
Abstract
COPD is a progressive condition involving chronic inflammation and parenchymal destruction with resulting airflow limitation. COPD is associated with worsening airflow limitation over time and increased frequency of COPD exacerbations, leading to increased mortality and morbidity. The effects of COPD extend beyond the lungs, as multiple comorbidities may occur with COPD, including cardiovascular disease, diabetes mellitus, osteoporosis, depression, and pneumonia. COPD exacerbations are associated with a rapid worsening of baseline symptoms that requires prompt management and may necessitate hospitalization in the case of a severe episode. Patients with COPD exacerbations require urgent management of symptoms to prevent further worsening, and preventative steps may be taken to help reduce the number and frequency of future exacerbations. Roflumilast is a potent and selective inhibitor of the enzyme phosphodiesterase-4 that targets the systemic inflammation associated with COPD. Roflumilast has a variety of anti-inflammatory effects including decreasing inflammatory mediators and the expression of cell surface markers and inhibition of apoptosis. Several clinical trials evaluating roflumilast in the treatment of COPD have demonstrated significant improvements from baseline versus placebo in lung function, including increases in mean pre- and postbronchodilator forced expiratory volume in 1 second and forced vital capacity. Data suggest that roflumilast reduces moderate to severe exacerbations with the benefit most well established in patients with severe disease. Given this evidence, roflumilast, as part of a combination regimen with long-acting bronchodilators, appears to be a reasonable treatment option for patients with severe to very severe COPD associated with chronic bronchitis and a history of exacerbations.
Introduction
COPD is a progressive condition that usually leads to a steady decline in lung function, increased symptoms, and recurrent and worsening exacerbations.Citation1 The progressive airflow limitation that characterizes COPD is a result of chronic airway inflammation in response to the inhalation of noxious stimuli and resulting parenchymal destruction.Citation2 Many systemic inflammatory markers have been associated with COPD health status and its extrapulmonary effects.Citation1,Citation3,Citation4 Inflammatory cells, tissue swelling, and accumulated mucus directly obstruct airways, but also activate innate repair mechanisms that remodel and thicken airway walls over time, leading to parenchymal destruction.Citation5,Citation6 Parenchymal destruction leads to further decreased gas transfer and increased air trapping. Overall, the combined pathological defects of COPD translate to symptoms of breathlessness, coughing, and variable sputum production that greatly impact a patient’s quality of life.Citation2
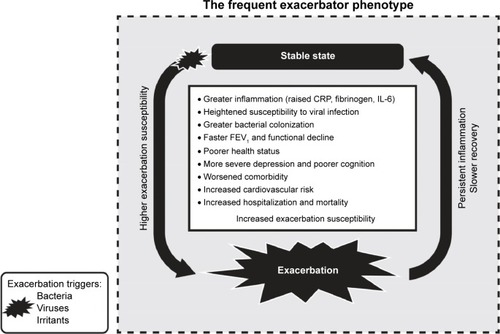
COPD is associated with an approximate 3.5-fold increase in the risk of death and is linked to multiple comorbidities, including hypertension, heart failure, ischemic heart disease, diabetes mellitus, myocardial infarction, osteoporosis, depression, and pneumonia.Citation7–Citation9 Exposure to viral or bacterial pathogens or inhalation of pollutants may be sufficient to precipitate a COPD exacerbation, defined as an acute worsening of a patient’s baseline symptoms.Citation10–Citation12 COPD exacerbations are accompanied by marked increases in systemic inflammatory mediators,Citation13–Citation16 decreased quality of life,Citation17 and further elevated risk of morbidity and mortality with each successive exacerbation compared with baseline disease.Citation18–Citation20 Some patients with COPD may be more prone to frequent COPD exacerbations () and thus present a greater therapeutic challenge.Citation10 This recognition is underscored in the guidelines for the management of COPD, which emphasize the importance of minimizing the impact of current exacerbations and preventing the development of subsequent exacerbations.Citation21,Citation22
Figure 1 Schematic of the frequent exacerbator phenotype.
Abbreviations: CRP, C-reactive protein; FEV1, forced expiratory volume in 1 second; IL-6, interleukin-6.
The purpose of this review is to highlight the pharmacology, clinical efficacy, tolerability, and place in therapy of roflumilast for the treatment of patients with COPD.
