
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Nifedipine gastrointestinal therapeutic system (GITS) is used to treat angina and hypertension. The authors aimed to study the early intervention impact on arterial stiffness and pulse wave velocity (PWV) independent of its blood-pressure-(BP) lowering effect in mild hypertensive patients.
Methods
This single-center, single-arm, open-label, prospective, Phase IV study recruited patients with mild hypertension and increased PWV from December 2013 to December 2014 (N=138; age, 18–75 years; systolic blood pressure, 140–160 mmHg; diastolic BP, 90–100 mmHg; increased brachial–ankle pulse wave velocity [baPWV, ≥12 m/s]). Nifedipine GITS (30 mg/d) was administered for 24 weeks to achieve target BP of <140/90 mmHg. The dose was uptitrated at 60 mg/d in case of unsatisfactory BP reduction after 4 weeks. Primary study end point was the change in baPWV after nifedipine GITS treatment. Hemodynamic parameters (office BP, 24-hour ambulatory BP monitoring, and heart rate and adverse events) were evaluated at baseline and followed-up at 2, 4, 8, 12, 18, and 24 weeks.
Results
Majority of patients (n=117; 84.8%) completed the study. baPWV decreased significantly at 4 weeks compared with baseline (1,598.87±239.82 vs 1,500.89±241.15 cm/s, P<0.001), was stable at 12 weeks (1,482.24±215.14 cm/s, P<0.001), and remained steady through 24 weeks (1,472.58±205.01 cm/s, P<0.001). Office BP reduced from baseline to week 4 (154/95 vs 136/85 mmHg) and remained steady until 24 weeks. Nifedipine GITS significantly decreased 24-hour ambulatory BP monitoring (P<0.001) after 24 weeks from baseline. Mean arterial pressure and pulse pressure were lowered significantly after 4, 12, and 24 weeks of treatment (P<0.001). These changes in baPWV were significantly correlated with changes in systolic blood pressure, diastolic BP, and mean arterial pressure (P<0.05), but not with changes in pulse pressure (P>0.05). There were no other drug-related serious adverse events.
Conclusion
Nifedipine GITS was considerably effective in reducing baPWV and BP, indicating improvement in arterial stiffness as early as 4 weeks.
Introduction
Hypertension is a frequently occurring chronic lifestyle disease that is considered as an important public health concern in People’s Republic of China. The 1991–2011 China Health and Nutrition Survey demonstrated a significant increase in the prevalence of hypertension (from 15.6% to 20.9%, P<0.001) and a substantial increase in the use of antihypertensive medications (from 2.55% to 9.01%).Citation1,Citation2 Treatment of hypertension primarily aims at reducing the overall risk of cardiovascular (CV) complications and mortality.Citation2 Successful attainment of adequate blood pressure (BP) control by appropriate treatment regimen is therefore of great concern to physicians and patients.
Aortic stiffness and arterial pulse wave velocity (PWV) are the key determinants of BP. Arterial stiffness is considered as an important prognostic index and a potential therapeutic target of hypertension that increases with age. It is an independent predictor of CV-related mortality and morbidity in patients with hypertension, diabetes mellitus, atherosclerosis, and end-stage renal disease, requiring early diagnosis.Citation3,Citation4 Increase in arterial stiffness increases the heart rate (HR) and pulsatile BP, thereby increasing cardiac workload by left ventricular afterload and altered coronary perfusion.Citation3 The assessment of brachial–ankle pulse wave velocity (baPWV) is regarded to be a classic index of arterial stiffness in large clinical trials and is considered to be a useful screening method for evaluating the atherosclerotic risk. Age and BP are reported to be robust independent predictors of the PWV.Citation5 Antihypertensive therapy should therefore be able to achieve BP reduction without any undesirable influence on the arterial stiffness.Citation6
Several clinical trials have proved the efficacy of the dihydropyridine calcium-channel blocker (CCB) “nifedipine gastrointestinal therapeutic system (GITS)” in the treatment of hypertension.Citation7–Citation10 Chronic management of hypertension with nifedipine may interfere with remodeling of large arteries and decrease arterial stiffness.Citation11 The vascular protective effects of nifedipine therapy might be related to BP reduction and appear shortly after initiation of treatment.Citation12 Therefore, vascular protection by nifedipine is not restricted to a prolonged BP modulation. It remains mostly unclear whether arterial stiffness is affected by CCBs. These findings could be relevant for an intervention in augmented vascular stiffness and related CV risk.
