
Abstract
Background
Arginine silicate inositol complex (ASI; arginine 49.5%, silicon 8.2%, and inositol 25%) is a novel material that is a bioavailable source of silicon and arginine. ASI offers potential benefits for vascular and bone health.
Objective
The aim of this study was to evaluate the potential effects of ASI complex on bone healing of critical-sized defects in rats.
Methods
The rats were randomly assigned to two groups of 21 rats each. The control group was fed a standard diet for 12 weeks; after the first 8 weeks, a calvarial critical-sized defect was created, and the rats were sacrificed 7, 14, and 28 days later. The ASI group was fed a diet containing 1.81 g/kg of ASI for 12 weeks; after the first 8 weeks, a calvarial critical-sized defect was created, and the rats were sacrificed 7, 14, and 28 days later. The calvarial bones of all the rats were then harvested for evaluation.
Results
Osteoblasts and osteoclasts were detected at higher levels in the ASI group compared with the control group at days 7, 14, and 28 of the calvarial defect (P<0.05). New bone formation was detected at higher levels in the ASI group compared with the controls at day 28 (P<0.05). However, new bone formation was not detected at days 7 and 14 in both the groups (P>0.05).
Conclusion
ASI supplementation significantly improved bone tissue healing in rats with critical-sized defects. This study demonstrated that ASI can enhance bone repair and has potential as a therapeutic regimen in humans.
Introduction
Loss and defects of jaw bone can stem from trauma, tooth loss, cancer surgery, congenital anomalies, periodontal disease, and oral-maxillofacial pathologies.Citation1,Citation2 Regeneration of bone defects is a long healing process, requiring recruitment and differentiation of new bone cells. Various graft materials are used to restore bone defects, but they are prone to failure. Several dietary supplements have been explored for their ability to enhance bone regeneration, such as calcium, vitamin D, and alpha lipoic acid.Citation1,Citation3 Recent studies suggest that dietary arginine and silicon may play important roles in the development, growth, and modeling of long bones.Citation4 Arginine is involved both in the synthesis of substrates implicated in collagen synthesis and in the production of growth hormone, insulin-like growth factor (IGF)-1, and nitric oxide.Citation5–Citation7 Arginine is clinically suggested for metabolic disturbances in calcium absorption, growth, dentition and ossification defects, rachitism, osteomalacia, decalcification, and convalescence.Citation8,Citation9 Several roles for silicon have been defined, largely on the basis of animal studies.Citation10,Citation11 Its most important functions appear to be involved in the growth and development of bone, cartilage, and connective tissue. There is a direct relationship between silicon and calcium; it has been reported that silicon is associated with calcium at an early stage of bone formation.Citation12,Citation13 In addition, silicon appears to be required for the synthesis of collagen, the protein matrix found in connective tissue and cartilage, and which is the single most abundant protein in the human body.Citation12
Arginine silicate inositol complex (ASI; arginine 49.5%, silicon 8.2%, and inositol 25%) is a novel, bioavailable source of silicon and arginine and has potential benefits for vascular and bone health.Citation14–Citation17 Several studies support the safety of the components of the ASI complex, with clinical studies demonstrating no adverse effects following the administration of arginine.Citation14–Citation19 Similarly, no adverse effects were observed following the administration of inositol 12 g/day for 4 weeks or of silicon 45 mg/day for 31 days.Citation16,Citation20,Citation21 The ASI complex is absorbed efficiently, raises plasma arginine levels, and is biologically more effective than the arginine from arginine hydrochloride.Citation14,Citation15 The roles of arginine and silicon alone in bone metabolism, osteoporosis, and connective tissue collagen metabolism are well documented, but information about the effects of ASI complex supplementation on bone tissue healing is limited. Therefore, the purpose of this study is to examine the effects of ASI complex supplementation on the healing of calvarial bone tissue defects in rats.
