Japan, the prevalence of COPD in patients with CAD ranged from 10.5% to 25.9%.Citation10,Citation11 Most recently, a study from Spain used methodology and definitions similar to those in our study and showed that one fourth of patients who underwent PCI for CAD had COPD.Citation12 Despite these consistent reports on the association between CAD and COPD, the latter is still largely underdiagnosedCitation9,Citation11,Citation12,Citation18,Citation19 and carries higher mortality and morbidity.Citation12 In this study, the findings are in agreement with the inference in these reports: most patients with COPD who had CAD were not previously diagnosed. The low rate of diagnosis of COPD among our symptomatic heavy smokers is puzzling but in agreement with a previous study in primary care in Jordan.Citation17 This may be partly explained by the lack of spirometry service in most primary-care centers in Jordan, by the notion that patients may be diagnosed with chronic bronchitis but not made aware of the diagnosis, or patients may simply deny having a disease that is strongly linked to their smoking habit.
Using a different methodology, epidemiological and hospital-based studies addressed the prevalence and risk of cardiovascular diseases including CAD in patients with an established diagnosis of COPD.Citation7,Citation23 Results of a meta-analysis showed a consistent increased risk (two- to five-fold) of CAD in patients with COPD relative to those without COPD.Citation23 However, the risk appears to vary with the studied population, methodology of the study, and case definition. In the US population, 16.1% of patients with physician-diagnosed COPD had CAD, whereas 6.1% of patients without COPD had CAD. Patients with COPD were twice as likely to have CAD,Citation24 and this risk appears to be two times higher in those >60 years of age.Citation25 In a UK primary-care setting, the risk of acute myocardial infarction in patients with established diagnosis of COPD can be as high as ten-fold.Citation26 Finally, in various European populations, the prevalence of CAD in patients with COPD ranged from 14% to 30%.Citation23
Reports from developing countries on the association between COPD and CAD are scarce. In a small study from Sudan, 28% of patients with angiographically conformed CAD had FEV1 <80% and were considered to have COPD. Another study from Pakistan found that one third of patients with CAD (based on ECG criteria) had COPD (FEV1/FVC ratio <70%). Lastly, a large regional epidemiological study on the prevalence and impact of COPD in the Middle East and North Africa (BREATHE study) showed that the overall prevalence of COPD was 3.6% (ranging from 1.9% to 6.1%),Citation16 and one fourth of all subjects with COPD reported having coexisting cardiovascular disease.Citation27 Our results are comparable to these regional studies, with almost one-in-five men with CAD having COPD. The prevalence of COPD in subjects without CAD (6.6%) is comparable to what has been reported in the general population in Jordan (5.4%–8.2%).Citation16,Citation17
This significant association may be explained by the shared enhanced systemic inflammatory biomarkers including interleukin 6, C-reactive protein, and fibrinogen in patients with COPD and CAD,Citation5,Citation6 which is more prominent during COPD exacerbations.Citation28 Moreover, hypoxic stress and the impaired arterial flow-mediated dilation in COPDCitation29 may result in vascular dysfunction that is noted in patients with COPD. The prevalence of both COPD and CAD increases with advancing age. In this study, the prevalence of COPD increased from 6.5% in younger patients to 37.5% in the older ones. Lastly, our patient population showed a high smoking intensity – a shared risk factor for both diseases.