Till date, limited data from small-scale clinical studies are present on the effectiveness of GITS on arterial stiffness in Chinese patients with hypertension. This first Phase IV study was conducted to evaluate the effects of nifedipine GITS intervention on arterial stiffness in Chinese patients with mild hypertension and increased PWV to explore whether the improvement of structural vascular lesion with nifedipine is beyond its BP-lowering effects.
Materials
Study design
This 24-week, single-center, single-arm, open-label, prospective, cohort, Phase IV study evaluated the efficacy of nifedipine GITS (30 mg/d) on arterial stiffness and structural vascular lesions in Chinese patients with mild hypertension and increased PWV recruited between December 2013 and December 2014 (Chinese Clinical Trial Registry: ChiCTR-ONC-13004063) from the Second Hospital of Hebei Medical University, People’s Republic of China.
Patients attended an initial visit and up to six follow-up clinical visits during the 24-week observation period. The timings of the visits were specified at 2, 4, 8, 12, 18, and 24 weeks by the treating physician. Nifedipine GITS was administered at a dose of 30 mg/d, with a treatment target clinical systolic blood pressure (SBP) and diastolic blood pressure (DBP) of <140 and <90 mmHg, respectively. A permitted dose uptitration of nifedipine GITS up to 60 mg/d was allowed in case of unsatisfactory BP reduction after 4 weeks. Patients with BP >140/90 mmHg after 8 weeks of nifedipine GITS treatment were given routine clinical treatment.
The study was conducted using approved country-specific prescribing information of nifedipine GITS. It was performed in accordance with the guidelines of the European Medicines Agency and the US Food and Drug Administration, Declaration of Helsinki (1996), and the ICH Harmonized Tripartite Guideline for Good Clinical Practice and was approved by the ethics committee of the Second Hospital of Hebei Medical University, People’s Republic of China. All the patients signed the informed consent form before enrollment and were screened for inclusion in the study.
Study patients
Patients aged 18–75 years with 24-hour ambulatory BP monitoring (ABPM)-confirmed mean arterial pressure (MAP) of ≥135/85 mmHg; mild hypertension (≥140 mmHg, <160 mmHg; DBP ≥90 mmHg, <100 mmHg); body mass index <33 kg/m2; and increased baPWV (≥15 m/s) were enrolled in the study. On the contrary, pregnant or lactating women; patients who had participated in a drug clinical trial within the past 3 months, who had moderate-to-severe hypertension, or were taking any antihypertensive drug(s); and patients who had secondary hypertension, clinically significant cardio-cerebrovascular diseases, Type 1 or 2 diabetes, lower limb/peripheral arterial disease with decreased baPWV or any other GI disorder that could compromise absorption of nifedipine GITS or passage of the tablets were excluded from the analysis. Patients with creatinine level >2 mg/dL (local upper limit of normal) and alanine transaminase or aspartate transaminase level >3 mg/dL (local upper limit of normal) and those who were undergoing concomitant treatment containing a cytochrome P450-3A4 inhibitor or inducer or had valvular disease or cardiogenic disease, intracranial hemorrhage, or subarachnoid hemorrhage in the past 12 months were also excluded.
Hemodynamic and baPWV measurements
The primary aim of this study was to assess the change in baPWV from baseline to 24 weeks after nifedipine GITS treatment. Hemodynamic parameters such as office BP, HR, and baPWV were evaluated at baseline and followed-up at 2, 4, 8, 12, 18, and 24 weeks, whereas ABPM was evaluated at baseline and at the 24th week of study.
