

Abstract
Purpose
This systematic review aimed to identify the most effective components of interventions to facilitate self-management of health care behaviors for patients with COPD. PROSPERO registration number CRD42011001588.
Methods
We used standard review methods with a systematic search to May 2012 for randomized controlled trials of self-management interventions reporting hospital admissions or health-related quality of life (HRQoL). Mean differences (MD), hazard ratios, and 95% confidence intervals (CIs) were calculated and pooled using random-effects meta-analyses. Effects among different subgroups of interventions were explored including single/multiple components and multicomponent interventions with/without exercise.
Results
One hundred and seventy-three randomized controlled trials were identified. Self-management interventions had a minimal effect on hospital admission rates. Multicomponent interventions improved HRQoL (studies with follow-up >6 months St George’s Respiratory Questionnaire (MD 2.40, 95% CI 0.75–4.04, I2 57.9). Exercise was an effective individual component (St George’s Respiratory Questionnaire at 3 months MD 4.87, 95% CI 3.96–5.79, I2 0%).
Conclusion
While many self-management interventions increased HRQoL, little effect was seen on hospital admissions. More trials should report admissions and follow-up participants beyond the end of the intervention.
Supplementary materials
Figure S1 HRQoL (SGRQ) at final follow-up for comparisons assessing the effects of one additional component of self-management.
Abbreviations: ANCOVA, analysis of covariance; CI, confidence interval; HRQoL, health-related quality of life; SGRQ, St George’s respiratory questionnaire; Int, intervention group; Cont, control group.
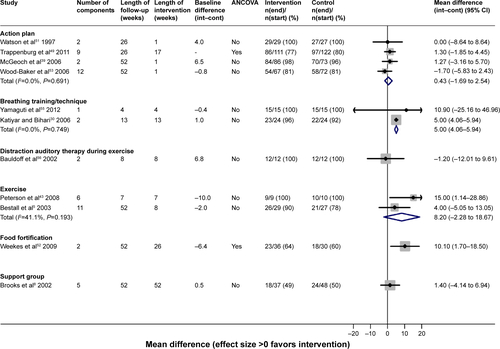
Figure S2 HRQoL (CRQ) at final follow-up for comparisons assessing the effects of one additional component of self-management.
Note: D = rehabilitation (traditional and modern) + qigong + breathing training + limb training vs modern rehabilitation + breathing training + limb training.
Abbreviations: ANCOVA, analysis of covariance; CI, confidence interval; HRQoL, health-related quality of life; CRQ, Chronic Respiratory disease Questionnaire.
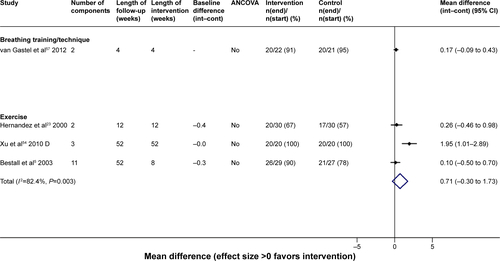
Figure S3 HRQoL (SGRQ) outcomes for exercise-only interventions versus usual care/sham intervention.
Note: *The control group that has been halved in size (split between two comparisons). A = t’ai chi qigong vs control. B = exercise vs control.
Abbreviations: ANCOVA, analysis of covariance; CI, confidence interval; HRQoL, health-related quality of life; SGRQ, St George’s respiratory questionnaire.
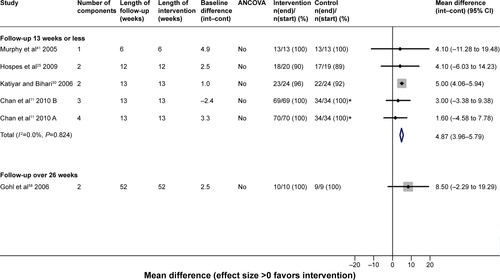
Figure S4 Hospital admissions for multicomponent self-management interventions versus usual care.
Notes: B = exercise vs control. ^Several papers are represented by this lead publication.
