
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Individuals with COPD may experience ambulatory difficulty due to both effort intolerance arising from respiratory dysfunction and impaired balance control during walking. However, the trunk movement during walking has not been evaluated or adjusted for patients with COPD. The Lissajous index (LI) visually and numerically evaluates the left–right symmetry of the trunk movement during walking and is useful in clinical practice. In COPD patients, the LI is used as an indicator of the left–right symmetry of the trunk during walking. Here, we used the LI to evaluate the symmetry of COPD patients based on bilateral differences in mediolateral and vertical accelerations, and we investigated the correlation between the patients’ symmetry evaluation results and their physical function.
Patients and methods
Sixteen stable COPD patients (all males; age 71.3±9.2 years) and 26 healthy control subjects (15 males; age 68.2±6.9 years) participated in this study. They performed the 10-minute walk test at a comfortable gait speed wearing a triaxial accelerometer, and we measured their trunk acceleration for the evaluation of symmetry. Motor functions were also evaluated in the patients with COPD.
Results
The average mediolateral bilateral difference and LI values of the COPD patients were significantly larger than those of the healthy subjects. The COPD patients’ LI values were significantly correlated with their static balance.
Conclusion
The LI measured using a triaxial accelerometer during walking is useful in balance assessments of patients with COPD.
Introduction
Individuals with COPD may have an ambulatory disability due to both effort intolerance arising from respiratory dysfunction and impaired gait parameters. The impairment of gait parameters includes the decreasing step length, cadence, and gait speed.Citation1,Citation2 Gait parameter deficits in daily living increase the risk of falling.Citation1 Many studies have recorded the gait in patients with COPD using a three-dimensional (3D) motion capture system and a pressure-sensitive mat.Citation3 A pressure-sensitive mat and 3D motion capture system can only assess a limited number of consecutive strides due to space and equipment constraints.Citation4,Citation5 In addition, 3D motion capture system is very expensive.Citation6 In contrast, triaxial accelerometers are small and useful to measure gaits in various environments.Citation7 Recent studies have reported that gait analysis using triaxial accelerometers has many advantages and reliability of measurement.Citation8–Citation11 Several gait parameters associated with acceleration have been developed, eg, the Lissajous index (LI)Citation7 for evaluating gait symmetry of the trunk movement, the root mean squareCitation11,Citation12 representing the average of trunk acceleration amplitudes, and the harmonic ratioCitation13 indicating the smoothness of a gait.
In our previous study, the LI visually and numerically evaluated the left–right symmetry of a Lissajous figure (LF); this LF is made from trunk acceleration data.Citation14 Further, it was clear that the LI during gait was effective at evaluating gait balance in patients with stroke.Citation14 The gait parameter has been found useful for the patients with COPD, but the trunk movement during walking has not been evaluated or adjusted for patients with COPD. It was considered that the patients with COPD have the abnormal trunk movement during walking by impaired gait parameters.
The purpose of this study was to evaluate the trunk movement using the LF and the LI, to compare the LI with the uniaxial acceleration, and to examine the relation between LI and body function in patients with COPD.
Patients and methods
Subjects
Sixteen stable elderly COPD patients (all male; aged 71.3±9.2 years) who had undergone pulmonary rehabilitation at Akita City Hospital were enrolled in this study. Twenty-six healthy control subjects (15 males; aged 68.2±6.9 years) who had worked at the Akita Prefectural Center for Rehabilitation and Psychiatric Medicine were also enrolled. All subjects provided written informed consent.
The following patients were excluded: 1) patients who were not able to walk by themselves without canes, 2) those with an illness or injury other than COPD that impaired their behavior, and 3) those who did not understand the purpose of the experiment. The characteristics of the patients and healthy controls are summarized in .