Office BP measurement
At the initial visit, office BP was measured in a quiet room with a mercury sphygmomanometer. Measurements were obtained after the patient had rested in a sitting position for at least 5 minutes. Patients with inadequate control over 5 mmHg (>145 mmHg SBP and >95 mmHg DBP) at baseline were selected as the criteria for ABPM measurement, which was performed both at baseline and at the 24th week. A 24-hour ABPM was done initially using a portable, noninvasive oscillometric device (Oscar2™, Sun Tech, Morrisville, NC, USA) with a cuff fit to the patient’s arm. The devices were programmed to measure BP every 20 minutes for 24 hours and reperformed during the 24th week of follow-up to monitor adequate BP control.
baPWV measurement
PWV was measured using the Omron-BP-203PREII full-automatic arteriosclerosis detector (Japan Colin Medical Apparatus Co., Komaki, Japan). Before the examination, various parameters of the examinee (eg, age, sex, height, and body weight) were input into the apparatus; the patients were asked to rest for 5 minutes in a supine position without a pillow and with both palms upward at the side of body; the BP measuring cuffs were then wrapped onto both upper arms and then connected to the ankle. ECG electrodes were placed on the internal side of left and right wrist, and the phonocardiogram sensor was placed at the left margin of breastbone between the fourth ribs, connected to the arterial PWV detector. The baPWV was automatically calculated according to the parameters of patient, monitored continuously twice, and their mean was analyzed. During the whole examination, the patient was advised to be in a calm state. baPWV is calculated using the following formula:
Conduction distance (L) = (D1 − D2), where D1 is the distance from the heart to the ankle and D2 is the distance from the heart to the right upper arm. These distances were calculated on the basis of the patient’s height.
Pulse conduction time is the time between the onset of the rise in the pulse volume record of the right upper arm and the onset of the rise in the pulse volume record of the left ankle.
Safety measurements
Patients demographic and blood biochemistry data were collected at baseline. Safety measures included whole blood laboratory examination (erythrocyte, hemoglobin, hematocrit, and leukocyte), blood biochemical examination (liver/kidney functional examination (eg, creatinine and urea nitrogen, electrolyte, blood fat, and uric acid), and urine laboratory examinations (pH, specific gravity, erythrocyte, glucose, and protein). Patients who were not followed up because of adverse drug reactions, worsening of symptoms, refusal to continue the study, or protocol deviations were considered as withdrawals. Patients who stopped visiting the hospital and whose condition could not be confirmed despite follow-up by letters or telephone calls were considered as being lost to follow-up.
Statistical analysis
For sample size calculation, given the scarcity of data on PWV change from 0 to 4 weeks for nifedipine, it was estimated that PWV could drop by 0.60±2.0 m/s in hypertension patients after the administration of nifedipine controlled-release tablets for 4 weeks, based on calculation from retrospective data of a different CCB.Citation13 Choosing a power of 80% and a two-sided α-level of 0.05, at least 96 patients in total were required to reach statistical significance on the basis of the preceding assumptions.
Statistical analysis was performed using SPSS statistical software (version 17.0, SPSS, Inc, Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation, and count data were expressed as percentage under normal data distribution. Repeated measures one-way analysis of variance was applied for comparing parameters such as baPWV, SBP, DBP, and HR at baseline and 4, 12, and 24 weeks. Multiple linear regression analysis was performed to determine the correlation between the following: 1) baseline characteristics and baPWV reduction and 2) change in baPWV and change of BP. A P-value of <0.05 was considered to be statistically significant.
Results
Baseline characteristics
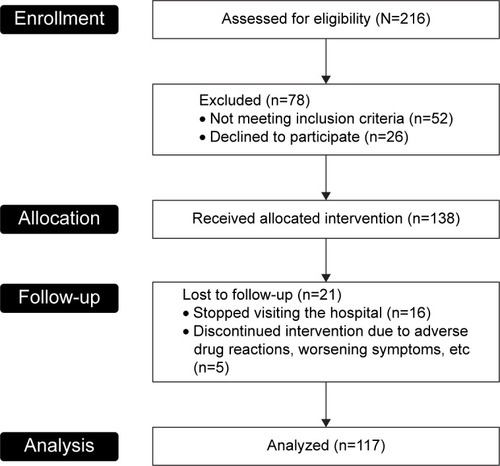
A total of 138 eligible patients were enrolled in the study. Most of the patients (n=117; 85.4%) completed the study, and few patients were removed from the study (n=21; 5 withdrew from the study and 16 were lost to follow-up; ). Baseline characteristics of 117 patients are listed in . The patient population had a mean age of 48.43±11.92 years, body mass index of 26.00±2.90 kg/m2, and consisted of 71 (60.6%) men. Mean cholesterol, low-density lipoprotein, and triglyceride levels at baseline were 4.70±0.89, 2.54±0.85, and 1.88±1.00 mmol/L, respectively. Multiple linear regression analysis showed that none of the baseline characteristics were related to baPWV reduction (P>0.05). A permitted dose uptitration of nifedipine GITS to 60 mg/d as given to 20 (14.5%) patients in whom the target BP reduction was unsatisfactory even after 4 weeks of treatment ().