Materials and methods
A total of 42 female Sprague-Dawley rats were used. Their average body weights were 230–280 g on the first day of the experiment. The animals were kept in temperature-controlled cages, exposed to a 12/12-hour light/dark cycle, and had ad libitum access to food and water. The experimental design and study protocol (protocol number: 2015/25) were approved by the animal ethics committee at the University of Dicle. The Helsinki Declaration for laboratory animal care guidelines was strictly obeyed. The rats were randomly divided into two groups of 21 each. The control group was fed a normal diet for 12 weeks; after the first 8 weeks, a calvarial critical-sized defect was created, and the rats were sacrificed 7, 14, and 28 days later. The ASI group was given dietary ASI complex for 12 weeks; after the first 8 weeks, a calvarial critical-sized defect was created, and the rats were sacrificed 7, 14, and 28 days later. A dose of 1.81 g/kg was chosen based on a previous rodent study.Citation15
To create the calvarial defects, general anesthesia was administered using ketamine, and the surgical operations were performed under sterile conditions, after the skull skin was shaved. A skin incision was made on the skull over the linea media. A periosteal elevator was used to lift the flap and periosteum to reach the skull bone. The skull skin was sutured with 4/0 polyglactin resorbable sutures. Cephalosporin antibiotics and an analgesic were injected intramuscularly into all animals after the operation. After 7, 14, and 28 days, the rats were sacrificed by anesthetic overdose. A surgical drill attached to an electrical hand motor was used to harvest the calvarial bone. The calvarial bone specimens were then separated from muscles and soft tissues.Citation22
Histologic and histomorphologic analysis
The original defect area and the surrounding tissues were used for histological analysis. The specimens were fixed in 10% formaldehyde for 72 hours and demineralized in 10% formic acid; after this, they were dehydrated, embedded in paraffin wax, and sectioned for hematoxylin and eosin staining for light microscopy analysis. Sections of 6 μm thickness, corresponding to the bone defect area, were evaluated with light microscopy. Osteoblast numbers were scored in the total defect area as follows: 0, no osteoblast cells; 1, osteoblasts seen as mild; and 2, osteoblasts seen as dense. Osteoclast cells were detected visually on histomorphometric analysis. Osteoclast cells with ruffled borders were found in both the groups. Osteoclast morphology was scored as follows: 0, no osteoclasts; 1, mild osteoclasts; and 2, dense osteoclasts. To measure bone formation histologically, lamellar bone tissue formation was detected and scored. Trabeculations and bone marrow in lamellar bone tissue, unlike in old bone, were detected. Bone formation was scored as follows: 0, no bone formation; 1, mild visible bone formation; 2, moderate visible bone formation; and 3, dense visible bone formation. Images of all of the histological specimens were captured with a digital camera attached to a light microscope with original magnification and were saved on a computer. The Olympus imaging system (Olympus Bx51, Light Microscope; Olympus DP71, Imaging System; Olympus, Tokyo, Japan) was used for the histomorphometric analysis.Citation22,Citation23
Statistical analysis
For statistical analysis, SPSS software (version 22) was used (IBM Corporation, Armonk, NY, USA). After the healing period, mean values and standard deviations were calculated. According to homogeneity and normality of data, the Wilcoxon test was used for pairwise comparisons in dependent groups. P-values of <0.05 were considered statistically significant.
Results
During the postsurgical period, healing was uneventful for both the control and the experimental group animals, and there were no complications of inflammatory tissue responses or allergic reactions. As seen in and –, at days 7 and 14, new bone formation was not detected in either group and at day 28, new bone formation in both the groups was increased compared with that at days 7 and 14 (P<0.05). Overall, the mean new bone area in the control group was lower compared with that in the ASI group at day 28 (P<0.05).
Table 1 The effects of ASI on histomorphometric changes
Figure 1 Histopathologic sections of both the groups at 7 days.
Abbreviation: ASI, arginine silicate inositol complex.