Table 1 Characteristics of the COPD patients and healthy controls
Study design
For the measurement of trunk acceleration during walking, each subject wore the triaxial accelerometer described below and underwent a 10-minute gait test at a comfortable gait speed. The subject’s symmetry during his walking was calculated based on his trunk acceleration. The patients with COPD also underwent an evaluation of their motor function. This study was reviewed and approved by the Ethics Committees of Akita University Graduate School of Medicine (2015; approval no 1319) and carried out in conformity with Declaration of Helsinki.
Accelerometer
The small (20 g) wireless triaxial accelerometer (MG-M1110; LSI Medience, Tokyo, Japan)Citation9,Citation10 is 75 mm long, 50 mm high, and 20 mm wide (). The sampling rate was 100 Hz. The accelerometer was used to measure the vertical (VT), anteroposterior (AP), and mediolateral (ML) acceleration of the subject’s trunk during his gait. Each aspect of acceleration is indicated by graphs produced by the accelerometer’s analysis software for a personal computer (MG-M1110-PC™; LSI Medience).Citation9,Citation10 This software calculated the steps, gait speed, and gait coefficient of variation and exported the values of each aspect of acceleration into Microsoft’s Excel program.
Figure 1 A triaxial accelerometer (MG-M1110; LSI Medience, Tokyo, Japan).
Accelerometer measurements
The accelerometer was fixed to a belt at the level of the subject’s L3 spinous process (). All subjects performed the 10-minute walk test twice for the recording of definitive data on trunk acceleration. A 10-m-long walkway with a 1-m spare walkway area at both the start and the end was constructed. The subject was instructed to walk straight at a self-selected comfortable speed toward a target line on the floor, without the use of a cane. The acceleration measurements were performed twice by the same tester. The acceleration data of second walk test was used for analysis. All acceleration data from the 10-m walk except for the first and final steps were used.
Symmetry evaluation (ML or VT acceleration)
The MG-M1110 displays the ML acceleration waveforms as “x” and the VT acceleration waveforms as “y”. A positive x-value indicates acceleration to the left, and a negative x-value indicates acceleration to the right. Thus, for our comparison of the amount of acceleration occurring on the left and right, we calculated the maximum difference in the absolute value for lateral acceleration (Δx lateral). The difference between the maximum value for VT acceleration when the right leg is in the stance phase and the maximum value for VT acceleration when the left leg is in the stance phase (Δy lateral) was also calculated.
Symmetry evaluation (Lissajou index)
We calculated the LI,Citation7,Citation14 which indicates the symmetry based on both ML and VT accelerations. For the calculation of an LI, an LF must be drawn. Using Excel, the LF was graphed on a scatter chart with the y-axis representing VT acceleration and the x-axis representing ML acceleration. shows the LF made from actual measured values of trunk acceleration. The quadrangle surrounded by the undulating line (Rr) and the quadrangle surrounded by the undulating and dotted lines (Rl) were the calculated areas ().
Figure 2 Lissajous figure.
Abbreviations: L, left; R, right; Rl, rectangle area of left, the quadrangle surrounded by undulating and dotted line; Rr, rectangle area of right, the quadrangle surrounded by undulating line.
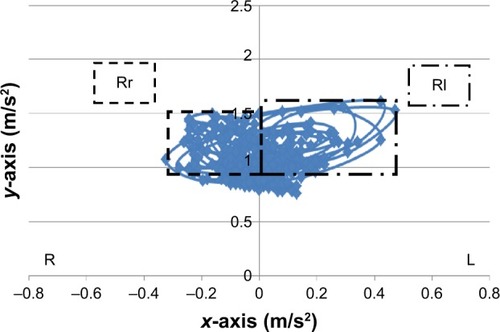
The following formulae were used to calculate the values of Rr and Rl:
The formula for calculating the LI is as follows:
A large LI value indicates asymmetry, and small LI values denote symmetry on the frontal plane.