Pharmacology
Pharmacodynamics
Roflumilast, a potent and selective inhibitor of phosphodiesterase-4 (PDE4), is indicated for treatment to reduce the risk of COPD exacerbations in patients with severe COPD associated with chronic bronchitis and a history of exacerbations.Citation23,Citation24 Selective inhibition of PDE4 inhibits the hydrolysis of cyclic adenosine monophosphate (cAMP) in inflammatory cells.Citation25 Increased intracellular cAMP results in a wide range of anti-inflammatory effects, including decreased release of inflammatory mediators in neutrophils, decreased release of cytokines,Citation24 decreased expression of cell surface markers in many cell types, and decreased apoptosis. The suppression of inflammatory mediators and cytokines usually translates into benefits for patients with COPD exacerbations who often have elevated markers of inflammation compared to patients with baseline disease.Citation26 Roflumilast also reduces allergen-induced inflammationCitation27 and has been shown to stabilize lipopolysaccharide-induced systemic inflammation.Citation28
Pharmacokinetics
Roflumilast is available in a once-daily oral dosage form (500 µg tablets) with a bioavailability of approximately 80%.Citation23 Maximum plasma concentrations of roflumilast are achieved in ~1 hour (range: 0.5–2 hours) after a single dose, and maximum concentrations of the active N-oxide metabolite are achieved in ~8 hours (range: 4–13 hours). Roflumilast and its active metabolite are both highly protein bound in plasma (≥97%). Metabolism occurs by Phase I cytochrome P450 (CYP) reactions (isoenzymes 1A2 and 3A4) and by Phase II conjugation, and the half-life is approximately 17 hours.Citation23 While roflumilast is three times more potent than its metabolite, the metabolite has approximately ten times greater exposure (plasma area under the curve) than the active drug. Patients with hepatic dysfunction may have impaired elimination, although dose adjustments are not necessary.Citation29 No dosage adjustments are required for renal impairment.Citation23 However, roflumilast should not be coadministered with strong inhibitors of CYP3A4 or dual inhibitors of CYP3A4 and CYP1A2 (eg, erythromycin, ketoconazole, fluvoxamine, enoxacin, cimetidine, or rifampicin).Citation23 The macrolide azithromycin, which is commonly used in patients with COPD, is only a weak inhibitor of CYP3A4 and is expected to interact with roflumilast to a much lesser degree than erythromycin.Citation30
Clinical efficacy
The clinical efficacy and safety of roflumilast in the treatment of COPD has been evaluated in nine Phase III/IV randomized double-blind clinical trials, including studies M2-107, M2-111, M2-112, M2-124, M2-125, M2-127, M2-128, ACROSS (ClinicalTrials.gov identifier: NCT1313494), and REACT (Roflumilast in the Prevention of COPD Exacerbations While Taking Appropriate Combination Treatment; NCT1329029) ().Citation31–Citation36 Patients in these studies were required to have at least a 10–20-year pack history of smoking. Studies M2-111, M2-112, M2-124, M2-125, and REACT included only patients with severe to very severe airflow limitation as assessed by Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria (ie, forced expiratory volume in 1 second [FEV1] ≤50%).Citation31,Citation34–Citation36 Across all Phase III studies, active treatment with 500 µg of roflumilast was associated with improvements from baseline in lung function, including increases in mean pre- and post-bronchodilator FEV1 ranging from 39 to 88 mL and from 45 to 97 mL, respectively, compared with placebo with all differences statistically significant (P<0.0001).Citation31–Citation33,Citation35–Citation37 In addition, postbronchodilator forced vital capacity increased 58–114 mL compared with placebo (P<0.05).
Table 1 Randomized double-blind trials evaluating roflumilast in patients with COPD
While studies M2-111 and M2-112 demonstrated that roflumilast was associated with improved lung function in patients with severe COPD, neither study demonstrated a significant effect on exacerbations, although there was a trend toward lower exacerbations for roflumilast in each study.Citation34 When results from the two trials were pooled, a significant reduction (14.3%) in moderate to severe exacerbations was observed compared with placebo (P=0.026).Citation34 Post hoc analyses identified several subgroups of patients that were associated with greater response. In particular, patients receiving concomitant inhaled corticosteroids (ICSs) or short-acting anticholinergics, patients with a history of chronic bronchitis with or without emphysema, and patients with elevated cough or sputum scores at baseline (≥1 average score per day) saw significant reductions in the incidence rate of moderate to severe COPD exacerbations by 18% to 30%.Citation34
The identified patient groups most responsive to roflumilast in the M2-111 and M2-112 studies helped to inform the design of the subsequent M2-124 and M2-125 studies. These trials included patients with COPD aged >40 years with severe airflow limitation, bronchitic symptoms, and a history of exacerbations. In these studies, roflumilast was not only associated with improvements in lung function, but the drug was also associated with a 15% reduction in moderate or severe exacerbations (P=0.0278) in study M2-124 and an 18% reduction in M2-125 (P=0.0035).Citation31 In trials M2-127 and M2-128, roflumilast also significantly improved lung function when combined with salmeterol (M2-127) and tiotropium (M2-128) compared with the use of either agent alone.Citation32
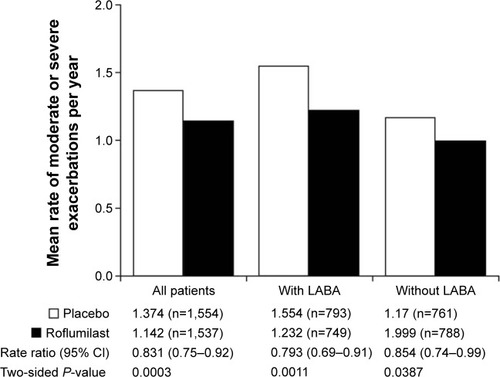
Post hoc analyses of these later trials have evaluated the efficacy of roflumilast in select subgroups of patients, for example, the efficacy of roflumilast in patients who were taking concomitant long-acting β2-agonists (LABAs).Citation38 Moderate to severe exacerbations of COPD were reduced by 20.7% in patients taking roflumilast concomitantly with a LABA (P=0.001) compared with 14.6% in patients taking roflumilast alone (P=0.039) ().Citation38 Roflumilast also prolonged the time to first (P=0.035 with LABA; P=0.300 without LABA) and second COPD exacerbations (P=0.018 with LABA; P=0.049 without LABA).Citation38 Patients who had frequent COPD exacerbations (≥2) in the year prior to treatment with roflumilast saw the greatest reduction versus placebo in the incidence of exacerbations compared with patients who had infrequent exacerbations (22.3% versus 16.5%, respectively; 95% confidence interval [CI]: 9%–34%).Citation38
Figure 2 Effect of roflumilast on the mean rate of moderate or severe exacerbations with or without a LABA.
