
Abstract
This review article discusses the potential of nanomaterials in targeted therapy and immunomodulation for stroke-induced immunosuppression. Although nanomaterials have been extensively studied in various biomedical applications, their specific use in studying and addressing immunosuppression after stroke remains limited. Stroke-induced neuroinflammation is characterized by T-cell-mediated immunodepression, which leads to increased morbidity and mortality. Key observations related to immunodepression after stroke, including lymphopenia, T-cell dysfunction, regulatory T-cell imbalance, and cytokine dysregulation, are discussed. Nanomaterials, such as liposomes, micelles, polymeric nanoparticles, and dendrimers, offer advantages in the precise delivery of drugs to T cells, enabling enhanced targeting and controlled release of immunomodulatory agents. These nanomaterials have the potential to modulate T-cell function, promote neuroregeneration, and restore immune responses, providing new avenues for stroke treatment. However, challenges related to biocompatibility, stability, scalability, and clinical translation need to be addressed. Future research efforts should focus on comprehensive studies to validate the efficacy and safety of nanomaterial-based interventions targeting T cells in stroke-induced immunosuppression. Collaborative interdisciplinary approaches are necessary to advance the field and translate these innovative strategies into clinical practice, ultimately improving stroke outcomes and patient care.
Introduction
Stroke is a devastating neurological condition characterized by the interruption of blood flow to the brain, leading to brain tissue damage and functional impairments.Citation1–3 In addition to the acute damage caused by the initial ischemic event, stroke triggers a complex cascade of secondary processes, including neuroinflammation, immune cell activation, and immunodepression.Citation4–10 Among the immune cells involved in the poststroke immune response, T cells have emerged as key players in modulating the inflammatory environment and influencing stroke outcomes.Citation11–13
T-cell-mediated immunodepression refers to the functional impairment and reduced immune response observed in T cells following stroke. This immunodepressive state can lead to increased susceptibility to infections and impaired recovery.Citation14 Understanding the role of T cells in stroke pathophysiology and their impact on stroke outcomes is crucial for developing effective therapeutic strategies.
In recent years, nanomaterials have gained considerable attention in the field of biomedicine due to their unique properties and versatile applications. Nanomaterials offer opportunities for targeted therapy and immunomodulation by enabling precise interactions with biological systems at the nanoscale. The small size and tunable characteristics of these vesicles make them ideal for targeting specific cells, including T cells, and delivering therapeutic agents directly to the desired sites of action.Citation15–18 While nanomaterials have been extensively studied for the treatment of various diseases, few studies have applied them to address immunodepression after stroke.Citation19
The use of nanomaterials in stroke research provides exciting avenues for modulating T-cell-mediated immunodepression and improving stroke outcomes. Nanomaterials can be functionalized with ligands or antibodies that selectively bind to T cells, allowing for targeted delivery of immunomodulatory agents.Citation20 Furthermore, the physicochemical properties of nanomaterials can be engineered to enhance drug stability, prolong circulation time, and provide controlled release, ensuring optimal delivery and efficacy.Citation21
Additionally, nanomaterials possess inherent immunomodulatory properties that can be harnessed to counteract immunodepression. Some nanomaterials can act as adjuvants, stimulating immune responses and enhancing T-cell activation.Citation22–24 Others can scavenge reactive oxygen species, reducing oxidative stress and mitigating T-cell dysfunction.Citation25 By leveraging these unique properties, nanomaterial-based approaches hold great promise for promoting a favorable immune environment and restoring T-cell function in stroke patients.
In this review article, we aim to explore the untapped potential of nanomaterials for targeted therapy and immunomodulation, specifically in the context of stroke-induced immunodepression (). Our goal was to provide a comprehensive overview of the role of T-cell-mediated immunodepression in stroke pathophysiology and its significant implications for stroke outcomes. We will delve into the unique properties of nanomaterials and their diverse applications in targeted therapy and immunomodulation. Specifically, we highlight recent advancements in nanomaterial-based delivery systems and immunomodulatory nanotherapies, focusing on their potential to modulate T-cell function and alleviate immunodepression in stroke patients. By shedding light on the unexplored potential of nanomaterials in this specific context, we hope to inspire further research and development in the field and ultimately contribute to the advancement of stroke treatment strategies.