Motor function
The severity level of the patients’ COPD was evaluated with the Global Initiative for Chronic Obstructive Lung Disease (GOLD),Citation15 and the patients’ dyspnea was evaluated with the Modified Medical Research Council scale.Citation16 For the pulmonary function, we measured the %FVC (% forced volume capacity), %FEV1, and FEV1/FVC with the use of a spirometer (Chestgraph Jr. HI-101, Chest M.I., Tokyo, Japan).Citation17 The static balance was evaluated with the one-leg standing test (OLST), and the dynamic balance was evaluated with the short physical performance battery (SPPB)Citation18 and the muscle strength of leg with the Weight Bearing Index of quadriceps.Citation19 The 6-minute walk distance was measured as an indicator of functional exercise capacity.Citation20 Motor function was evaluated only in the COPD patients.
Statistical analyses
The LI, Δx lateral, and Δy lateral values in the COPD group and control group were compared with an unpaired t-test. The relationships of the Δx lateral and LI values in the COPD group with all physical functions were investigated using Pearson correlation coefficient for analyses on quantitative variables and Spearman correlation in the case of ordinal variables. The statistical software SPSS Statistics 24 was used for the analyses. The level of significance was set at 5%.
Results
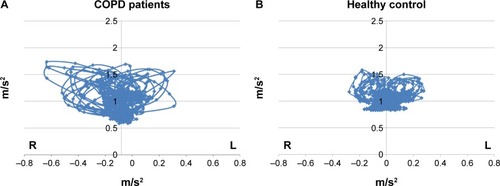
shows the actual LF of the healthy subjects and the patients with COPD. From this figure, it is clear that the LFs of the patients with COPD were larger and more asymmetric than the LFs of the healthy subjects. illustrates the LI, the Δx lateral, and the Δy lateral of the patients with COPD and the healthy subjects. An unpaired t-test revealed that both the average LI value and the x-bilateral difference of the COPD patients were significantly larger than those of the healthy subjects (P=0.02 and P=0.007, respectively).
Table 2 Symmetry evaluation of COPD patients and healthy control
Figure 3 Actual Lissajous figures.
Abbreviations: L, left; R, right.
The results of the correlation analysis are given in . The LI values of the patients with COPD were significantly correlated with their OLST results (P=0.042).
Table 3 Correlation coefficient between symmetry evaluation and motor function in patients with COPD
Discussion
In this study, the trunk acceleration of patients with COPD and healthy subjects was measured during walking at a comfortable speed for 10 minutes by a triaxial accelerometer at the waist. To evaluate the trunk movement during walking, the Δx lateral, Δy lateral, and LI values were calculated based on the acceleration data. The Δx lateral value was significantly higher in the COPD group compared with the healthy controls. The Δy lateral demonstrated no significant difference between the two groups. The LI of the COPD patients was significantly higher than that of the healthy controls, and the LI was shown to be related to the patients’ standing balance ability.
The Δx lateral value was significantly higher in the COPD group compared with the healthy controls. Lim et alCitation21 reported that decreased movement in the gluteal muscles and the erector spinae muscle in elderly individuals leads to increases in trunk acceleration in the lateral direction. It has also been indicated that COPD often exhibits severe muscle wasting.Citation22 It is thus possible that decreased muscle strength in the trunk and legs of patients with COPD has an effect on the lateral asymmetry of both their lateral acceleration and trunk acceleration.
We observed that the LI values of the COPD patients were significantly higher than those of the healthy subjects. The LI values of the COPD group were also correlated with their results on the OLST, which assesses standing balance. In a previous study, the standing balance ability in COPD patients was lower than that of healthy subjects.Citation23 Our present group of COPD patients was composed of patients who did not have conditions that affected one side of their bodies, such as hemiplegia or orthopedic disorders. Our findings indicate that decreased balance ability in patients with COPD is related to their increased lateral asymmetry during walking.