The coexistence of COPD and CAD is detrimental and associated with a negative impact on the outcome of the affected individuals. Patients with undiagnosed COPD who undergo PCI have higher morbidity and mortality,Citation12,Citation13 and cardiovascular comorbidity increases the burden of patients with COPD as more than a quarter of patients with COPD die of cardiovascular disease.Citation14,Citation30 Moreover, patients admitted for COPD exacerbation were found to have a high troponin level in the absence of acute coronary symptoms and a subsequent coronary angiography showed significant coronary stenosis.Citation31 A recent extended follow-up study on patients with CAD showed persistent increase of cardiovascular mortality in patients with coexisting COPD.Citation32 Additionally, when treating patients who are diagnosed with both COPD and CAD, the long-term use of beta-2 agonists is considered a safe practice,Citation33 and the use of cardio-selective beta-blockers in CAD may even lower the mortality of patients with COPD. Lastly, statins – commonly used in patients with CAD – may be helpful in treating coexisting COPD.Citation34
In this study, there was a trend toward increased prevalence of COPD in patients who were referred for CABG compared with those who had PCI or medical therapy, but the difference was not statistically significant. Similarly, there was no increase in prevalence with increasing number of diseased coronary vessels. These findings may be partially explained by the lack of power in this study to detect the differences as well as by the notion that choice of therapy may be influenced by other factors beside the severity and complexity of the coronary disease. Moreover, the sole use of the number of vessels to stratify the severity of CAD has limitations,Citation35 and a more comprehensive angiographic scoring system has been developed to better define the severity and prognosis of coronary atherosclerosis.Citation36,Citation37
This study had number of limitations that merit consideration. The study sample was recruited from a single referral center in Jordan, and women were not included in the analysis. Women represented <5% of smokers who had coronary angiography, and national data in Jordan showed that whereas one in two adult men smoke cigarettes, only 5% of women were regular smokers. This may limit the generalization of the results to the general population in Jordan and to other countries in the region. Furthermore, the study excluded patients with CAD and a smoking history of less than 10 pack-years and this may have resulted in an overestimation of the prevalence of COPD. In contrast, the study did not include patients with acute myocardial infarction and patients who were too ill to carry out spirometry, which may have resulted in a lower prevalence of COPD. Finally, the study was cross-sectional in nature and, therefore, was not intended to identify the impact of this strong association on short- and long-term morbidity and mortality of patients with CAD. Further multicenter and longitudinal studies using a robust scoring system of the severity of CAD are needed to address the impact of airflow limitation and COPD on the outcomes of patients with CAD in developing countries.
Conclusion
There was a high prevalence of COPD among male patients with CAD and most were underdiagnosed despite having respiratory symptoms. Smoking men with CAD and respiratory symptoms should be evaluated for airflow limitation and the presence of COPD.
Acknowledgments
The authors thank Mr Bryan Simmons for proofreading the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- Global Initiative for Chronic Obstructive Lung Disease (GOLD)The Global Strategy for the Diagnosis, Management and Prevention of COPD2017 Available from: http://goldcopd.orgAccessed May 20, 2017
- LopezADShibuyaKRaoCChronic obstructive pulmonary disease: current burden and future projectionsEur Respir J200627239741216452599
- NicholsMTownsendNScarboroughPRaynerMCardiovascular disease in Europe 2014: epidemiological updateEur Heart J201435422929295925381246
- BenjaminEJBlahaMJChiuveSEHeart Disease and Stroke Statistics-2017 Update: A Report From the American Heart AssociationCirculation201713510e146e60328122885
- CelliBRLocantoreNYatesJInflammatory biomarkers improve clinical prediction of mortality in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2012185101065107222427534
- MaclayJDMacneeWCardiovascular disease in COPD: mechanismsChest2013143379880723460157
- MüllerovaHAgustiAErqouSMapelDWCardiovascular comorbidity in COPD: systematic literature reviewChest201314441163117823722528
- SchnellKWeissCOLeeTThe prevalence of clinically-relevant comorbid conditions in patients with physician-diagnosed COPD: a cross-sectional study using data from NHANES 1999–2008BMC Pulm Med2012122622695054