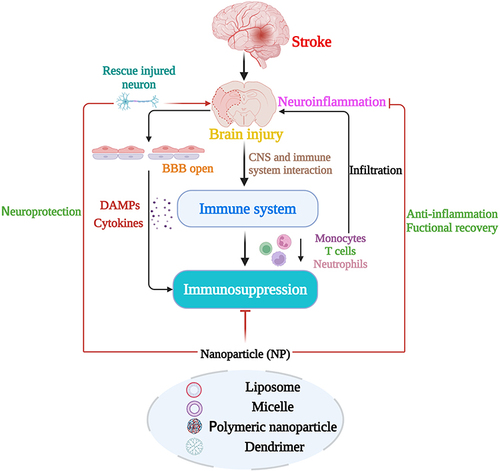
Figure 1 Illustration of the relationships between stroke, brain injury, and immunodepression and the role of nanotechnologies. The diagram illustrates the sequence of events following a stroke. Initially, stroke causes brain injury, leading to the opening of the blood‒brain barrier (BBB) and the release of damage-associated molecular patterns (DAMPs). This influences the peripheral immune system, particularly affecting T-cell function and leading to a state of immunodepression. Concurrently, the brain interacts with the immune system, further intensifying this immunodepression. Following these initial changes, peripheral immune cells, including neutrophils, monocytes, and T cells, are recruited to the ischemic brain, where they exacerbate neuroinflammation and reinforce the immunosuppressive state. Nanotechnologies are potential tools for intervening in this cascade and have potential applications in acute neuroprotection, anti-inflammatory therapy, and T-cell targeting strategies aimed at attenuating poststroke immunodepression.
By elucidating the synergistic interplay between T-cell-mediated immunodepression and nanomaterial-based interventions, we hope to pave the way for the development of innovative and effective strategies to improve stroke outcomes. This comprehensive exploration of nanomaterial-based approaches for targeted therapy and immunomodulation in stroke patients holds great promise for advancing our understanding of stroke pathophysiology and facilitating the translation of novel therapies from the bench to the bedside.
Stroke Results in Immunodepression
Stroke-Induced Immunosuppression and T-Cell Dysfunction
Immunodepression after stroke is associated with alterations in specific subsets of T cells, namely, CD4+ and CD8+ T cells.Citation26 These T-cell populations play crucial roles in orchestrating immune responses and regulating inflammation.Citation6,Citation27 Following ischemic stroke, there is a reduction in both CD4+ and CD8+ T-cell numbers, contributing to the overall lymphopenia observed in stroke-induced immunosuppression.
CD4+ T cells, also known as helper T cells, are important for coordinating immune responses and activating other immune cells.Citation28 They play a crucial role in promoting the differentiation and function of various immune cell subsets, including B cells and cytotoxic CD8+ T cells.Citation29 After stroke, a reduction in the CD4 T-cell number compromises the ability of patients to provide adequate immune support and effectively modulate the immune response.Citation11 CD8+ T cells, also known as cytotoxic T cells, are responsible for directly eliminating infected or damaged cells. They recognize and kill target cells harboring specific antigens, including those derived from pathogens or damaged tissue.Citation12 In stroke-induced immunosuppression, there is a decrease in the number of circulating CD8+ T cells, which compromises the immune system’s ability to eliminate infected cells and control immune responses at the site of injury.Citation27 Along with functional impairments, the reductions in CD4+ and CD8+ T cells after stroke contribute to an inadequate immune response against infections and to the dysregulation of poststroke inflammation.Citation30–32 This immunodepression state increases susceptibility to infections and impairs the body’s ability to control inflammatory processes effectively. Understanding the mechanisms underlying the reduction and dysfunction of CD4+ and CD8+ T cells after stroke is crucial for developing strategies to mitigate immunodepression and improve patient outcomes. However, further research is needed to uncover the specific factors contributing to these T-cell alterations and to explore potential therapeutic interventions targeting T cells to restore immune function and mitigate the adverse effects of immunodepression after stroke.
Stroke-induced immunodepression is characterized by functional changes in lymphocyte populations, particularly a shift from T helper 1 (Th1) to T helper 2 (Th2) activity.Citation33,Citation34 This shift impairs the antibacterial defense mediated by Th1 cytokines, such as interferon-γ (IFN-γ). Reestablishing IFN-γ production helps prevent stroke-associated pneumonia. Studies in both animals and humans have shown that the rapid Th1/Th2 shift,Citation35 assessed by key cytokines, is associated with stroke-associated pneumonia and correlates with stroke severity.Citation6 The shift toward a Th2 response persists for several months and is linked to a higher infection rate.Citation36 Invariant natural killer T cells also contribute to the Th1/Th2 shift by releasing IL-10. These findings highlight the importance of understanding the immune response in stroke-induced immunosuppression and its impact on infection susceptibility.Citation37
Regulatory T cells (Tregs) are a subset of CD4+ T cells known for their immunosuppressive properties.Citation38 They function to maintain immune homeostasis, prevent excessive inflammation, and suppress autoreactive and excessive immune responses. In the context of stroke, Tregs have been shown to be involved in regulating the immune response and mitigating poststroke inflammation.Citation39 The number of Tregs in the ischemic brain after stroke gradually increases over time, reaching a peak at approximately 40% of the CD4+ T cells on day 14 and persisting for 2 months.Citation40 Tregs exhibit temporal and spatial variations, with increased proliferation on the ischemic hemisphere side.Citation41 However, there are differences in the timing and distribution of Tregs in various stroke models, with some studies observing an early increase in Tregs within 24 hours after stroke.Citation42 These findings emphasize the dynamic nature of Tregs in stroke-induced immune responses. Studies have demonstrated a reduction in Treg numbers and impaired suppressive function after stroke, contributing to the dysregulated immune response and increased inflammation observed in stroke-induced immunosuppression.Citation43 This reduction in Tregs compromises their ability to suppress excessive immune activation and dampen inflammation, thereby exacerbating poststroke immune dysregulation.Citation31 Changes in the number of peripheral Tregs occur after ischemic stroke. The total number of T cells in the peripheral blood decreases, while the proportion of Tregs significantly increases. The proportion of Tregs initially decreases on day 1 after stroke, then returns to normal on day 3 and reaches approximately 10% on day 7, suggesting that Tregs are redistributed after stroke. It is believed that Tregs migrate from the periphery to the brain early after stroke and exert their effects on cerebral ischemia through the peripheral immune system.Citation44