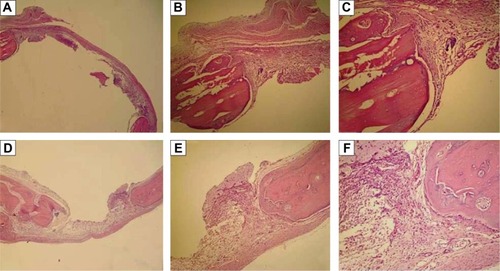
Figure 2 Histopathologic sections of both the groups at 14 days.
Abbreviation: ASI, arginine silicate inositol complex.
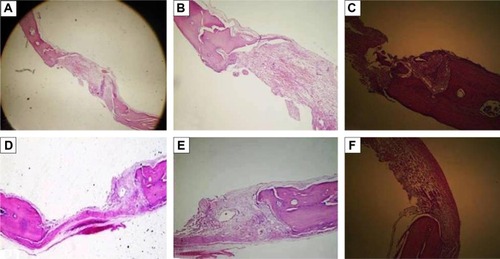
Figure 3 Histopathologic sections of both the groups at 28 days.
Abbreviation: ASI, arginine silicate inositol complex.
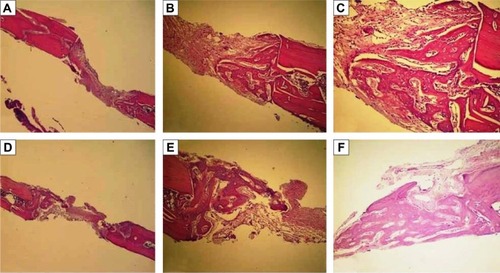
At days 7, 14, and 28, osteoclast numbers were higher in the ASI group compared with those in the control group (P<0.05). At day 7, no statistically significant difference in osteoblast numbers was detected between the two groups (P>0.05). At days 14 and 28, osteoblast numbers were higher in the ASI group compared to the controls (P<0.05) (; –).
The ASI complex used in the present study does not cause adverse effects when administered orally for up to 8 weeks in rats; and it lacks mutagenic potential, as demonstrated in two separate genotoxicity studies.Citation16,Citation17 Rat calvarial defects are considered a preferred experimental model for bone regeneration. For this reason, a 5-mm rat calvarial critical-sized defect model was used, in accordance with previous studies.Citation22,Citation23
In the literature, research is limited with regard to the ASI complex in osteoblastic metabolism, connective tissue and vessel collagen metabolism, and osteoporosis. However, the positive immunological activities of arginine and silicon are well known, and the osteoblastic activity and wound-healing processes in bone and connective tissues are well documented.Citation14–Citation17 Based on the present study, ASI complex supplementation may be an effective material for the treatment of bone tissue defects.
Two components of the product used in the present study, arginine and silicon, can increase osteogenesis.Citation8,Citation12,Citation24 Arginine deficiency may be involved in osteoporosis, fractures, and bone defectsCitation25 and arginine may be involved in the synthesis of polyamine and L-proline (which act as substrates for collagen synthesis) and of growth hormone and IGF, and in nitric oxide production.Citation5–Citation7 Nitric oxide has been shown to prevent corticosteroid-induced bone loss in mature rats.Citation26 Torricelli et alCitation27 reported that arginine in human osteoblasts markedly increased certain parameters called bone-formation markers, such as alkaline phosphatase, nitric oxide, type I collagen, and IGF. These markers increase the synthesis of bone matrix, acting at the cellular level in bone tissue. Torricelli et alCitation27 also reported that the effects of arginine on bone tissue were directly related to the effect on the cell proliferation mechanism. In the same study, IL-6 production was determined to be lower in osteoblasts exposed to arginine.Citation27
Silicon has been implicated as an important component in bone formation, and its deficiency negatively influences skeletal development.Citation11 The primary effect of silicon in bone and cartilage is thought to be on matrix synthesis, although it also has a significant influence on calcification.Citation28 Silicon supplementation inhibits bone resorption and increases trabecular bone volume and bone mineral density in postmenopausal women with osteoporosis.Citation25 Although limited research has been done in vivo, silicon increases osteoblastic activity and decreases osteoclastic activity in vitro.Citation16,Citation17,Citation29 Schroder et alCitation30 and Wiens et alCitation31 reported that osteoprotegerin produced increased osteoblast-like cells exposed to silicate; but no changes occurred in the production of the receptor activator of NF-κB ligand. These researchers stated