Abbreviations: CI, confidence interval; LABA, long-acting β2-agonist.
As frequent COPD exacerbations have been associated with increased morbidity and mortality, an additional analysis looked further into endpoints for the frequent exacerbator population of patients. For patients with GOLD severe airway limitation of 3, treatment with roflumilast may help to shift frequent exacerbator patients at baseline to the more stable infrequent exacerbator type.Citation39 After 1 year of treatment, only 26.4% of patients treated with roflumilast who were frequent exacerbators at baseline remained frequent exacerbators compared with 38.9% of patients randomized to placebo (P=0.0042).Citation39 An additional analysis of studies M2-124 and M2-125 demonstrated that roflumilast reduced the rate of severe COPD exacerbations leading to hospitalization compared with placebo (rate ratio [RR] 0.78; 95% CI: 0.62–0.90; P=0.044).Citation40
A post hoc analysis of study M2-128 indicated that roflumilast shows efficacy in patients with highly symptomatic COPD.Citation41 Using the modified Medical Research Council questionnaire, which evaluates the severity of breathlessness, the efficacy of roflumilast in patients with moderate to severe COPD and Grade 2 or higher breathlessness was evaluated. Mean pre- and postbronchodilator FEV1 increased by 79 mL and 78 mL, respectively, compared with placebo (P=0.0002).Citation41 Roflumilast was associated with a 45.5% reduction in moderate to severe exacerbations compared with placebo (P=0.0338).Citation41 The reduction observed in this subgroup of patients with highly symptomatic COPD was greater than the 27% reduction in exacerbations observed in the overall study population.Citation32
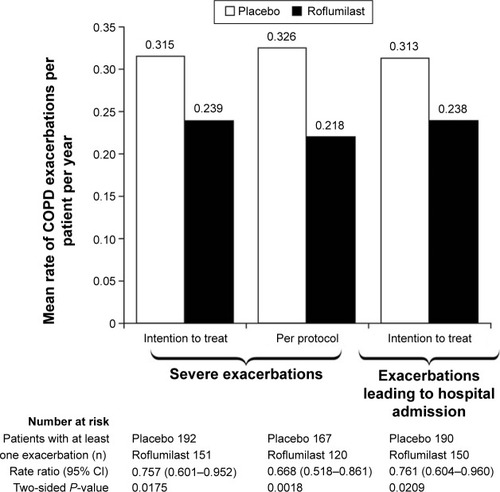
The most recent study was REACT, a Phase III/IV randomized, double-blind, multicenter study designed to investigate whether roflumilast further reduces exacerbations when added to inhaled combination therapy (LABA/ICS) in patients still suffering from frequent exacerbations.Citation42 Patients were randomized to receive roflumilast 500 µg or placebo once daily in combination with a fixed ICS/LABA combination. The rate of moderate to severe COPD exacerbations in the intention-to-treat population (primary endpoint) was 13.2% lower in the roflumilast group versus the placebo group in the Poisson regression analysis (RR 0.868; 95% CI: 0.753–1.002; P=0.0529) and was 14.2% lower in the negative binomial regression analysis (RR 0.858; 95% CI: 0.740–0.995; P=0.0424).Citation35 The benefit was evident irrespective of concomitant use of long-acting antimuscarinic agents. Roflumilast was also superior to placebo for reducing severe events (RR 0.757; 95% CI: 0.601–0.952; P=0.0175) and for reducing exacerbations requiring hospitalization (RR 0.761; 95% CI: 0.604–0.960; P=0.0209) ().Citation35
Figure 3 Mean rate of serious exacerbations or exacerbations leading to hospital admission per patient per year in the REACT study.
Abbreviation: CI, confidence interval.