A study led by Professor Offner investigated the impact of experimental stroke on the spleen and immune cell populations.Citation45 Their results showed that stroke leads to splenic atrophy, accompanied by an increase in the number of Tregs in the spleen and in the number of circulating macrophages in the blood. These findings suggest an immune regulatory response and immune activation following stroke. This study provides insights into the immune alterations associated with stroke, highlighting the involvement of Tregs and macrophages.Citation45 An imbalance of Tregs during stroke-induced immunodepression has implications for the overall immune response and disease progression.Citation46 Decreased Treg numbers and dysfunction contribute to a proinflammatory environment, promoting the release of inflammatory cytokines and the activation of other immune cells.Citation47 This sustained inflammation can further damage brain tissue, impair neuroregeneration, and exacerbate secondary complications.Citation48 The relationship between Tregs and immunodepression after stroke is complex and multifaceted.Citation27 While Tregs normally play a beneficial role in immune regulation, their depletion and dysfunction in stroke can contribute to an inadequate immune response, heightened inflammation, and subsequent immunodepression.Citation49 Therefore, understanding the underlying mechanisms involved in Treg alterations after stroke and exploring strategies to restore Treg numbers and suppressive function hold potential for developing therapeutic interventions, including T-cell-based nanoparticles.Citation50 Targeting Tregs to enhance their regulatory capacity or modulate their function may help mitigate immunodepression, promote immune homeostasis, and improve poststroke outcomes.Citation51 Elucidating the intricate mechanisms governing Treg dynamics after stroke and exploring innovative approaches to harness the immunomodulatory potential of Tregs are essential.
In addition, in stroke-induced immunodepression, both the adaptive and innate immune systems are affected, with more changes observed in functionality than in cellularity. The expression of monocytic HLA-DR, a well-characterized marker, has been found to be significantly lower in stroke patients with stroke-associated pneumonia (SAP) than in patients without SAP or healthy controls.Citation52,Citation53 Decreased HLA-DR expression on monocytes is observed as early as day 1 after stroke, preceding the occurrence of infections typically observed between days 2 and 5.Citation53,Citation54 Similar rapid effects are observed in lymphocytes. Additionally, other myeloid cells, such as dendritic cells, exhibit decreased HLA-DR, CD64, and CD14 expression, which may contribute to immunosuppression.Citation55 Interestingly, immunodepressive IL-10+ monocytes exhibit increased HLA-DR expression after stroke. In experimental stroke,Citation56 impaired antibacterial defense of macrophages and alveolar epithelial cells has been shown to play a crucial role in SAP.Citation57 These findings collectively demonstrate that stroke induces functional changes in monocytes and other myeloid cells, increasing susceptibility to infection. Understanding stroke-induced immunosuppression and T-cell dysfunction, especially the different functions of various T-cell subtypes as well as their functional timing, is crucial for choosing the correct nanoparticles and timing for the application of this medicine.
Relationship Between Immunodepression and Cytokine Dysregulation
After stroke, cytokines, which are signaling molecules that play a crucial role in immune responses and inflammation, are dysregulated.Citation58 This dysregulation contributes to immunosuppression by promoting a proinflammatory environment and impairing the balance between proinflammatory and anti-inflammatory signaling.Citation59 One key observation is the increase in proinflammatory cytokines, including interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α), and IFN-γ, after stroke in the ischemic brain. These cytokines are produced by various immune cells, such as macrophages, microglia, and T cells, and contribute to the activation of immune responses and the recruitment of immune cells to sites of injury. Furthermore, these proinflammatory cytokines can directly affect T-cell function by inhibiting T-cell proliferation, cytokine production, and cytotoxic activity. These cells create an inflammatory environment that is detrimental to T-cell survival and function. Additionally, excessive proinflammatory cytokine production contributes to the recruitment and activation of other immune cells, further exacerbating inflammation and tissue damage. In the context of stroke, excessive production of proinflammatory cytokines can lead to sustained inflammation and tissue damage.Citation60,Citation61 Conversely, there is a decrease in the levels of anti-inflammatory cytokines, such as interleukin-10 (IL-10), which normally play regulatory roles in dampening immune responses and promoting immune tolerance.Citation62 Marius Piepke et al reported that IL-10 improves stroke outcome by controlling the detrimental interleukin-17A response.Citation62 The reduced levels of anti-inflammatory cytokines contribute to an imbalance between proinflammatory and anti-inflammatory signals, favoring a proinflammatory environment that further perpetuates immune dysfunction. This cytokine imbalance has several implications for immunosuppression after stroke.Citation27,Citation63 First, the excessive production of proinflammatory cytokines can impair the function of immune cells, including T cells, leading to their dysfunction and reduced immune responses. It can also disrupt the balance of immune cell subsets and contribute to the polarization of immune responses toward a proinflammatory phenotype. Second, the decrease in anti-inflammatory cytokines limits the regulatory mechanisms that dampen excessive immune activation, contributing to prolonged inflammation and tissue damage.