Table 1 Baseline characteristics
Figure 1 Study flowchart.
Efficacy outcomes
Reduction in baPWV post-nifedipine GITS treatment
Nifedipine GITS treatment led to a significant reduction in baPWV at 4 weeks from baseline (1,598.87±239.82 cm/s vs 1,500.89±241.15 cm/s; P<0.001; ). Compared with baseline values, the decrease in baPWV was consistent and significant both after 12 and 24 weeks of treatment (1,482.24±215.14 cm/s and 1,472.58±205.01 cm/s vs 1,598.87±239.82 cm/s; P<0.001 for both). However, no statistical differences were observed between baPWV at 1) 4 and 12 weeks of treatment and 2) 12 and 24 weeks of treatment (P>0.05).
Table 2 Changes in hemodynamic parameters and baPWV during the follow-up periodTable Footnotea
BP-dependent baPWV changes
Multiple linear regression analysis () revealed correlation between changes in baPWV and changes in SBP (r=0.325; P=0.008), DBP (r=0.348; P=0.005), and MAP (r=0.39; P=0.002). This explains that acute baPWV changes may be dependent on BP. However, the change in baPWV did not correlate with change in pulse pressure (PP; r=0.219; P=0.074).
Figure 2 Correlation of baPWV with BP changes.
Attenuation of hemodynamic indices after 24-week nifedipine GITS treatment
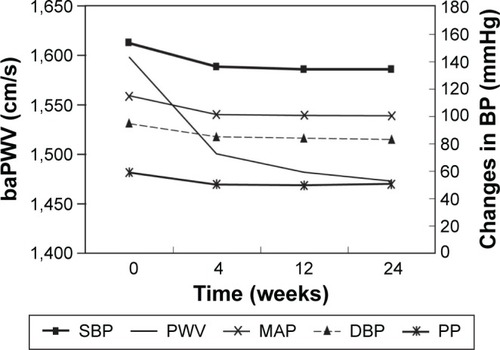
Treatment with nifedipine GITS for 24 weeks demonstrated a significant lowering of the 24-hour ABPM (A-SBP, 144.59±22.62 vs 134.12±22.29 mmHg; A-DBP, 90.25±15.89 vs 82.99±14.75 mmHg; P<0.001; ). After 24 weeks of nifedipine treatment, a significant decrease in SBP, DBP, MAP, and PP was observed compared with the baseline values (P<0.001; ). However, nonsignificant changes were observed in BP, MAP, and PP between values after 4, 12, and 24 weeks of treatment (P>0.05). There were no significant changes in HR after 4, 12, and 24 weeks treatment compared with the baseline values (P>0.05). As can be seen from , the baPWV gradually decreased with increased duration independent of the SBP- and DBP-lowering effect of nifedipine GITS.
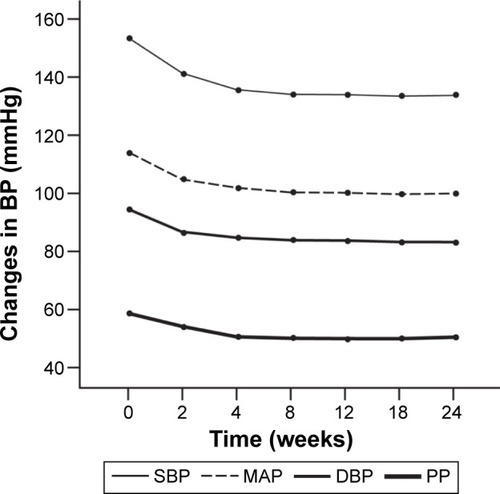
Figure 3 Changes in hemodynamic parameters.