Quality of life
In the DACOTA (Daxas for COPD therapy; NCT1285167) study, the effects of roflumilast on the quality of life of patients with COPD (N=3,597) were investigated in a non-interventional, real-life cohort study for 6 months.Citation43 Patients were divided into frequent and infrequent exacerbator subpopulations based on their exacerbation history over the 12 months leading up to treatment with roflumilast. Clinical COPD Questionnaire (CCQ) scores (1-week version) and COPD Assessment Test (CAT) scores were used to assess improvements in quality of life. The minimal clinically important difference thresholds for CCQ and CAT scores demonstrating improvement in quality of life are 0.41 and 2.0, respectively.Citation44,Citation45 At the end of 12 months, both subpopulations showed significant improvements from baseline in mean CCQ scores with roflumilast treatment (P<0.001), with greater improvements seen for frequent exacerbators compared with infrequent exacerbators (−1.00 versus −0.73, respectively; P<0.001).Citation43 Similar results were shown for CAT scores, with significant improvements from baseline scores observed in both subpopulations (P<0.001) and significantly greater improvements in frequent exacerbators compared with infrequent exacerbators (−6.62 versus −4.91; P<0.001).Citation43 An earlier study also demonstrated that treatment with roflumilast improved health-related quality of life as assessed by the St George’s Respiratory Questionnaire total score.Citation33 In this study, roflumilast showed greater improvement in health-related quality of life than placebo, although the difference was not statistically significant.
Cost effectiveness
Both COPD treatment and COPD exacerbations have an economic impact on health care systems. The total direct costs related to COPD in the USA and Europe are 53.7 billion dollars ($) (COPD/asthma combined)Citation46 and 23 billion euros (£), respectively.Citation47 Using claims data from the United Kingdom National Health Service, a Markov cohort model was developed to evaluate the total costs, life-years, and quality-adjusted life-years of COPD exacerbations related to different COPD regimens.Citation48 Roflumilast was found to be generally cost effective when added on to standard-of-care therapy. Roflumilast added on to a regimen of tiotropium and salmeterol resulted in an incremental cost-effectiveness ratio of £13,764/quality-adjusted life-year gained. When added on to a regimen of tiotropium and salmeterol/fluticasone, the result was £16,566/quality-adjusted life-year gained.Citation48 Similar findings were observed for a cost-effectiveness analysis comparing roflumilast added on to tiotropium versus tiotropium alone. Roflumilast was found to be cost effective as add-on therapy over a period of 5 years ($15,815/quality-adjusted life-year).Citation49 Economic analyses of data from the REACT study will provide additional data on the cost effectiveness of roflumilast when used in combination with LABA/ICS.
Tolerability
Roflumilast is generally well tolerated with adverse events (AEs) consistent with those expected for PDE4 inhibitors. Combining the data from several 1-year and 6-month clinical trials of roflumilast (N=8,630), the most common AEs were gastrointestinal disorders (diarrhea and nausea) and weight loss ().Citation50 Other AEs that occurred with greater frequency compared with placebo were back pain, insomnia, and decreased appetite. In another pooled safety analysis that included data from 14 intermediate- and long-term placebo-controlled clinical trials of roflumilast (N=12,054), the rates of AEs (67.2% versus 62.8%) and severe AEs (13.5% versus 14.2%) were found to be near similar compared with placebo.Citation51 Rates of infection (25.9% versus 27.5%), pneumonia (1.8% versus 2.0%), and cardiovascular AEs (5.2% versus 5.7%) were also similar.Citation51 In the REACT trial, AEs were reported by 67% of those receiving roflumilast compared with 59% of the placebo group, with serious AEs reported in 26% and 30%, respectively. However, there were more discontinuations due to AEs among those receiving roflumilast (n=82) versus placebo (n=29).Citation35
Table 2 Adverse reactions (≥2%) associated with roflumilast from four 1-year placebo-controlled trials and four 6-month trials
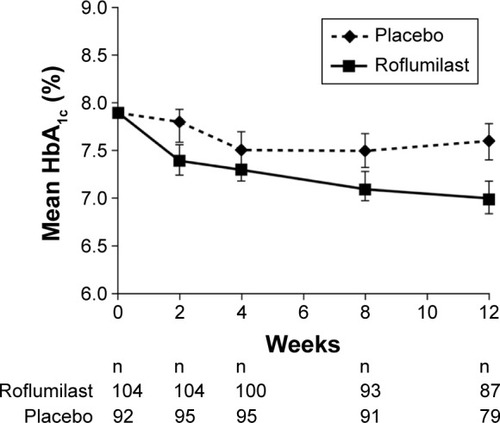
A common systemic effect of COPD is weight loss, which can be seen in patients with severe COPD.Citation21,Citation52 Both selective and nonselective PDE inhibitors have been associated with weight loss,Citation37 which may be related to the effects of increased cAMP on signaling pathways that regulate lipolysis.Citation53 Weight loss in one pooled analysis was found to be 2.14 kg greater with roflumilast treatment compared with placebo (P<0.0001).Citation51 The extent of weight loss was mostly realized within the first 4 weeks of treatment and was shown to occur in patients with greater fat mass. After discontinuing roflumilast, patients regained one-half of their lost weight within 3 months.Citation51 Animal models suggest that PDE4 inhibitors may also increase glucagon-like peptide-1 levels.Citation54 Glucagon-like peptide-1 receptor agonists are used in the treatment of diabetes and are also associated with weight loss.Citation55 This may serve as another possible explanation for the weight loss seen in patients with COPD treated with roflumilast and could also explain favorable effects on glycemic parameters as well as the gastrointestinal AEs (nausea and diarrhea) associated with the drug. In a 12-week, placebo-controlled trial in patients with newly diagnosed type 2 diabetes mellitus, roflumilast increased insulin sensitivity and was associated with a significantly greater change in glycated hemoglobin than placebo (least-square mean =−0.45%; P<0.0001) ().Citation56
Figure 4 Changes in mean glycated hemoglobin (HbA1c) levels over 12 weeks in patients with newly diagnosed, treatment-naïve type 2 diabetes mellitus.