Overall, the dysregulation of cytokines after stroke plays a significant role in immunosuppression by promoting a proinflammatory environment and impairing immune responses. Targeting cytokine signaling pathways and rebalancing the cytokine profile may be useful for modulating the immune response, reducing inflammation, and restoring immune function in stroke-induced immunosuppression. Dysregulation of cytokines after stroke profoundly impacts T-cell reduction and dysfunction.Citation30 An altered cytokine profile characterized by increased proinflammatory cytokines and decreased anti-inflammatory cytokines contributes to impaired function and a reduced number of T cells. A dysregulated cytokine profile not only directly affects T cells but also influences the overall immune environment and T-cell interactions with other immune cells.Citation64 An imbalance between proinflammatory and anti-inflammatory cytokines can disrupt regulatory networks that involve T cells and other immune cells, such as macrophages, dendritic cells, and Tregs cells.Citation46,Citation65,Citation66 These interactions are crucial for maintaining immune homeostasis and proper T-cell function. Disruption of these networks further contributes to T-cell dysfunction and impaired immune responses.
In summary, the dysregulation of cytokines after stroke has a direct impact on T-cell reduction and dysfunction. Altered proinflammatory cytokines and anti-inflammatory cytokines create an inflammatory environment that impairs T-cell function and survival. Utilizing nanoparticles to restore the balance of cytokines and modulate cytokine signaling pathways may be promising for mitigating T-cell-mediated immunodepression and promoting immune recovery after stroke.
The Pathological Mechanisms of Immunosuppression After Stroke
Stroke-induced immunodepression is a complex process that involves intricate interactions among central nervous system (CNS) injuries, immune system dysregulation, sympathetic and parasympathetic pathways, and the endocrine system ().Citation6,Citation8,Citation67,Citation68 Following ischemic stroke, the CNS is damaged and releases a cascade of proinflammatory cytokines and damage-associated molecular patterns (DAMPs).Citation69 While these signals trigger an immune response, the immune-privileged status of the CNS and the release of immunosuppressive factors result in dysregulated immune function. Microglia, the resident immune cells of the CNS, become activated in response to stroke-induced inflammation.Citation70 While their activation initially contributes to neuroinflammation, prolonged microglial activation can lead to excessive inflammation and immune cell dysfunction, including T-cell dysfunction. Furthermore, the breakdown of the blood‒brain barrier (BBB) allows immune cells, including T cells, to infiltrate the brain.Citation71 However, the CNS environment, characterized by immunosuppressive factors and limited antigen presentation, can dampen T-cell responses, resulting in immunodepression.
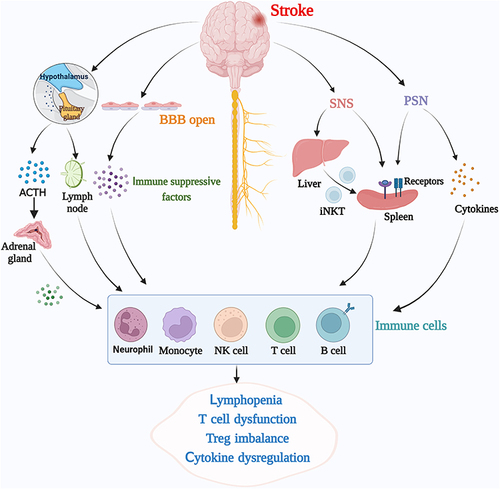
Figure 2 Diagram illustrating the pathophysiological mechanisms of stroke-induced immunosuppression. Following a stroke, several systems—including systemic inflammatory responses, the neuroendocrine system, and the autonomic nervous system—contribute to the induction of immunosuppression. Initial neuroinflammation in the ischemic brain leads to breakdown of the blood‒brain barrier (BBB) and release of inflammatory mediators into the circulation, thereby impacting circulating immune cells. The activation of the hypothalamic‒pituitary‒adrenal (HPA) axis in response to stroke results in elevated levels of glucocorticoids, which inhibit immune cell function, contributing to immunosuppression. Additionally, the sympathetic nervous system (SNS) mediates immunosuppression via the delivery of invariant natural killer T (iNKT) cells to the liver and norepinephrine (NE), subsequently affecting spleen function and resulting in immunodepression. Finally, the parasympathetic nervous system (PSNS) influences immunosuppression through the release of acetylcholine (Ach) and cytokines, further affecting T-cell functions. The diagram illustrates these complex interactions and their cumulative role in stroke-induced immunosuppression.