Safety outcomes
Headache (n=3; 2.2%) and lack of drug efficacy (n=2; 1.4%) were the main reasons for withdrawal from the study. Manageable headache and peripheral edema were reported in five patients each (3.6%). There were no other drug-related serious adverse events.
Discussion
The rising prevalence of hypertension and arterial stiffness, and associated risk factors, provides a major thrust to better understand treatment modalities. Arterial stiffness progressively increases with age and is a risk factor for CV diseases, and it adversely affects the prognosis of a patient.Citation14,Citation15 The correlation between elevation in BP and arterial stiffness is yet to be completely elucidated. Aortic stiffness and pulse wave are the key determinants of elevated systolic pressure and are closely associated with adverse CV outcomes.Citation16 It has been observed that uncontrolled BP and the combination of metabolic factors might cause an increase in arterial stiffness.Citation17 However, literature shows that arterial stiffness may even precede hypertension, challenging the classic paradigm that hypertension leads to altered vascular structure and function that causes increased arterial stiffness.Citation18 Although both have a close association with increasing age, in certain cases even hypertension, diabetes mellitus, hypercholesterolemia, and oxidative stress may amplify or act synergistically in causing vascular changes leading to arterial stiffening.Citation19,Citation20 PWV is one of the most important, commonly measured, well understood, and the best surrogate parameter for measuring arterial stiffness.Citation21,Citation22 Although carotid femoral PWV is the gold standard for measuring arterial stiffness, baPWV is considerably faster and is more convenient. Moreover, the PWV of peripheral arteries is greater than central arteries; hence, it is a suitable index for monitoring arterial wall stiffness.Citation13 Studies suggest that despite similar brachial arterial BP-lowering effects, the impact of various antihypertensive drug classes on central aortic BP and arterial stiffness differs. ACE inhibitors,Citation23,Citation24 CCBs,Citation25,Citation26 and mineralocorticoid receptor antagonists Citation27,Citation28 are beneficial in reducing arterial stiffness and central BP, whereas some β-blockers may have the opposite effects while lowering peripheral BP.Citation29 It is of utmost concern for the physicians that antihypertensive agents should not have an undesirable influence on arterial stiffness.
Nifedipine GITS (controlled-release form) is known to be present in the GI tract for a period of 24–36 hours and provide steady plasma concentrations.Citation30 Intervention as a Goal in Hypertension Treatment, a large randomized controlled trial, showed the efficacy and safety of nifedipine GITS in elderly patients with hypertension.Citation7 Nonetheless, a post hoc analysis of the Intervention as a Goal in Hypertension Treatment data using the Framingham risk equation demonstrated that nifedipine GITS improved CV outcomes and reduced the risk of CV events by about 50%.Citation31
Furthermore, genetic variations may influence the efficacy and safety of drugs. The genetic variations in cytochrome P3A4 are known to be associated with defective metabolism of nifedipine.Citation32 However, studies report that the incidence of CYP3A4 enzyme mutations is very rare or minimal in Chinese subjects compared to the western population.Citation33 In addition, a study on the impact of genetic variations in CYP enzymes on efficacy and safety of amlodipine in Chinese hypertensive patients revealed that the CYP3A4 activity had no clear influence on the curative effects of amlodipine.Citation34 As nifedipine belongs to the amlodipine class of antihypertensives, it is plausible to infer that such genetic variants would have no or minimal influence on the curative effects of this study intervention. However, further studies on the impact of such genetic variants on nifedipine GITS treatment in Chinese hypertensive patients are warranted to further understand the outcomes.
This first open-label prospective study conducted in People’s Republic of China will provide guidance to physicians for better understanding of effect of long-term nifedipine GITS treatment on arterial stiffness in mild hypertensives. However, further studies on the curative effects of nifedipine GITS on arterial stiffness in elderly hypertensive patients with diabetes and chronic renal diseases are warranted, as these groups are at high risk of CV events as they are usually present with arterial stiffness.