Among the evaluations of trunk movement in the present study, the LI of COPD patients was the only measurement that was not only significantly larger than the LI of healthy individuals but also related to standing balance. In recent years, there has been increasing research focusing on the decrease in COPD patients’ balance ability.Citation24,Citation25 Bernabeu-Mora et al reported the correlation between impairment of balance ability and physical function using each test of the SPPB, which assesses dynamic balance.Citation26 Several reports indicated that decreases in the level of physical activity, which affect the prognosis of patients with COPD, can cause reduced balance ability.Citation27–Citation29 Compared with healthy individuals, COPD patients take a longer time to correct losses of balance while walking, and they require more trunk muscle activity.Citation30 If patients with COPD fall and injure themselves, they may experience decreased physical functions, and their resulting reluctance to walk may lead to decreased levels of physical activity.Citation31,Citation32
Based on these findings, it is extremely important to use an approach for COPD patients that assesses their balance while walking. Based on the presented findings, the LI measured using a triaxial accelerometer is useful in balance assessments.
This study had three limitations. First, the number of subjects analyzed was small. For the precise determination of the usefulness of balance assessments during walking in patients with COPD, further studies are required with greater numbers of subjects, including those with stage IV conditions. Second, the lateral differences in the legs’ muscle strength were not evaluated in both the COPD and healthy groups. Third, we did not measure the leg or trunk muscle strength of any muscle other than the quadriceps. Trunk acceleration is affected by the muscles of the trunk, the gluteal region, and the legs. Further research that measures the muscle strength in the other regions is required.
Conclusion
The present study is the first research of the trunk movement during walking in the patients with COPD. The lateral symmetry of COPD patients during walking could be evaluated based on the LI obtained by a triaxial accelerometer. In addition, the LI values of the COPD patients were associated with their standing balance. The ambulatory disability of COPD patients is affected by not only their effort intolerance due to respiratory dysfunction but also their underlying balance control. If patients with COPD fall and injure themselves, they may experience decreased physical functions, and their resulting reluctance to walk may lead to decreased levels of physical activity. It is very important to use an approach that assesses balance while walking in patients with COPD. Our present findings demonstrate that the LI is a useful parameter for virtual and numerical evaluations of the walking balance of individuals with COPD.
Disclosure
The authors report no conflicts of interest in this work.
References
- AnnegarnJSpruitMASavelbergHHDifferences in walking pattern during 6-min walk test between patients with COPD and healthy subjectsPLoS One201275e3732922624017
- KarpmanCBenzoRGait speed as a measure of functional status in COPD patientsInt J Chron Obstruct Pulmon Dis2014991315132025473277
- LahousseLVerlindenVJvan der GeestJNGait patterns in COPD: the Rotterdam StudyEur Respir J2015461889525700390
- YentesJMSchmidKKBlankeDRombergerDJRennardSIStergiouNGait mechanics in patients with chronic obstructive pulmonary diseaseRespir Res2015163125849481
- HowellDOsternigLChouLSMonitoring recovery of gait balance control following concussion using an accelerometerJ Biomech201548123364336826152463
- HenriksenMLundHMoe-NilssenRBliddalHDanneskiod-SamsøeBTest-retest reliability of trunk accelerometric gait analysisGait Posture200419328829715125918
- YamaguchiRHirataSDoiTMiuraYThe usefulness of a new gait symmetry parameter derived from Lissajous figures of tri-axial acceleration signals of the trunkJ Phys Ther Sci2012245405408