Abbreviations: ANCOVA, analysis of covariance; CI, confidence interval; HR, hazard ratio.
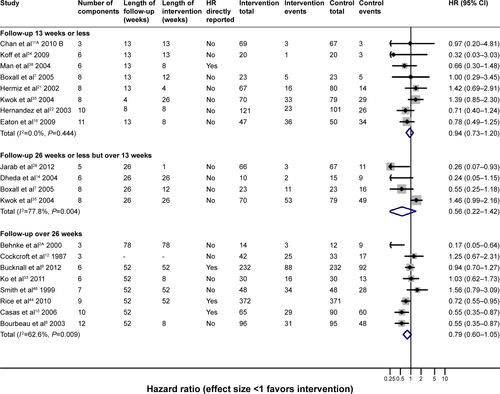
Figure S5 HRQoL (CRQ) outcomes for multicomponent self-management intervention versus usual care.
Note: A = rehabilitation (traditional and modern) + qigong + breathing training + limb training vs UC.
Abbreviations: ANCOVA, analysis of covariance; CI, confidence interval; HRQoL, health-related quality of life; CRQ, Chronic Respiratory disease Questionnaire; UC, usual care.
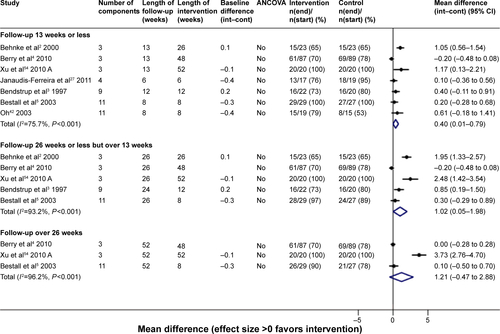
Figure S6 HRQoL (SGRQ) outcomes for multicomponent self-management interventions including supervised exercise versus usual care/control.
Notes: B = exercise vs control. ^Several papers are represented by this lead publication.
Abbreviations: ANCOVA, analysis of covariance; CI, confidence interval; HRQoL, health-related quality of life; SGRQ, St George’s respiratory questionnaire.
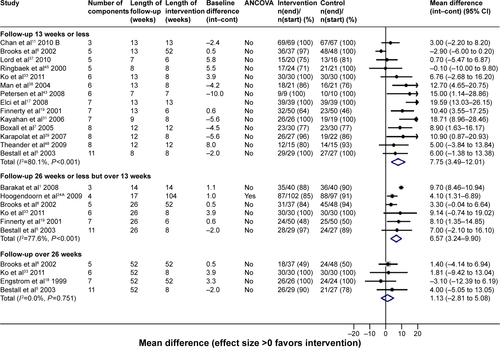
Figure S7 HRQoL (CRQ) outcomes for multicomponent self-management interventions including supervised exercise versus usual care/control.
Note: A = rehabilitation (traditional and modern) + qigong + breathing training + limb training vs UC.
Abbreviations: ANCOVA, analysis of covariance; CI, confidence interval; HRQoL, health-related quality of life; CRQ, Chronic Respiratory disease Questionnaire; UC, usual care.
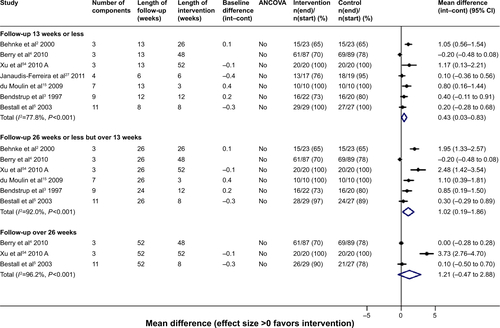
Figure S8 HRQoL (SGRQ) outcomes for multicomponent self-management interventions with structured, unsupervised exercise versus usual care/control.
Abbreviations: ANCOVA, analysis of covariance; CI, confidence interval; HRQoL, health-related quality of life; SGRQ, St George’s respiratory questionnaire.