In addition to CNS injuries, sympathetic pathways are activated in response to stroke.Citation58,Citation72,Citation73 Increased sympathetic outflow leads to the release of stress hormones, such as adrenaline and noradrenaline, which can modulate immune responses, including T-cell function. Sympathetic activation induces T-cell apoptosis,Citation74 suppresses T-cell activation and proliferation, and alters the balance of T-cell subsets, contributing to immunodepression.Citation73 Furthermore, sympathetic pathways influence the trafficking of immune cells by altering adhesion molecule expression and chemokine gradients, affecting their recruitment and infiltration into stroke-affected regions.Citation75
The endocrine system also plays a significant role in stroke-induced immunodepression.Citation76,Citation77 Stroke triggers a stress response, resulting in the release of glucocorticoids, such as cortisol, from the adrenal glands. Glucocorticoids have potent immunosuppressive effects and can modulate T-cell function. They inhibit T-cell activation, proliferation, and cytokine production, leading to immunodepression. Glucocorticoids also influence the balance of T-cell subsets, favoring the expansion of Tregs over effector T cells and further suppressing immune responses.
In summary, immunodepression after stroke arises from the complex interplay of CNS injuries, immune system dysregulation, sympathetic and parasympathetic pathways, and the endocrine system. The CNS environment, microglial activation, sympathetic outflow, stress hormone release, and glucocorticoid signaling collectively contribute to impaired function, reduced numbers, and dysregulation of T cells. Therefore, it is necessary to understand these mechanisms to develop targeted nanoparticle interventions that restore immune function and alleviate immunodepression after stroke.
Clinical Consequences of Immunodepression After Stroke
Immunosuppression after stroke has significant consequences for patients, leading to increased morbidity and mortality. A compromised immune system leaves stroke patients more vulnerable to infections, which can have severe implications. The following are the key points highlighting the consequences of immunosuppression after stroke: (1) Increased risk of infection:Citation78,Citation79 Immunodepression impairs the body’s ability to fight infections, increasing susceptibility to various infectious diseases. (2) Pneumonia: Aspiration pneumonia is a common and severe infection in stroke patients due to immobility, an impaired cough reflex, and compromised respiratory function. Immunodepression further weakens the defense mechanisms against bacterial colonization and lung infection. (3) Urinary tract infections:Citation80,Citation81 Bladder dysfunction in stroke patients increases the risk of urinary tract infections (UTIs). UTIs can progress to sepsis, a severe condition associated with a high mortality rate. (4) Other infections:Citation82 Stroke patients are also at increased risk of developing skin and soft tissue infections, bloodstream infections, and gastrointestinal infections, which can complicate their recovery and increase mortality rates. (5) Impact on overall health:Citation83–85 Prolonged immunosuppression not only affects the immediate poststroke period but also has long-term consequences.Citation6,Citation27,Citation86,Citation87 Chronic infections, delayed wound healing, and secondary complications can impact the overall health and survival of stroke patients.Citation88
Addressing immunosuppression as a major cause of death in stroke patients is crucial for improving outcomes. However, treating immunosuppression is challenging. Antibiotics alone are insufficient for restoring immune function, and the optimal timing and selection of immunomodulatory therapies are still being investigated.Citation89,Citation90 Stem cell therapyCitation91,Citation92 and personalized medicine approaches hold promise but require further research on their role in stroke-induced inflammation. Comprehensive poststroke care, including rehabilitation and supportive measures, is essential.Citation93 Therefore, it would be interesting to see that the combination of T-cell-based nanoparticle treatment with these methods could be a new avenue. Overcoming these challenges necessitates a deeper understanding of the mechanisms underlying immunosuppression and the development of targeted and personalized treatment strategies, especially nanoparticles. By addressing immunosuppression and preventing infections, we can significantly improve patient outcomes and reduce mortality rates in stroke patients.
Nanomaterials for Targeted Drug Delivery to T Cells
Nanomaterials have shown promise in various aspects of stroke research.Citation94,Citation95 They have been utilized for targeted drug delivery to the brain, neuroprotection, neuroregeneration, and immunomodulation. NPs, such as liposomes and polymeric NPs, have been designed to deliver therapeutic agents specifically to stroke-affected regions, enhancing treatment efficacy and minimizing off-target effects.Citation96,Citation97 Additionally, nanomaterials have been used to deliver neuroprotective agents, anti-inflammatory drugs, and immunomodulatory agents to mitigate neuroinflammation and promote tissue repair.Citation98,Citation99
While nanomaterials have shown potential for neuroprotection in stroke and for modulating immune responses, including their use in immunotherapy for cancer and other diseases, their specific application for reversing stroke-induced immunodepression is an area that is still under investigation. The use of nanomaterials for immunomodulation in the context of stroke is an emerging field of research, and further studies are needed to fully understand their effectiveness and potential in addressing immunodepression after stroke.