- OsakaHShinkodaKWatanabeSAssociation between trunk acceleration during walking and clinically assessed balance in patients with strokeNeuro Rehabilitation201741478379029254113
- YoneyamaMMitomaHOkumaYAccelerometry-based long-term monitoring of movement disorders: from diurnal gait behavior to nocturnal bed mobilityJ Mech Med Biol20131321350041
- YoneyamaMKuriharaYWatanabeKMitomaHAccelerometry-based gait analysis and its application to Parkinson’s disease assessment-part 2: a new measure for quantifying walking behaviorIEEE Trans Neural Syst Rehabil Eng2013216999100523797284
- Moe-NilssenRTest-retest reliability of trunk accelerometry during standing and walkingArch Phys Med Rehabil19987911137713859821897
- SekineMTamuraTYoshidaMA gait abnormality measure based on root mean square of trunk accelerationJ Neuroeng Rehabil20131011824370075
- BrachJSMcGurlDWertDVanswearingenJMPereraSChamRStudenskiSValidation of a measure of smoothness of walkingJ Gerontol A Biol Sci Med Sci201166113614120923910
- TeruiYSutoEKonnoYEvaluation of gait symmetry using a tri-axial accelerometer in stroke patientsNeuro Rehabilitation201842217318029562555
- VestboJHurdSSAgustíAGGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2013187434736522878278
- CelliBRMacNeeWATS/ERS Task ForceStandards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paperEur Respir J200423693294615219010
- Standardization of spirometry – 1987 updateStatement of the American Thoracic SocietyAm Rev Respir Dis19871365128512983674589
- GuralnikJMSimonsickEMFerrucciLA short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admissionJ Gerontol1994492M85M948126356
- SugawaraKTakahashiHKashiwaguraTEffect of anti-inflammatory supplementation with whey peptide and exercise therapy in patients with COPDRespir Med2012106111526153422857881
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function LaboratoriesATS statement: guidelines for the six-minute walk testAm J Respir Crit Care Med2002166111111712091180
- LimYPLinYCPandyMGMuscle function during gait is invariant to age when walking speed is controlledGait Posture201338225325923267819
- Skeletal muscle dysfunction in chronic obstructive pulmonary diseaseA statement of the American Thoracic Society/European Respiratory SocietyAm J Respir Crit Care Med19991594 Pt 2S1S4010194189
- IwakuraMOkuraKShibataKKawagoshiASugawaraKTakahashiHShioyaTRelationship between balance and physical activity measured by an activity monitor in elderly COPD patientsInt J Chron Obstruct Pulmon Dis2016111505151427445470
- RoigMEngJJMacIntyreDLRoadJDFitzGeraldJMBurnsJReidWDFalls in people with chronic obstructive pulmonary disease: an observational cohort studyRespir Med2011105346146920869227
- PortoEFCastroAASchmidtVGRabeloHMKümpelCNascimentoOAJardimJRPostural control in chronic obstructive pulmonary disease: a systematic reviewInt J Chron Obstruct Pulmon Dis2015101233123926170652
- Bernabeu-MoraRGiménez-GiménezLMMontilla-HerradorJGarcía-GuillamónGGarcía-VidalJAMedina-MirapeixFDeterminants of each domain of the Short Physical Performance Battery in COPDInt J Chron Obstruct Pulmon Dis2017122539254428883721
- BeauchampMKSibleyKMLakhaniBRomanoJMathurSGoldsteinRSBrooksDImpairments in systems underlying control of balance in COPDChest201214161496150322116798
- VoicaASOanceaCTudoracheECrisanAFFira-MladinescuOTudoracheVTimarBChronic obstructive pulmonary disease phenotypes and balance impairmentInt J Chron Obstruct Pulmon Dis20161191992527199555
- KawagoshiAKiyokawaNSugawaraKTakahashiHSakataSSatakeMShioyaTEffects of low-intensity exercise and home-based pulmonary rehabilitation with pedometer feedback on physical activity in elderly patients with chronic obstructive pulmonary diseaseRespir Med2015109336437125682543
- SmithMDChangATHodgesPWBalance recovery is compromised and trunk muscle activity is increased in chronic obstructive pulmonary diseaseGait Posture20164310110726471324
- CrişanAFOanceaCTimarBFira-MladinescuOTudoracheVBalance impairment in patients with COPDPLoS One2015103e012057325768731
- TudoracheEOanceaCAvramCFira-MladinescuOPetrescuLTimarBBalance impairment and systemic inflammation in chronic obstructive pulmonary diseaseInt J Chron Obstruct Pulmon Dis2015101847185226392759