- SorianoJBRigoFGuerreroDHigh prevalence of undiagnosed airflow limitation in patients with cardiovascular diseaseChest2010137233334019783666
- WadaHNakanoYNagaoTDetection and prevalence of chronic obstructive pulmonary disease in a cardiovascular clinic: evaluation using a hand held FEV1/FEV6 meter and questionnaireRespirology20101581252125820920134
- OnishiKYoshimotoDHaganGWJonesPWPrevalence of airflow limitation in outpatients with cardiovascular diseases in JapanInt J Chron Obstruct Pulmon Dis2014956356824920894
- AlmagroPLapuenteAParejaJUnderdiagnosis and prognosis of chronic obstructive pulmonary disease after percutaneous coronary intervention: a prospective studyInt J Chron Obstruct Pulmon Dis2015101353136126213464
- ZhangMChengYJZhengWPImpact of Chronic Obstructive Pulmonary Disease on Long-Term Outcome in Patients with Coronary Artery Disease Undergoing Percutaneous Coronary InterventionBiomed Res Int201620168212459628042573
- CalverleyPMAndersonJACelliBCardiovascular events in patients with COPD: TORCH study resultsThorax201065871972520685748
- Aït-KhaledNEnarsonDBousquetJChronic respiratory diseases in developing countries: the burden and strategies for prevention and managementBull World Health Organ2001791097197911693980
- TageldinMANaftiSKhanJADistribution of COPD-related symptoms in the Middle East and North Africa: results of the BREATHE studyRespir Med2012106Suppl 2S25S3223290701
- Al OmariMKhassawnehBYKhaderYDauodASBergusGPrevalence of chronic obstructive pulmonary disease among adult male cigarettes smokers: a community-based study in JordanInt J Chron Obstruct Pulmon Dis2014975375825092972
- AhmedAHYagoubTEMuthanaFPrevalence of chronic obstructive pulmonary disease in patients with catheter-diagnosed coronary artery diseaseAnn Thorac Med200942919219561931
- UllahRSalamSGhaffarTMuhammadRKhanIFrequency Of Undiagnosed Chronic Obstructive Pulmonary Disease In Patients With Coronary Artery DiseaseJ Ayub Med Coll Abbottabad201729228528828718249
- van der MolenTWillemseBWSchokkerSTen HackenNHPostmaDSJuniperEFDevelopment, validity and responsiveness of the Clinical COPD QuestionnaireHealth Qual Life Outcomes2003111312773199
- Global Initiative for Chronic Obstructive Lung DiseaseGOLD spirometry guide2010 Available from: http://goldcopd.org/gold-spirometry-guide/Accessed May 20, 2017
- PellegrinoRViegiGBrusascoVInterpretative strategies for lung function testsEur Respir J200526594896816264058
- ChenWThomasJSadatsafaviMFitzgeraldJMRisk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysisLancet Respir Med20153863163926208998
- FinkelsteinJChaEScharfSChronic obstructive pulmonary disease as an independent risk factor for cardiovascular morbidityInt J Chron Obstruct Pulmon Dis2009433734919802349
- FranssenFMESorianoJBRocheNLung Function Abnormalities in Smokers with Ischemic Heart DiseaseAm J Respir Crit Care Med2016194556857627442601
- FearyJRRodriguesLCSmithCJHubbardRBGibsonJEPrevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary careThorax2010651195696220871122
- UzaslanEMahboubBBejiMThe burden of chronic obstructive pulmonary disease in the Middle East and North Africa: results of the BREATHE studyRespir Med2012106Suppl 2S45S5923290704
- HurstJRPereraWRWilkinsonTMDonaldsonGCWedzichaJAExacerbation Of Chronic Obstructive Pulmonary Disease: Pan-Airway and Systemic Inflammatory IndicesProc Am Thorac Soc20063648148216921117
- EickhoffPValipourAKissDDeterminants of Systemic Vascular Function in Patients with Stable Chronic Obstructive Pulmonary DiseaseAm J Respir Crit Care Med2008178121211121818836149
- HuiartLErnstPSuissaSCardiovascular Morbidity and Mortality in COPDChest200512842640264616236937
- PizarroCHerweg-SteffensNBuchenrothMInvasive coronary angiography in patients with acute exacerbated COPD and elevated plasma troponinInt J Chron Obstruct Pulmon Dis2016112081208927695304
- AlmagroPde La SierraAAcostaESpirometrically Confirmed Chronic Obstructive Pulmonary Disease Worsens Long-Term Prognosis after Percutaneous Coronary InterventionAm J Respir Crit Care Med2018197682482628885856
- DecramerMLHananiaNALotvallJOYawnBPThe safety of long-acting beta2-agonists in the treatment of stable chronic obstructive pulmonary diseaseInt J Chron Obstruct Pulmon Dis20138536423378756
- ZhangWZhangYCwLJonesPWangCFanYEffect of Statins on COPD: A Meta-Analysis of Randomized Controlled TrialsChest201715261159116828847550
- RingqvistIFisherLDMockMPrognostic value of angiographic indices of coronary artery disease from the Coronary Artery Surgery Study (CASS)J Clin Invest1983716185418666863543
- FarooqVvan KlaverenDSteyerbergEWAnatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients: development and validation of SYNTAX score IILancet2013381986763965023439103
- NeelandIJPatelRSEshtehardiPCoronary angiographic scoring systems: an evaluation of their equivalence and validityAm Heart J20121644e541547552