Current research on the use of nanomaterials for the treatment of stroke-induced immunosuppression faces several limitations. First, there is a lack of comprehensive studies in this specific area, with limited preclinical and clinical investigations. The translation of nanomaterials into clinical practice is still in its early stages.Citation100 Specifically, immunological responses and long-term safety concerns related to nanomaterials need to be thoroughly addressed. Moreover, scale-up and manufacturing challenges need to be overcome to ensure cost-effective production. Thus, the biological process, large-scale manufacturing and safety all need extensive improvement.Citation100 Additionally, designing nanomaterials with optimal properties for targeted therapy is complex, especially because efficiently crossing the BBB remains a challenge.Citation101,Citation102 The BBB is a self-protective layer that allows only particles that are small enough or lipid soluble to bypass this barrier. In 2022, MIT scientists developed nanoparticles that could be used as chemical drugs for brain glioblastoma infection in animal models, and particles coated with the AP2 peptide were found to be superior at penetrating the vessels surrounding tumors.Citation103 However, whether this basic research protocol could be translated into clinical trials requires further testing. Overcoming these limitations will require further research, interdisciplinary collaboration, and advancements in nanomaterial design and manufacturing processes to facilitate the effective translation of nanomaterial-based therapies for stroke-induced immunosuppression.Citation104
Nanomaterials offer a promising platform for targeted drug delivery to T cells in stroke therapy.Citation20 By utilizing nanocarriers, such as nanoparticles or liposomes, immunomodulatory drugs or therapeutic agents can be specifically delivered to T cells, enabling precise modulation of their function and immune response.Citation105,Citation106 This targeted approach provides several advantages over conventional drug delivery systems.Citation107,Citation108 First, nanomaterials can enhance the T-cell targeting ability.Citation109 By functionalizing the surface of nanocarriers with ligands or antibodies that recognize T-cell-specific markers or receptors, nanomaterials can selectively bind to T cells and facilitate their uptake.Citation110 This targeted binding increases the accumulation of drugs or therapeutic agents in T cells while minimizing off-target effects on other cell types. This specificity is particularly important in the context of stroke, where the modulation of T-cell function while minimizing interference with other immune cells or tissues is desired.Citation111 For instance, the combination of cell surface markers and nanoparticles has shown great potential in the treatment of cancer.Citation112 The 100 nm iron nanomaterials were modified with antibodies against CD137 (anti-CD137) and programmed death-ligand 1 (anti-PD-L1). Anti-PD-L1 antibodies blocked PD-L1–PD-1 interactions and thus prevented PD-1-mediated T-cell exhaustion, which showed that T cells could function well without exhaustion in an animal model.Citation112 Clinically, nanogels are nanodrug delivery systems (NDDSs) in which the drug is delivered as an IL-15 superagonist complex to treat various solid tumors and lymphomas and are now in a phase II clinical trial.Citation113 Second, nanomaterials allow for localized drug release.Citation21 The unique properties of nanocarriers can be harnessed to control the release of therapeutic agents in a spatial and temporal manner. Nanomaterials can be designed to respond to specific stimuli, such as pH, temperature, or enzymatic activity, which are characteristic of the T-cell microenvironment.Citation114 By incorporating stimuli-responsive components into the nanocarrier, drug release can be triggered specifically within T cells or within the vicinity of T-cell populations, ensuring efficient and localized therapeutic effects. This localized drug release minimizes systemic exposure and reduces the risk of off-target effects.
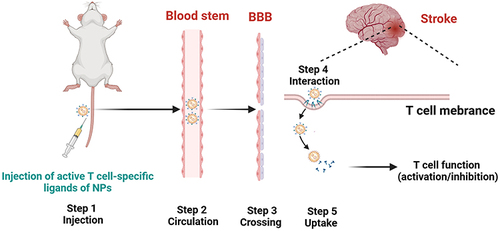
Moreover, nanomaterials can improve the stability and pharmacokinetics of immunomodulatory drugs or therapeutic agents.Citation115 Many drugs or bioactive molecules have limited stability or solubility, which can compromise their efficacy. Nanocarriers can protect these drugs from degradation and facilitate their transport to T cells, increasing their stability and bioavailability.Citation116,Citation117 Additionally, nanomaterials can prolong the circulation time of drugs in the bloodstream.Citation118 For instance, Maxim Nikitin’s group reported an improved method for enhancing the blood circulation time and performance of nanomedicines via the forced clearance of erythrocytes.Citation118 This kind of improvement allows sustained release and prolonged exposure of T cells, which is particularly important for achieving durable therapeutic effects. Furthermore, the small size of these nanomaterials enables efficient cellular uptake and intracellular drug delivery.Citation119 T cells possess specific mechanisms for internalizing nanoscale particles, making them highly receptive to nanocarrier-based drug delivery. Once internalized, nanocarriers can release their cargo directly into cells,Citation120,Citation121 ensuring efficient intracellular drug delivery and maximizing therapeutic potential. shows a series of steps illustrating the potential of a nanomaterial carrying an immunomodulatory drug from administration to T-cell targeting in the context of stroke. First, functionalized nanoparticles were intravenously injected with T-cell-specific ligands. Next, circulation in the bloodstream occurs with prolonged retention time due to surface modifications (eg, PEGylation). It is necessary to cross the BBB either passively (poststroke) or actively (using BBB permeation strategies). Then, these nanoparticles need to interact with T cells in inflamed brain tissue; therefore, the targeted cells can take up the nanoparticles by T cells through receptor-mediated endocytosis or pinocytosis. Finally, drugs can be released inside T cells, leading to the modulation of T-cell function (activation/inhibition).