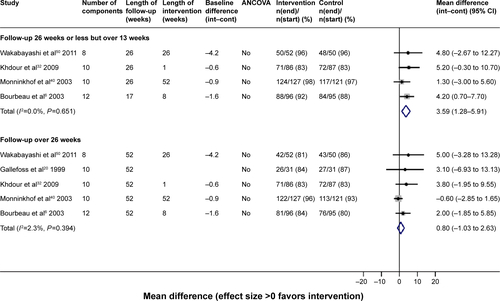
Figure S9 HRQoL (SGRQ) outcomes for multicomponent self-management interventions with exercise counseling only versus usual care/control.
Note: ^Several papers are represented by this lead publication.
Abbreviations: ANCOVA, analysis of covariance; CI, confidence interval; HRQoL, health-related quality of life; SGRQ, St George’s respiratory questionnaire.
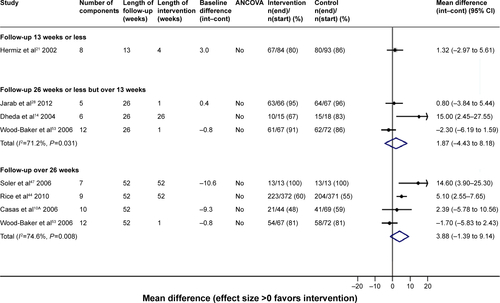
Figure S10 HRQoL (SGRQ) outcomes for multicomponent self-management interventions without an exercise element versus usual care/control.
Notes: *The control group that has been halved in size (split between two comparisons). A = nurse-assisted collaborative management vs UC; B = nurse-assisted medical management vs UC.
Abbreviations: ANCOVA, analysis of covariance; CI, confidence interval; HRQoL, health-related quality of life; SGRQ, St George’s respiratory questionnaire; UC, usual care.
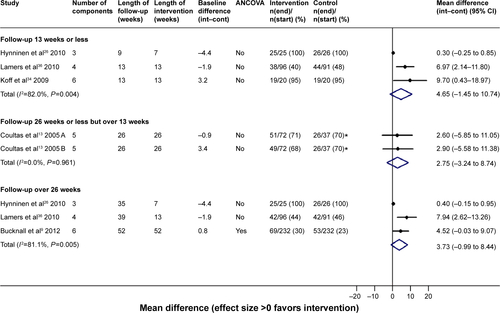
Table S1 Definitions of components of self-management
Table S2 Content of interventions by the number of components within the self-management package
References
- BarakatSMicheleGGeorgePNicoleVGuyAOutpatient pulmonary rehabilitation in patients with chronic obstructive pulmonary diseaseInt J Chron Obstruct Pulmon Dis20083115516218488439
- BehnkeMTaubeCKirstenDLehnigkBJorresRAMagnussenHHome-based exercise is capable of preserving hospital-based improvements in severe chronic obstructive pulmonary diseaseRespir Med200094121184119111192954
- BendstrupKEIngemannJJHolmSBengtssonBOut-patient rehabilitation improves activities of daily living, quality of life and exercise tolerance in chronic obstructive pulmonary diseaseEur Respir J19971012280128069493664
- BerryMJRejeskiWJMillerMEA lifestyle activity intervention in patients with chronic obstructive pulmonary diseaseRespir Med2010104682983920347286
- BestallJCPaulEAGarrodRLongitudinal trends in exercise capacity and health status after pulmonary rehabilitation in patients with COPDRespir Med200397217318012587969
- BourbeauJJulienMMaltaisFReduction of hospital utilization in patients with chronic obstructive pulmonary disease: a disease-specific self-management interventionArch Intern Med2003163558559112622605
- BoxallAMBarclayLSayersACaplanGAManaging chronic obstructive pulmonary disease in the community. A randomized controlled trial of home-based pulmonary rehabilitation for elderly housebound patientsJ Cardiopulm Rehabil200525637838516327534
- BrooksDKripBMangovski-AlzamoraSGoldsteinRSThe effect of postrehabilitation programmes among individuals with chronic obstructive pulmonary diseaseEur Respir J2002201202912166571
- BucknallCEMillerGLloydSMGlasgow supported self-management trial (GSuST) for patients with moderate to severe COPD: randomised controlled trialBMJ2012344e106022395923
- CasasATroostersTGarcia-AymerichJIntegrated care prevents hospitalisations for exacerbations in COPD patientsEur Respir J200628112313016611656
- ChanAWLeeASuenLKTamWWEffectiveness of a Tai chi Qigong program in promoting health-related quality of life and perceived social support in chronic obstructive pulmonary disease clientsQual Life Res201019565366420229333
- CockcroftABagnallPHeslopAControlled trial of respiratory health worker visiting patients with chronic respiratory disabilityBr Med J (Clin Res Ed)19872946566225228
- CoultasDFrederickJBarnettBSinghGWludykaPA randomized trial of two types of nurse-assisted home care for patients with COPDChest200512842017202416236850