In this study, SBP, DBP, MAP, and PP values significantly (P<0.001) reduced after 4, 12, and 24 weeks of treatment with nifedipine GITS compared with baseline values. Compared with baseline values, 24-hours ABPM was also significantly decreased after 24 weeks of treatment with nifedipine GITS (P<0.001). These observations were consistent with the pharmacological profile of nifedipine GITS and demonstrated maximal BP-lowering potential of nifedipine GITS at 4 weeks.
Although there is abundant evidence that long-acting CCBs can improve the prognosis of patients with CV disease,Citation35,Citation36 their mechanism of action remains unclear in patients with hypertension. This study showed a significant decrease in baPWV after 4 weeks of nifedipine GITS treatment, and this effect was maintained up to 24 weeks of treatment. In addition, there were no significant changes in HR over the entire 24-week treatment schedule. Multiple linear regression analysis performed in the study revealed that changes in baPWV were correlated with changes in SBP, DBP, and MAP, but not with changes in PP. However, the study results also revealed that the baPWV decreasing capacity and arterial stiffness improvement was little beyond the BP-lowering effect of nifedipine. Hence, larger studies with longer treatment duration are warranted to derive the pressure-independent baPWV-lowering factors of nifedipine GITS.
A randomized study by Munakata et alCitation37 demonstrated reduction in PWV with 3 months of treatment with nifedipine coat-core versus baseline values (−69±40 cm/s vs 1,622±64 cm/s nonsignificant) and reduction in BP (nifedipine, −18.4±4.2/−11.9±2.7 mmHg), demonstrating a positive effect of nifedipine on arterial stiffness. Significant reduction in baPWV was also observed in another study with nifedipine coat-core (P=0.0472) compared with amlodipine. HR recovery was significantly better with nifedipine treatment (P=0.0280), indicating that nifedipine reduced functional arterial stiffness and improved HR recovery by varying autonomic activity balance in patients with hypertension.Citation11
The aforementioned observations indicate that the results of this study are in accordance with the previously published literature and suggest that nifedipine GITS can significantly decrease baPWV and BP in patients with mild hypertension and increased PWV from 4 weeks after initiating the therapy.
This study has some inherent limitations that do not allow for definite conclusions to be drawn. The bias introduced by the open-label, nonrandomized study design cannot be overcome by any statistical method. BP reading could be highly variable because of factors such as posture, room temperature, and pain/discomfort or stress. BP can also vary if patients move the cuff due to uneasiness caused by 24-hour ABPM. Many factors such as emotional state and patient compliance influence the measurement of baPWV, resulting in erroneous values. The patients were followed-up for only 24 weeks, and so the long-term effects of nifedipine GITS on arterial stiffness remain largely unknown. Furthermore, the study had nongeneralizable findings as it is restricted to Chinese population alone and was conducted at a single center. In addition, the study did not infer the curative benefits of the intervention on secondary or moderate-to-severe hypertensive patients due to the exclusion criteria and study design, which was limited only to mild hypertensives. In addition, elderly patients with Type 1 and 2 diabetes and CKD were excluded. Given these limitations, the results may not indicate an improvement of arterial stiffness with long-term treatment with nifedipine GITS. Therefore, the results of the present analysis should be interpreted with caution. However, the fact that this study can provide relevant information in real-life clinical settings that are likely to reflect and inform daily practice cannot be neglected. Further studies are warranted to explore whether this improvement of arterial stiffness following long-term treatment with nifedipine GITS could bring some beneficial effects on CV events in CKD and Type 1 and 2 diabetes patients as well.
Conclusion
Given the salutary benefit of nifedipine GITS in decreasing baPWV and BP, as well as improvement in arterial stiffness as early as 4 weeks, it may be considered a valuable treatment option in mild hypertensive patients with increased PWV. However, further large multicenter and long-duration studies are warranted to elucidate the findings.
Authors contributions
All the authors planned and contributed to the interpretation of the data, revisions, and inputs at all stages of the study. All the authors have approved the final version of the manuscript.