Cardiovascular safety
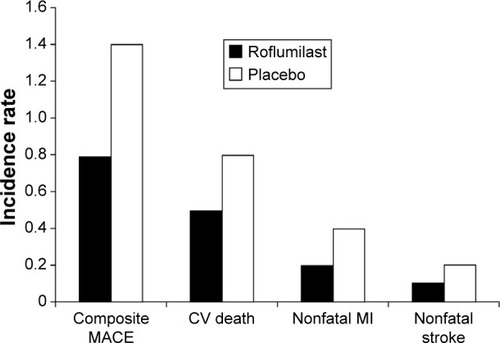
Patients diagnosed with COPD are approximately 3 and 3.5 times more likely to experience a stroke and acute myocardial infarction,Citation8 respectively. Thus, the effect of COPD treatment on cardiovascular safety is a concern for both clinicians and patients. Using the same pooled safety data for previous analyses described (N=12,054), the potential major adverse cardiovascular events (eg, composite of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke) were assessed in patients randomized to receive roflumilast ().Citation57 Roflumilast was associated with a significantly lower risk of major adverse cardiovascular events versus placebo-treated patients: 14.3 per 1,000 versus 22.3 per 1,000 patient-years, respectively (hazard ratio 0.65; 95% CI: 0.45–0.93; P=0.019).Citation57
Figure 5 Pooled analysis of the incidence rate of the composite of MACE (nonfatal MI, nonfatal stroke, and CV death) for patients receiving roflumilast (n=6,563) or placebo (n=5,491).
Abbreviations: CV, cardiovascular; MACE, major adverse cardiovascular events; MI, myocardial infarction.
Place in therapy
Treatment goals for patients with active COPD exacerbations include reducing symptoms of current exacerbations and preventing further episodes. The relationship between the development of exacerbations and disease progression and morbidity and mortality in patients with COPD underscores the importance of prevention and risk reduction. In addition, frequent exacerbators are a distinct clinical subgroup who are at high risk and need close management.Citation10,Citation58 For the management of stable COPD, guidelines generally recommend the regular use of an inhaled LABA and ICS, alone or in combination, for patients with moderate to severe COPD with recurrent exacerbations.Citation21,Citation22 Additionally, preventative measures such as vaccination, smoking cessation, and reeducation on inhaler technique are also recommended. Pulmonary rehabilitation, including exercise training, education, psychosocial/behavioral intervention, and nutritional therapy, can also reduce exacerbations.Citation21
While treatment with LABAs and ICS are associated with reductions in exacerbations, patients still suffer from these episodes over time.Citation58 In addition, long-term ICS therapy may be associated with an increased risk of pneumonia. Data from the INSPIRE (Investigating New Standards for Prophylaxis in Reducing Exacerbations; NCT0361959) study indicated that pneumonia was more common among patients receiving ICS therapy, with the risk apparently related to protracted symptomatic exacerbations.Citation59 One retrospective analysis of a patient claims database indicated an increased pneumonia risk of 38%, 69%, and 157% for patients taking low-dose (<500 µg daily), medium-dose (500–999 µg daily), and high-dose (≥1,000 µg daily) ICS therapy, respectively.Citation60 There appear to be differences between ICS for the risk of pneumonia, with a 73% higher rate of pneumonia among patients receiving fluticasone/salmeterol compared with those receiving budesonide/formoterol.Citation61
Roflumilast is a PDE4 inhibitor with demonstrated efficacy for improving lung function and decreasing exacerbations in patients with severe to very severe COPD associated with chronic bronchitis. This includes decreasing the incidence of exacerbations in frequent exacerbators and also of hospitalization.Citation31,Citation32,Citation34,Citation35 Thus, roflumilast in combination with a LABA with or without an ICS or a long-acting muscarinic antagonist appears to be a reasonable alternative choice for patients with severe to very severe COPD associated with chronic bronchitis and a history of COPD exacerbations. As of now, the benefits of roflumilast are most well established in those with severe disease. A recent benefit/harm analysis of the use of roflumilast in patients with COPD found that only patients with a high risk of severe exacerbations achieved a net benefit from roflumilast therapy.Citation62