that the increased osteoprotegerin emission suppressed the receptor activator of NF-κB ligand activity, and consequently increased osteoclastogenesis. Additionally, Sahin et alCitation16 and Önderci et alCitation17 examined the effects of ASI on bone tissue in a study on poultry fed a diet supplemented with 500 mg/kg and 1,000 mg/kg, respectively. In these studies, an increase in the levels of bone mineral density, calcium, and phosphorus in the tibia and of osteocalcin and alkaline phosphatase in the serum, depending on the dose in both the experimental groups compared to the controls, was determined. The findings of the present study confirmed these previous results. In this study, bone formation and bone metabolism associated with bone remodeling and the bone tissue healing process were statistically significantly higher (eg, osteoblast and osteoclast numbers and area of new bone formation) in the ASI-supplemented group compared to the controls. During the bone tissue healing and remodeling process, osteoblasts and osteoclasts act together. These findings also indicate significant positive associations between ASI intake and bone metabolism in the bone tissue defect model used in this experiment.
This study had some limitations. Only the calvarium of the animals were used; however, other skeletal animal parts, for example, long bones (tibia and femur), would be useful for an analysis of the long-bone tissue effects of ASI supplementation. In addition, the histomorphometric method was used for the analysis of the bone tissue effects of ASI, but micro-computerized tomography would be very useful for a better analysis of ASI supplementation in calvarial bones. In addition, the potent anti-inflammatory effects of arginine are well known; however, no research about these effects was made.
Conclusion
Within the limitations of this study, ASI complex could increase bone tissue healing in the rat calvarial critical-sized defect model. Further studies are needed on the effects of ASI complex on bone tissue healing mechanisms and on the effects of new materials on these mechanisms.
Acknowledgments
The authors thank Nutrition 21 Inc (NY, USA) for providing ASI complex. This work was supported in part by the Turkish Academy of Sciences (KS).
Disclosure
The authors report no conflicts of interest in this work. The authors alone are responsible for the content and writing of the paper.
References
- AcarAHYolcuÜAltindişSGülMAlanHMalkoçSBone regeneration by low-level laser therapy and low-intensity pulsed ultrasound therapy in the rabbit calvariumArch Oral Biol201661606526513683
- AkmanSCanakciVKaraATozogluUArabaciTDagsuyuIMTherapeutic effects of alpha lipoic acid and vitamin C on alveolar bone resorption after experimental periodontitis in rats: a biochemical, histochemical, and stereologic studyJ Periodontol201384566667422702517
- ReidIRBristowSMBollandMJCalcium supplements: benefits and risksJ Intern Med2015278435436826174589
- SeabornCDNielsenFHSilicon deprivation decreases collagen formation in wounds and bone, and ornithine transaminase enzyme activity in liverBiol Trace Elem Res200289325126112462748
- ChevalleyTRizzoliRManenDCaverzasioJBonjourJPArginine increases insulin-like growth factor-I production and collagen synthesis in osteoblast-like cellsBone19982321031099701468
- TrippelSBPotential role of insulin-like growth factors in fracture healingClin Orthop Relat Res1998355 Suppl301313
- ColaoADi SommaCPivonelloRBone loss is correlated to the severity of growth hormone deficiency in adult patients with hypopituitarismJ Clin Endocrinol Metab19998461919192410372687