Acknowledgments
The authors acknowledge Dr Guanming Zhang and Dr Qian Wang (The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China) for providing their inputs throughout the study. The authors also thank Dr Amit Bhat and Miss Navya Reddy (Indegene Private Ltd., Bangalore, India), for providing editorial support in the preparation of the manuscript, with funding from Bayer Healthcare Company Ltd. This manuscript is a unique submission and is not being considered for publication by any other source in any medium. Furthermore, the manuscript has not been published, in part or in full, in any form.
Disclosure
The study was partly funded by Bayer Healthcare Company Ltd. The authors report no other conflicts of interests in this work.
References
- QiSFZhangBWangHJPrevalence of hypertension subtypes in 2011 and the trends from 1991 to 2011 among Chinese adultsJ Epidemiol Community Health201670544445126612877
- WangJZhangLWangFLiuLWangHPrevalence, awareness, treatment, and control of hypertension in China: results from a national surveyAm J Hypertens201427111355136124698853
- BlacherJAsmarRDjaneSLondonGMSafarMEAortic pulse wave velocity as a marker of cardiovascular risk in hypertensive patientsHypertension19993351111111710334796
- CeceljaMChowienczykPRole of arterial stiffness in cardiovascular diseaseJRSM Cardiovasc Dis201214
- JanicMLunderMSabovicMArterial stiffness and cardiovascular therapyBiomed Res Int2014201462143725170513
- DuprezDAIs vascular stiffness a target for therapy?Cardiovasc Drugs Ther201024430531020628896
- BrownMJPalmerCRCastaigneAMorbidity and mortality in patients randomised to double-blind treatment with a long-acting calcium-channel blocker or diuretic in the International Nifedipine GITS study: Intervention as a Goal in Hypertension Treatment (INSIGHT)Lancet2000356922736637210972368
- Poole-WilsonPALubsenJKirwanBAEffect of long-acting nifedipine on mortality and cardiovascular morbidity in patients with stable angina requiring treatment (ACTION trial): randomised controlled trialLancet2004364943784985715351192
- HasebeNKikuchiKControlled-release nifedipine and candesartan low-dose combination therapy in patients with essential hypertension: the NICE Combi (Nifedipine and Candesartan Combination) studyJ Hypertens200523244545315662234
- SaitoIFujikawaKSarutaTCost-effectiveness analysis: controlled-release nifedipine and valsartan combination therapy in patients with essential hypertension: the adalat CR and valsartan cost-effectiveness combination (ADVANCE-Combi) studyHypertens Res20083171399140518957811
- FukudaMMasudaTOguraMNInfluence of nifedipine coat-core and amlodipine on systemic arterial stiffness modulated by sympathetic and parasympathetic activity in hypertensive patientsHypertens Res200932539239819373239
- VajaVOchodnickyPKrenekPKlimasJBajuszovaZKyselovicJRapid large artery remodeling following the administration and withdrawal of calcium channel blockers in spontaneously hypertensive ratsEur J Pharmacol20096191–3859119683522
- KitaTSuzukiYEtoTKitamuraKLong-term anti-hypertensive therapy with benidipine improves arterial stiffness over blood pressure loweringHypertens Res2005281295996416671334
- DudenbostelTGlasserSPEffects of antihypertensive drugs on arterial stiffnessCardiol Rev201220525926322573107
- GlasserSPDudenbostelTThe global burden of cardiovascular disease: the role of endothelial function and arterial elasticity in cardiovascular disease as novel and emerging biomarkersCurr Cardiovasc Risk Rep20115218719524000308
- PayneRAWilkinsonIBWebbDJArterial stiffness and hypertension: emerging conceptsHypertension201055191419948990
- NajjarSSScuteriAShettyVPulse wave velocity is an independent predictor of the longitudinal increase in systolic blood pressure and of incident hypertension in the Baltimore longitudinal study of agingJ Am Coll Cardiol200851141377138318387440