Extrapulmonary manifestations of COPD also need to be taken into consideration when managing patients. Recent evidence suggests that COPD has manifestations beyond the respiratory tract, including an increased risk of cardiovascular disease, osteoporosis, diabetes, and anxiety/depression.Citation2,Citation63 One of the key mechanisms underlying these systemic manifestations is low-grade, chronic systemic inflammation, and it is possible that these represent a common pathophysiology or at least shared risk factors. Data supporting this include the observation that roflumilast decreases the risk of cardiovascular events in patients with COPDCitation57 and that the drug improves glucose homeostasis in patients with type 2 diabetes mellitus.Citation56 Thus, the current target population for the use of roflumilast is patients at high risk who have a higher risk for exacerbations, COPD hospitalization, and death.Citation64
Additional trials are underway to further define the role of roflumilast for targeting the underlying systemic inflammation associated with COPD. Another ongoing trial (Trial to Assess the Anti-inflammatory Effects of Roflumilast in COPD; NCT1509677) is evaluating the effect of roflumilast 500 µg versus placebo on inflammation parameters in bronchial biopsy tissue specimens in patients with moderate to severe COPD associated with chronic bronchitis.Citation65
In summary, clinical efficacy, quality of life, and cost-effectiveness data suggest that roflumilast can be an important and cost-effective alternative to ICS in the prevention of exacerbations, particularly for patients with severe to very severe COPD associated with chronic bronchitis and a history of exacerbations.
Acknowledgments
Bret Fulton, RPh; Maria McGill, RPh, CMPP; and Robert Schupp, PharmD, of inScience Communications, Springer Healthcare provided medical writing support funded by Takeda Pharmaceuticals International. The development of this manuscript was supported by Takeda Pharmaceuticals North America, Inc.
Disclosure
JAW has participated in advisory board meetings and/or spoken at meetings for GlaxoSmithKline, Pfizer, Takeda, Boehringer Ingelheim, AstraZeneca, Johnson & Johnson, Napp Pharmaceuticals Limited, Vifor Pharma, and Novartis. PMAC has advised on study conduct and spoken at meetings sponsored by GlaxoSmithKline, Boehringer Ingelheim, AstraZeneca, Novartis, and Takeda. KFR has received research support for serving as an investigator from Altana Pharma, Novartis, Astra-Zeneca, Merck Sharp & Dohme, and Nycomed. The authors report no other conflicts of interest in this work.
References
- AgustiAGCOPD, a multicomponent disease: implications for managementRespir Med200599667068215878483
- Global Initiative for Chronic Obstructive Lung Disease (GOLD)Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease2014 Available from: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2014_Jan23.pdfAccessed July 28, 2015
- GanWQManSFSenthilselvanASinDDAssociation between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysisThorax200459757458015223864
- FabbriLMRabeKFFrom COPD to chronic systemic inflammatory syndrome?Lancet2007370958979779917765529
- HoggJCChuFUtokaparchSThe nature of small-airway obstruction in chronic obstructive pulmonary diseaseN Engl J Med2004350262645265315215480
- SaettaMAirway inflammation in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med19991605 Pt 2S17S2010556163
- DonaldsonGCHurstJRSmithCJHubbardRBWedzichaJAIncreased risk of myocardial infarction and stroke following exacerbation of COPDChest201013751091109720022970
- FearyJRRodriguesLCSmithCJHubbardRBGibsonJEPrevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary careThorax2010651195696220871122
- StällbergBJansonCJohanssonGManagement, morbidity and mortality of COPD during an 11-year period: an observational retrospective epidemiological register study in Sweden (PATHOS)Prim Care Respir J2014231384524346825
- WedzichaJABrillSEAllinsonJPDonaldsonGCMechanisms and impact of the frequent exacerbator phenotype in chronic obstructive pulmonary diseaseBMC Med20131118123945277
- PeacockJLAndersonHRBremnerSAOutdoor air pollution and respiratory health in patients with COPDThorax201166759159621459856
- SethiSMurphyTFInfection in the pathogenesis and course of chronic obstructive pulmonary diseaseN Engl J Med2008359222355236519038881
- BathoornELieskerJJPostmaDSChange in inflammation in outpatient COPD patients from stable phase to a subsequent exacerbationInt J Chron Obstruct Pulmon Dis2009410110919436694
- HurstJRDonaldsonGCPereraWRUse of plasma biomarkers at exacerbation of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2006174886787416799074
- MalliaPMessageSDGielenVExperimental rhinovirus infection as a human model of chronic obstructive pulmonary disease exacerbationAm J Respir Crit Care Med2010183673474220889904