- DhedaKCrawfordAHaganGRobertsCMImplementation of British Thoracic Society guidelines for acute exacerbation of chronic obstructive pulmonary disease: Impact on quality of lifePostgrad Med J20048094116917115016940
- du MoulinMTaubeKWegscheiderKBehnkeMvan denBHHome-based exercise training as maintenance after outpatient pulmonary rehabilitationRespiration200977213914518667807
- EatonTYoungPFergussonWDoes early pulmonary rehabilitation reduce acute health-care utilization in COPD patients admitted with an exacerbation? A randomized controlled studyRespirology200914223023819272084
- ElciABorekciSOvayoluNElbekOThe efficacy and applicability of a pulmonary rehabilitation programme for patients with COPD in a secondary-care community hospitalRespirology200813570370718713091
- EngstromCPPerssonLOLarssonSSullivanMLong-term effects of a pulmonary rehabilitation programme in outpatients with chronic obstructive pulmonary disease: a randomized controlled studyScand J Rehabil Med199931420721310599897
- FinnertyJPKeepingIBulloughIJonesJThe effectiveness of outpatient pulmonary rehabilitation in chronic lung disease: a randomized controlled trialChest200111961705171011399694
- GallefossFBakkePSRsgaardPKQuality of life assessment after patient education in a randomized controlled study on asthma and chronic obstructive pulmonary diseaseAm J Respir Crit Care Med1999159381281710051255
- HermizOCominoEMarksGRandomised controlled trial of home based care of patients with chronic obstructive pulmonary diseaseBMJ2002325737093812399344
- HernandezCCasasAEscarrabillJHome hospitalisation of exacerbated chronic obstructive pulmonary disease patientsEur Respir J2003211586712570110
- HernandezMTRubioTMRuizFOResults of a home-based training program for patients with COPDChest2000118110611410893367
- HoogendoornMvan WeteringCRScholsAMRutten-van MolkenMPSelf-report versus care provider registration of healthcare utilization: impact on cost and cost-utilityInt J Technol Assess Health Care200925458859519845991
- HospesGBossenbroekLTen HackenNHvanHPde GreefMHEnhancement of daily physical activity increases physical fitness of outclinic COPD patients: results of an exercise counseling programPatient Educ Couns200975227427819036552
- HynninenMJBjerkeNPallesenSBakkePSNordhusIHA random-ized controlled trial of cognitive behavioral therapy for anxiety and depression in COPDRespir Med2010104798699420346640
- Janaudis-FerreiraTHillKGoldsteinRSResistance arm training in patients with COPD: A Randomized Controlled TrialChest2011139115115820724740
- JarabASAlqudahSGKhdourMShamssainMMukattashTLImpact of pharmaceutical care on health outcomes in patients with COPDInt J Clin Pharm2012341536222101426
- KarapolatHAtaseverAAtamazFDo the benefits gained using a short-term pulmonary rehabilitation program remain in COPD patients after participation?Lung2007185422122517487535
- KatiyarSKBihariSRole of pranayama in rehabilitation of copd patients – a randomized controlled studyIndian Journal of Allergy Asthma Immunology200620298104
- KayahanBKarapolatHAtyntoprakEAtaseverAOzturkOPsychological outcomes of an outpatient pulmonary rehabilitation program in patients with chronic obstructive pulmonary diseaseRespir Med200610061050105716253496
- KhdourMRKidneyJCSmythBMMcElnayJCClinical pharmacyled disease and medicine management programme for patients with COPDBr J Clin Pharmacol200968458859819843062
- KoFWDaiDLNgaiJEffect of early pulmonary rehabilitation on health care utilization and health status in patients hospitalized with acute exacerbations of COPDRespirology201116461762421199163