Figure 3 A series of steps illustrating the journey of a nanomaterial carrying an immunomodulatory drug from administration to T-cell-targeting stroke therapy. Step 1: Intravenously inject the functionalized nanoparticles with T-cell-specific ligands. Step 2: Circulation in the bloodstream with prolonged retention time due to surface modifications (eg, PEGylation). Step 3: Crossing the blood‒brain barrier either passively (poststroke) or actively (using BBB permeation strategies). Step 4: T cells interact with T cells in inflamed brain tissue; the targeting ligand binds to a T-cell surface marker (eg, CD3 or CD4). Step 5: Uptake of the nanoparticles by T cells through receptor-mediated endocytosis or pinocytosis. Step 6: Drug release inside T cells leads to the modulation of T-cell function (activation/inhibition).
Based on the above discussion, there is a high possibility of utilizing nanomaterials for the targeted delivery of drugs to T cells in stroke therapy, which offers several advantages.Citation122–124 The advantages of nanomaterials in the precise delivery of drugs to T cells are shown in . By harnessing the unique properties of nanomaterials, it becomes possible to achieve precise modulation of T-cell function, attenuate immunodepression, and promote therapeutic effects in stroke patients (). Nanomaterial-based delivery systems hold great promise for the precise immunomodulation of T-cell function in stroke therapy. By incorporating immune checkpoint inhibitors, cytokines, or gene therapies into nanocarriers, it becomes possible to achieve targeted and controlled modulation of T-cell responses, optimizing the immune response and improving stroke outcomes. Further research and development in this area will undoubtedly contribute to advancing the field of stroke therapy and enhancing patient care.
Table 1 Advantages of Nanoparticles in the Precise Delivery of Drugs to T Cells
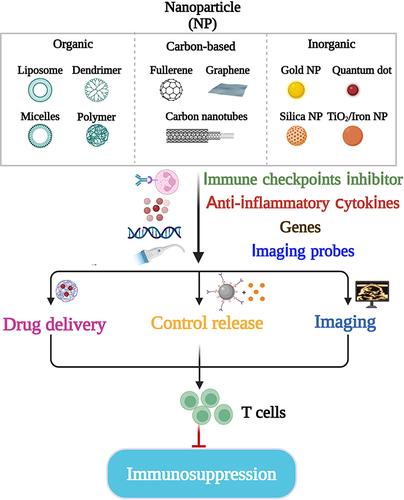
Figure 4 Illustration of potential strategies for targeting stroke-induced immunodepression via the use of nanomaterials. The diagram categorizes nanomaterials into three broad types: (1) organic materials, including liposomes, dendrimers, micelles, and polymers; (2) carbon-based materials, such as fullerenes and graphene; and (3) inorganic materials, such as gold nanoparticles and quantum dots. These nanomaterials can be engineered for a variety of applications to counter immunodepression. These applications include the delivery of therapeutic agents, controlled release of drugs, imaging of immune cell functions, targeting of immune checkpoints, modulation of inflammatory factors, and alteration of gene expression. The ultimate goal of these strategies is to attenuate the T-cell-mediated immunosuppression that occurs following stroke.
Using Nanoparticles to Modulate T-Cell Function
Immunomodulation of T-cell function plays a crucial role in stroke therapy, as T cells are key regulators of the immune response and can exert both beneficial and detrimental effects.Citation21,Citation135,Citation136 The specific material properties, design criteria, characteristics, and optimization strategies for these materials influence targeting efficacy and therapeutic outcomes, as discussed below.
Size
The size of the nanoparticles greatly impacts their biodistribution, cellular uptake, and ability to cross biological barriers such as the BBB. Generally, particles with sizes ranging from 10 to 200 nm are preferred because they exhibit longer circulation times and greater accumulation in the target tissue. Smaller nanoparticles (<200 nm) have a greater likelihood of crossing the compromised BBB after stroke, allowing for better penetration into the ischemic region where T cells accumulate.Citation137 An optimal size also facilitates endocytosis by T cells, ensuring effective drug delivery.Citation138
Surface Charge
The surface charge influences nanoparticle-cell interactions and colloidal stability. Cationic nanoparticles tend to have greater cellular uptake but can also cause cytotoxicity, while neutral or slightly negative charges can reduce nonspecific binding and improve biocompatibility.Citation139,Citation140 Modulating the surface charge to achieve a balance between cellular uptake and reduced toxicity is crucial for targeting T cells during stroke. Neutral or negatively charged nanoparticles can minimize nonspecific interactions and enhance the selective targeting of T cells via specific ligands.