- TkacovaRKluchovaZJoppaPPetrasovaDMolcanyiovaASystemic inflammation and systemic oxidative stress in patients with acute exacerbations of COPDRespir Med200710181670167617449234
- SeemungalTADonaldsonGCPaulEABestallJCJeffriesDJWedzichaJAEffect of exacerbation on quality of life in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med19981575 Pt 1141814229603117
- SeneffMGWagnerDPWagnerRPZimmermanJEKnausWAHospital and 1-year survival of patients admitted to intensive care units with acute exacerbation of chronic obstructive pulmonary diseaseJAMA199527423185218577500534
- Soler-CatalunaJJMartinez-GarciaMARoman SanchezPSalcedoENavarroMOchandoRSevere acute exacerbations and mortality in patients with chronic obstructive pulmonary diseaseThorax2005601192593116055622
- SuissaSDell’AnielloSErnstPLong-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortalityThorax2012671195796322684094
- American Thoracic Society/European Respiratory SocietyStandards for the diagnosis and management of patients with COPD2004 Available from: http://www.thoracic.org/copd-guidelines/resources/copddoc.pdfAccessed January 23, 2015
- QaseemAWiltTJWeinbergerSEDiagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory SocietyAnn Intern Med2011155317919121810710
- Daliresp (roflumilast) tablets [package insert]Wilmington, DEAstra-Zeneca Pharmaceuticals LP2015
- HatzelmannAMorcilloEJLungarellaGThe preclinical pharmacology of roflumilast – a selective, oral phosphodiesterase 4 inhibitor in development for chronic obstructive pulmonary diseasePulm Pharmacol Ther201023423525620381629
- SanzMJCortijoJMorcilloEJPDE4 inhibitors as new anti-inflammatory drugs: effects on cell trafficking and cell adhesion molecules expressionPharmacol Ther2005106326929715922015
- GrootendorstDCGauwSAVerhooselRMReduction in sputum neutrophil and eosinophil numbers by the PDE4 inhibitor roflumilast in patients with COPDThorax200762121081108717573446
- GauvreauGMBouletLPSchmid-WirlitschCRoflumilast attenuates allergen-induced inflammation in mild asthmatic subjectsRespir Res20111214022029856
- SchickMAWunderCWollbornJPhosphodiesterase-4 inhibition as a therapeutic approach to treat capillary leakage in systemic inflammationJ Physiol2012590Pt 112693270822495586
- HermannRNassrNLahuGSteady-state pharmacokinetics of roflumilast and roflumilast N-oxide in patients with mild and moderate liver cirrhosisClin Pharmacokinet200746540341617465639
- WestphalJFMacrolide-induced clinically relevant drug interactions with cytochrome P-450A (CYP) 3A4: an update focuses on clarithromycin, azithromycin and dirithromycinBr J Clin Pharmacol200050428529511012550
- CalverleyPMRabeKFGoehringUMKristiansenSFabbriLMMartinezFJRoflumilast in symptomatic chronic obstructive pulmonary disease: two randomised clinical trialsLancet2009374969168569419716960
- FabbriLMCalverleyPMIzquierdo-AlonsoJLRoflumilast in moderate-to-severe chronic obstructive pulmonary disease treated with long-acting bronchodilators: two randomised clinical trialsLancet2009374969169570319716961
- RabeKFBatemanEDO’DonnellDWitteSBredenbrökerDBethkeTDRoflumilast – an oral anti-inflammatory treatment for chronic obstructive pulmonary disease: a randomised controlled trialLancet2005366948556357116099292
- RennardSICalverleyPMGoehringUMBredenbrökerDMartinezFJReduction of exacerbations by the PDE4 inhibitor roflumilast – the importance of defining different subsets of patients with COPDRespir Res2011121821272339
- MartinezFJCalverleyPMAGoehringUMBroseMFabbriLMRabeKFEffect of roflumilast on exacerbations in patients with severe chronic obstructive pulmonary disease uncontrolled by combination therapy (REACT): a multicentre randomised controlled trialLancet2015385997185786625684586
- ZhengJYangJZhouXRoflumilast for the treatment of COPD in an Asian population: a randomized, double-blind, parallel-group studyChest20141451445224135893
- RabeKFUpdate on roflumilast, a phosphodiesterase 4 inhibitor for the treatment of chronic obstructive pulmonary diseaseBr J Pharmacol20111631536721232047
- BatemanEDRabeKFCalverleyPMRoflumilast with long-acting β2-agonists for COPD: influence of exacerbation historyEur Respir J201138355356021737553
- WedzichaJARabeKFMartinezFJEfficacy of roflumilast in the COPD frequent exacerbator phenotypeChest201314351302131123117188
- BatemanEDJardimJGoehringUMBroseMCalverlyPEffect of roflumilast on hospitalizations in COPD patientsEur Resp J201240Suppl 56P2109
