

Abstract
Background
It has recently been proposed that the concept of clinical control in COPD may be useful for deciding treatment in COPD, but the original control criteria (OCC) were considered too restrictive.
Objective
Define and subsequently validate “modified” control criteria (MCC) of COPD.
Method
Prospective observational study in COPD patients with a 1-year follow-up. Control was defined as the presence of low clinical impact and clinical stability. To evaluate clinical impact, the following clinical parameters were assessed: the degree of dyspnea, use of rescue medication, physical activity, and sputum color. Stability was assessed by clinical changes and exacerbations in the last 3 months. The COPD assessment test score and their changes were also evaluated as alternative control criteria. To define the MCC, adjustment for disease severity using BODEx index (MCC-B) or FEV1 (MCC-F) was evaluated, and the best cutoff point was established. Time to first combined event (emergency visit, hospitalization, or death) was analyzed to evaluate the predictive capacity of risk of the OCC, MCC-B, and MCC-F.
Results
We included 265 patients, 224 (83.9%) men, with a mean age (±SD) of 68±9 years and FEV1 of 58%±17%. The proportion of controlled patients was higher using clinical MCC-B or MCC-F (61.5% and 59.6%) than OCC (27.5%). Similar percentages were found using COPD assessment test scores. The time to the first combined event was significantly greater in controlled patients using MCC criteria (P<0.001, all cases). The predictive capacity of risk was similar in MCC-B (c-statistic [C]=0.639) and MCC-F (C=0.637) and higher than OCC (C=0.589).
Conclusions
The new MCC identified a higher number of controlled COPD patients. These patients have a better quality of life and lower risk of poor outcomes. The concept of control and the new MCC could be a useful tool to optimize therapy.
Supplementary materials
Figure S1 Accumulated probability of exacerbation in patients controlled or non controlled according to modified criteria of control adjusted by FEV1%.
Notes: (A) control was defined by clinical evaluation; (B) control was defined using the CAT scores.
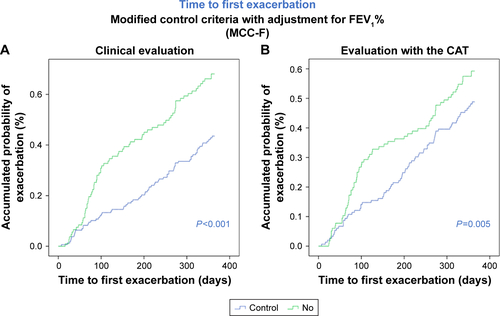
Table S1 Correlation coefficient between the variables included in the model and the level of severity measured by BODEx index or FEV1(%)
Table S2 Sensitivity, specificity, and Youden index of different cutoff points for CAT score
Table S3 Agreement between clinical impact evaluated by clinical assessment or by CAT (Kappa index), according to the number of criteria needed to define clinical control
Table S4 Predictive capacity of a composite event (c-statistic) according to the number of criteria needed to define clinical impact
Table S5 CAT score at 12 months, according to different control criteria
Disclosure
JJSC has received speaker fees from AstraZeneca, Boeh-ringer Ingelheim, Chiesi, Esteve, Ferrer, GSK, Menarini, Novartis, and Pfizer, and consulting fees from Air Liquide, Boehringer Ingelheim, Chiesi, GSK, AstraZeneca, Ferrer, and Novartis. BA reports personal fees and grants from Novartis AG, personal fees from BoehringerIngelheim, personal fees from GSK, personal fees from AstraZeneca, grants and personal fees from Menarini, outside the submitted work; M Miravitlles has received speaker or consulting fees from (in alphabetical order) Bial, Boehringer Ingelheim, Chiesi, Cipla, CSL Behring, Laboratorios Esteve, Gebro Pharma, GlaxoSmithKline, Grifols, Menarini, Mereo Biopharma, Novartis, pH Pharma, Rovi, TEVA, Verona Pharma and Zambon, and research grants from GlaxoSmithKline and Grifols, all outside the submitted work. The authors report no other conflicts of interest in this work.