- KoffPBJonesRHCashmanJMVoelkelNFVandivierRWProactive integrated care improves quality of life in patients with COPDEur Respir J20093351031103819129289
- KwokTLumCMChanHSMaHMLeeDWooJA randomized, controlled trial of an intensive community nurse-supported discharge program in preventing hospital readmissions of older patients with chronic lung diseaseJ Am Geriatr Soc20045281240124615271109
- LamersFJonkersCCBosmaHImproving quality of life in depressed COPD patients: effectiveness of a minimal psychological interventionCOPD20107531532220854045
- LordVMCavePHumeVJSinging teaching as a therapy for chronic respiratory disease – a randomised controlled trial and qualitative evaluationBMC Pulmonary Medicine2010104120682030
- ManWDPolkeyMIDonaldsonNGrayBJMoxhamJCommunity pulmonary rehabilitation after hospitalisation for acute exacerbations of chronic obstructive pulmonary disease: randomised controlled studyBMJ20043297476120915504763
- McGeochGRWillsmanKJDowsonCASelf-management plans in the primary care of patients with chronic obstructive pulmonary diseaseRespirology200611561161816916335
- MonninkhofEvan der ValkPvan der PalenJvan HerwaardenCZielhuisGEffects of a comprehensive self-management programme in patients with chronic obstructive pulmonary diseaseEur Respir J200322581582014621090
- MurphyNBellCCostelloRWExtending a home from hospital care programme for COPD exacerbations to include pulmonary rehabilitationRespir Med200599101297130216140230
- OhEGThe effects of home-based pulmonary rehabilitation in patients with chronic lung diseaseInt J Nurs Stud200340887387914568368
- PetersenAMMittendorferBMagkosFIversenMPedersenBKPhysical activity counteracts increased whole-body protein breakdown in chronic obstructive pulmonary disease patientsScand J Med Sci Sports200818555756418067517
- RiceKLDewanNBloomfieldHEDisease management program for chronic obstructive pulmonary disease: a randomized controlled trialAm J Respir Crit Care Med2010182789089620075385
- RingbaekTJBroendumEHemmingsenLRehabilitation of patients with chronic obstructive pulmonary disease. Exercise twice a week is not sufficient!Respir Med200094215015410714421
- SmithBJAppletonSLBennettPWThe effect of a respiratory home nurse intervention in patients with chronic obstructive pulmonary disease (COPD)Aust N Z J Med199929571872510630654
- SolerJJMartinez-GarciaMARomanPEffectiveness of a specific program for patients with chronic obstructive pulmonary disease and frequent exacerbations]. [SpanishArchivos de Bronconeumologia2006421050150817067516
- TheanderKJakobssonPJorgensenNUnossonMEffects of pulmonary rehabilitation on fatigue, functional status and health perceptions in patients with chronic obstructive pulmonary disease: a randomized controlled trialClinical Rehabilitation200923212513619164400
- TrappenburgJCMonninkhofEMBourbeauJEffect of an action plan with ongoing support by a case manager on exacerbation-related outcome in patients with COPD: a multicentre randomised controlled trialThorax2011661197798421785156
- WakabayashiRMotegiTYamadaKEfficient integrated education for older patients with chronic obstructive pulmonary disease using the Lung Information Needs QuestionnaireGeriatr Gerontol Int201111442243021447136
- WatsonPBTownGIHolbrookNEvaluation of a self-management plan for chronic obstructive pulmonary diseaseEur Respir J1997106126712719192927
- WeekesCEEmeryPWEliaMDietary counselling and food fortification in stable COPD: a randomised trialThorax200964432633119074931
- Wood-BakerRMcGloneSVennAWaltersEHWritten action plans in chronic obstructive pulmonary disease increase appropriate treatment for acute exacerbationsRespirology200611561962616916336