- FabbriLGoehringUMBroseMRabeKEffects of roflumilast in highly symptomatic COPD patientsEur Resp J201240Suppl 56P742
- CalverleyPMMartinezFJFabbriLMGoehringUMRabeKFDoes roflumilast decrease exacerbations in severe COPD patients not controlled by inhaled combination therapy? The REACT study protocolInt J Chron Obstruct Pulmon Dis2012737538222791991
- KardosPMakrosIVogelmeierCEffects of roflumilast on quality of life in frequent and infrequent exacerbatorsEur Resp J201342Suppl 57P4150
- KocksJWTuinengaMGUilSMvan den BergJWStåhlEvan der MolenTHealth status measurement in COPD: the minimal clinically important difference of the clinical COPD questionnaireRespir Res200676216603063
- JonesPWBrusselleGDal NegroRWProperties of the COPD assessment test in a cross-sectional European studyEur Respir J2011381293521565915
- National Institutes of Health National Heart, Lung, and Blood InstituteMorbidity and Mortality: 2012 Chart Book on Cardiovascular, Lung, and Blood DiseasesBethesda, MDNational Institutes of Health2012 Available from: http://www.nhlbi.nih.gov/files/docs/research/2012_ChartBook.pdfAccessed January 23, 2015
- European Lung White BookThe Economic Burden of Lung DiseaseSheffieldEuropean Lung White Book2014 Available from: http://www.erswhitebook.org/chapters/the-economic-burden-of-lung-disease/Accessed January 23, 2015
- HertelNKotchieRWSamyshkinYRadfordMHumphreysSJamesonKCost-effectiveness of available treatment options for patients suffering from severe COPD in the UK: a fully incremental analysisInt J Chron Obstruct Pulmon Dis2012718319922500119
- SunSXMarynchenkoMBanerjeeRCost-effectiveness analysis of roflumilast/tiotropium therapy versus tiotropium monotherapy for treating severe-to-very severe COPDJ Med Econ201114680581521992217
- MichalskiJMGoldenGIkariJRennardSIPDE4: a novel target in the treatment of chronic obstructive pulmonary diseaseClin Pharmacol Ther201291113414222130119
- CalverleyPMAFabbriLMRabeKFMosbergHRoflumilast in the treatment of COPD: a pooled safety analysisEur Respir J201036Suppl 54 Abstract P4001
- ScholsAMSlangenJVolovicsLWoutersEFWeight loss is a reversible factor in the prognosis of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med19981576 Pt 1179117979620907
- OmarBZmuda-TrzebiatowskaEManganielloVGöranssonODegermanERegulation of AMP-activated protein kinase by cAMP in adipocytes: roles for phosphodiesterases, protein kinase B, protein kinase A, Epac and lipolysisCell Signal200921576076619167487
- OngWKGribbleFMReimannFThe role of the PDE4D cAMP phosphodiesterase in the regulation of glucagon-like peptide-1 releaseBr J Pharmacol2009157463364419371330
- DavidsonJAIncretin-based therapies: focus on effects beyond glycemic control aloneDiabetes Ther20134222123824057947
- WoutersEFBredenbrokerDTeichmannPEffect of the phosphodiesterase 4 inhibitor roflumilast on glucose metabolism in patients with treatment-naive, newly diagnosed type 2 diabetes mellitusJ Clin Endocrinol Metab2012979E1720E172522723325
- WhiteWBCookeGEKoweyPRCardiovascular safety in patients receiving roflumilast for the treatment of COPDChest2013144375876523412642
- HurstJRVestboJAnzuetoASusceptibility to exacerbation in chronic obstructive pulmonary diseaseN Engl J Med2010363121128113820843247
- CalverleyPMStockleyRASeemungalTAINSPRIE InvestigatorsReported pneumonia in patients with COPD: findings from the INSPIRE studyChest2011139350551220576732
- YawnBPLiYTianHZhangJArconaSKahlerKHInhaled corticosteroid use in patients with chronic obstructive pulmonary disease and the risk of pneumonia: a retrospective claims data analysisInt J Chron Obstruct Pulmon Dis2013829530423836970
- JansonCLarssonKLisspersKHPneumonia and pneumonia related mortality in patients with COPD treated with fixed combinations of inhaled corticosteroid and long acting β2 agonist: observational matched cohort study (PATHOS)BMJ2013346f330623719639
- YuTFainKBoydCMBenefits and harms of roflumilast in moderate to severe COPDThorax20146961662224347460
- Nussbaumer-OchsnerYRabeKFSystemic manifestations of COPDChest2011139116517321208876
- LangePMarottJLVestboJPrediction of the clinical course of chronic obstructive pulmonary disease, using the new GOLD classification: a study of the general populationAm J Respir Crit Care Med20121861097598122997207
- BarnesNCSaettaMRabeKFImplementing lessons learned from previous bronchial biopsy trials in a new randomized controlled COPD biopsy trial with roflumilastBMC Pulmon Med2014149