- CohnJNFinkelsteinSMcVeighGNoninvasive pulse wave analysis for the early detection of vascular diseaseHypertension19952635035087649589
- ZiemanSJMelenovskyVKassDAMechanisms, pathophysiology, and therapy of arterial stiffnessArterioscler Thromb Vasc Biol200525593294315731494
- TomiyamaHKushiroTOkazakiRYoshidaHDobaNYamashinaAInfluences of increased oxidative stress on endothelial function, platelets function, and fibrinolysis in hypertension associated with glucose intoleranceHypertens Res200326429530012733697
- SethiSRiveraOOliverosRChiltonRAortic stiffness: pathophysiology, clinical implications, and approach to treatmentIntegr Blood Press Control20147293424910511
- WentlandALGristTMWiebenOReview of MRI-based measurements of pulse wave velocity: a biomarker of arterial stiffnessCardiovasc Diagn Ther20144219320624834415
- ProtogerouADStergiouGSVlachopoulosCBlacherJAchimastosAThe effect of antihypertensive drugs on central blood pressure beyond peripheral blood pressure. Part II: evidence for specific class-effects of antihypertensive drugs on pressure amplificationCurr Pharm Des200915327228919149618
- ShahinYKhanJAChetterIAngiotensin converting enzyme inhibitors effect on arterial stiffness and wave reflections: a meta-analysis and meta-regression of randomised controlled trialsAtherosclerosis20122211183322209214
- AgnolettiDZhangYBorghiCBlacherJSafarMEEffects of anti-hypertensive drugs on central blood pressure in humans: a preliminary observationAm J Hypertens20132681045105223736112
- HayozDZappeDHMeyerMAChanges in aortic pulse wave velocity in hypertensive postmenopausal women: comparison between a calcium channel blocker vs angiotensin receptor blocker regimenJ Clin Hypertens (Greenwich)2012141177377823126349
- BoesbyLElung-JensenTStrandgaardSKamperALEplerenone attenuates pulse wave reflection in chronic kidney disease stage 3–4 – a randomized controlled studyPLoS One201385e6454923704994
- VizzardiEPinaPDCarettaGThe effect of aldosterone-antagonist therapy on aortic elastic properties in patients with nonischemic dilated cardiomyopathyJ Cardiovasc Med (Hagerstown)201516959760224978872
- PoloniaJBarbosaLSilvaJABertoquiniSDifferent patterns of peripheral versus central blood pressure in hypertensive patients treated with beta-blockers either with or without vasodilator properties or with angiotensin receptor blockersBlood Press Monit201015523523920577082
- ElliottHLElawadMWilkinsonRSinghSPPersistence of anti-hypertensive efficacy after missed doses: comparison of amlodipine and nifedipine gastrointestinal therapeutic systemJ Hypertens200220233333811821720
- HeagertyAMNifedipine gastrointestinal therapeutic system – hypertension management to improve cardiovascular outcomesInt J Clin Pract20055991112111916115193
- LeeSJBellDACoulterSJGhanayemBGoldsteinJARecombinant CYP3A4*17 is defective in metabolizing the hypertensive drug nifedipine, and the CYP3A4*17 allele may occur on the same chromosome as CYP3A5*3, representing a new putative defective CYP3A haplotypeJ Pharmacol Exp Ther2005313130230915634941
- HsiehKPLinYYChengCLNovel mutations of CYP3A4 in ChineseDrug Metab Dispos200129326827311181494
- GuoCPeiQITanHHuangZYuanHYangGEffects of genetic factors on the pharmacokinetics and pharmacodynamics of amlodipine in primary hypertensive patientsBiomed Rep20153219520026075072
- LubsenJWagenerGKirwanBAdeBSPoole-WilsonPAEffect of long-acting nifedipine on mortality and cardiovascular morbidity in patients with symptomatic stable angina and hypertension: the ACTION trialJ Hypertens200523364164815716708
- NissenSETuzcuEMLibbyPEffect of antihypertensive agents on cardiovascular events in patients with coronary disease and normal blood pressure: the CAMELOT study: a randomized controlled trialJAMA2004292182217222515536108
- MunakataMNagasakiANunokawaTEffects of valsartan and nifedipine coat-core on systemic arterial stiffness in hypertensive patientsAm J Hypertens20041711 Pt 11050105515533733