- FioreCEPennisiPCutuliVMPratoAMessinaRClementiGL-arginine prevents bone loss and bone collagen breakdown in cyclosporin A-treated ratsEur J Pharmacol2000408332332611090650
- ClementiGFioreCEManganoNGRole of soy diet and L-arginine in cyclosporin-A-induced osteopenia in ratsPharmacol Toxicol2001881161911169156
- CarlisleEMSilicon: an essential element for the chickScience197217840616196215086395
- SchwarzKMilneDBGrowth-promoting effects of silicon in ratsNature1972239537133333412635226
- CarlisleEMIn vivo requirement for silicon in articular cartilage and connective tissue formation in the chickJ Nutr197610644784841255267
- CarlisleEMSilicon: a requirement in bone formation independent of vitamin D1Calcif Tissue Int198133127346257332
- ProctorSDKellySERussellJCA novel complex of arginine-silicate improves micro- and macrovascular function and inhibits glomerular sclerosis in insulin-resistant JCR:LA-cp ratsDiabetologia20054891925193215991019
- ProctorSDKellySEVineDFRussellJCMetabolic effects of a novel silicate inositol complex of the nitric oxide precursor arginine in the obese insulin-resistant JCR:LA-cp ratMetabolism200756101318132517884439
- SahinKOnderciMSahinNDietary arginine silicate inositol complex improves bone mineralization in quailPoult Sci200685348649216553280
- OnderciMSahinNSahinKDietary arginine silicate inositol complex during the late laying period of quail at different environmental temperaturesBr Poult Sci200647220921516641032
- AdamsMRForsythCJJessupWRobinsonJCelermajerDSOral L-arginine inhibits platelet aggregation but does not enhance endothelium-dependent dilation in healthy young menJ Am Coll Cardiol1995264105410617560599
- LermanABurnettJCJrHiganoSTMcKinleyLJHolmesDRJrLong-term L-arginine supplementation improves small-vessel coronary endothelial function in humansCirculation19989721212321289626172
- LevineJControlled trials of inositol in psychiatryEur Neuropsychopharmacol1997721471559169302
- Van DyckKRobberechtHVan CauwenberghRVan VlaslaerVDeelstraHIndication of silicon essentiality in humans: serum concentrations in Belgian children and adults, including pregnant womenBiol Trace Elem Res2000771253211097468
- TokerHOzdemirHOzerHErenKA comparative evaluation of the systemic and local alendronate treatment in synthetic bone graft: a histologic and histomorphometric study in a rat calvarial defect modelOral Surg Oral Med Oral Pathol Oral Radiol20121145 Suppl146152
- TokerHOzdemirHOzerHErenKAlendronate enhances osseous healing in a rat calvarial defect modelArch Oral Biol201257111545155022795567
- CarlisleEMSilicon: a possible factor in bone calcificationScience197016739162792805410261
- EisingerJClairetDEffects of silicon, fluoride, etidronate and magnesium on bone mineral density: a retrospective studyMagnes Res1993632472498292498
- WimalawansaSJChapaMTYallampalliCZhangRSimmonsDJPrevention of corticosteroid-induced bone loss with nitric oxide donor nitroglycerin in male ratsBone19972132752809276093
- TorricelliPFiniMGiavaresiGL-arginine and L-lysine stimulation on cultured human osteoblastsBiomed Pharmacother2002561049249712504270
- SeabornCDNielsenFHEffects of germanium and silicon on bone mineralizationBiol Trace Elem Res19944221511647981005
- SchützeNOurslerMJNolanJRiggsBLSpelsbergTCZeolite A inhibits osteoclast-mediated bone resorption in vitroJ Cell Biochem199558139467642721
- SchröderHCWangXHWiensMSilicate modulates the cross-talk between osteoblasts (SaOS-2) and osteoclasts (RAW 264.7 cells): inhibition of osteoclast growth and differentiationJ Cell Biochem2012113103197320622615001
- WiensMWangXSchröderHCThe role of biosilica in the osteoprotegerin/RANKL ratio in human osteoblast-like cellsBiomaterials201031307716772520673584