- XuY-HWangJ-HLiH-FEfficacy of integrative respiratory rehabilitation training in exercise ability and quality of life of patients with chronic obstructive pulmonary disease in stable phase: A ran-domized controlled trial. [Chinese]Journal of Chinese Integrative Medicine20108543243720456841
- YamagutiWPClaudinoRCNetoAPDiaphragmatic breathing training program improves abdominal motion during natural breathing in patients with chronic obstructive pulmonary disease: a randomized controlled trialArchives of Physical Medicine & Rehabilitation201293457157722464088
- BauldoffGSHoffmanLAZulloTGSciurbaFCExercise maintenance following pulmonary rehabilitation: effect of distractive stimuliChest2002122394895412226037
- Van GestelAJKohlerMSteierJTeschlerSRussiEWTeschlerHThe effects of controlled breathing during pulmonary rehabilitation in patients with COPDRespiration2012832011512421474911
- GohlOLinzHSchonlebenTOtteBWeineckJWorthHBenefits of a multimodular outpatient training program for patients with COPDPneumologie2006609529536 [Erratum published in Pneumologie. 2006;60(12):783]German17006787
Acknowledgments
The authors thank Simon Stevens for his administrative support. All the people who kindly gave their time to help translate articles are as follows: Yumiko Akiya, Dom Barkos, Susan Bayliss, Matthew Blackburn, Yumi Chen, Jennifer Choi, Karin Diaconu, Janine Dretzke, Maxwell Feltham, Ditte Hedegaard, Boris Kysela, Antje Lindenmeyer, Kinga Malottki, Cristina Peñaloza, and Amanda Zhang.
Disclosure
AMT reports grants from University of Birmingham/National Institute for Health Research (NIHR), during the conduct of the study; REJ was in receipt of an NIHR postdoctoral research fellowship (pdf/01/2008/023) during the conduct of the study; KJ, DAF, REJ, PA, and SJS are investigators on an NIHR SPCR funded trial of self-management for COPD; SJS reports that the University Hospitals of Leicester National Health Service trust holds the IP for a self-management manual for COPD. REJ was funded by NIHR Health Technology Assessment Programme (10/44/01). KJ is part-funded by the National Institute for Health Research (NIHR) Collaborations for Leadership in Applied Health Research and Care (CLAHRC) West Midlands. SJS is part-funded by the CLAHRC-East Midlands. Malcolm Price was supported by funding from a multivariate meta-analysis grant from the MRC Methodology Research Programme (grant reference number: MR/J013595/1). The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Health Technology Assessment programme, NIHR, National Health Service, or the Department of Health. Any errors are the responsibility of the authors. The other authors report no other conflicts of interest in this work.
Author contributions
KJ and REJ conceived the study, KJ, REJ, RDR, PA, DAF, and DJM contributed to the protocol, SEB advised on and performed search strategies, KJ, SM, REJ, NRH, DJM, PA, and AMT contributed to study selection, SM led the development of a risk of bias and data extraction tools, SM, NRH, and EJB extracted results, SM, EJB, NRH, DJM, and KJ undertook the risk of bias assessment, SM, MJP, and RDR coordinated and undertook some data extraction and/or calculation of effect estimates, RDR advised on statistical and reviewing methods and supervised statistical analyses, AJS undertook the statistical analyses, KJ oversaw the analyses, SJS, DAF, and AMT provided clinical input, KJ with input from REJ and RDR wrote and edited the paper. All authors contributed to the paper and commented on the final version.