Shape
Nanoparticle shape can affect cellular internalization pathways and clearance rates. Spherical shapes are common due to the ease of synthesis, but rod-shaped or discoidal particles may show preferential uptake by specific cell types.Citation95 Although the optimal shape for T-cell targeting in stroke has not been extensively studied, tailored shapes could enhance targeting efficiency if they match the uptake preferences of T cells.
Functionalization and Ligand Conjugation
Coating nanoparticles with targeting ligands (such as antibodies against T-cell surface markers such as CD3, CD4, or CD8) ensures specific recognition and binding to T cells. PEGylation can also be used to increase circulation time and stealth properties.Citation141 Selective targeting of T cells requires careful selection and attachment of ligands that recognize overexpressed receptors on these cells in the stroke environment.
Drug Loading Efficiency and Release Kinetics
NPs must have sufficient drug-loading capacity and controlled release kinetics to ensure that the appropriate amount of drug reaches the target cells at the appropriate time.Citation142–144 Optimization of drug loading methods and incorporation of stimuli-responsive components (eg, pH-sensitive linkers) can ensure the timely release of immunomodulatory agents upon reaching the acidic microenvironment of inflamed tissues where T cells are active.
Nanomaterials could offer a powerful platform for precisely modulating T-cell activation, proliferation, and differentiation, thereby influencing the immune response in stroke patients. This section focuses on the use of nanomaterials to deliver immune checkpoint inhibitors, cytokines, or gene therapies for targeted immunomodulation of T cells. One approach is to incorporate immune checkpoint inhibitors, such as antibodies against programmed cell death protein 1 (PD-1), as increasing evidence has shown that PD-1 plays an essential role in brain diseases, including stroke-induced neuroinflammation.Citation145–147 PD-L1 monoclonal antibodies treat ischemic stroke by controlling central nervous system inflammation.Citation148 Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) is another key T-cell immune checkpoint molecule that has evolved in idiopathic ischemic stroke.Citation149 These inhibitors can block the inhibitory signals that suppress T-cell activation, effectively enhancing T-cell responses against stroke-associated antigens. By encapsulating immune checkpoint inhibitors in nanomaterials, their stability can be improved, and their targeted delivery to T cells can be achieved. In a Chinese cohort, the serum CTLA-4 concentration was significantly greater in hypertensive patients with ischemic stroke than in hypertensive patients without ischemic stroke.Citation150 Therefore, this targeted delivery allows for higher local concentrations of inhibitors at the site of action, minimizing systemic side effects. Additionally, nanomaterials can be designed to provide controlled release of immune checkpoint inhibitors, ensuring sustained immunomodulation and prolonged therapeutic effects. Another strategy involves the delivery of cytokines to T cells using nanocarriers. For example, McHugh et al demonstrated the paracrine codelivery of Transforming growth factor-β (TGF-β) and IL-2 using CD4-targeted nanoparticles for the induction and maintenance of regulatory T cells.Citation150 Cytokines play critical roles in regulating T-cell function, proliferation, and differentiation. By encapsulating cytokines, such as interleukins (eg, IL-2 and IL-15), into nanomaterials, their stability and bioavailability can be enhanced, and targeted delivery to T cells can be achieved. This targeted delivery allows for precise modulation of T-cell responses in stroke. Moreover, nanomaterials can provide controlled release of cytokines, enabling sustained exposure and preventing the rapid clearance of cytokines in the bloodstream. This controlled release ensures that T cells receive the appropriate signals for prolonged and optimized immune activation. Furthermore, nanomaterials can facilitate the delivery of gene therapies for T-cell modulation.Citation151,Citation152 Gene therapies, such as the introduction of chimeric antigen receptors (CARs) or genetic modifications to enhance T-cell function, hold great potential in stroke therapy. Nanocarriers can protect and deliver therapeutic genes to T cells, allowing precise genetic modifications and controlled expression of therapeutic molecules. By incorporating gene therapies into nanomaterials, targeted delivery to T cells can be achieved, enhancing their therapeutic efficacy and minimizing off-target effects.Citation122
Multifunctional Nanoplatforms for T-Cell Modulation
The design and development of multifunctional nanoplatforms have emerged as promising approaches for simultaneously targeting neuroinflammation and T-cell-mediated immunodepression in the context of stroke.Citation123 These nanoplatforms integrate therapeutics and immunomodulatory agents within a single system, providing a comprehensive solution for precise and effective T-cell modulation.Citation123 These nanoplatforms can be loaded with various therapeutics, including neuroprotective agents, anti-inflammatory drugs, immune checkpoint inhibitors, or cytokines, to address different aspects of stroke pathology. The following summarizes some T-cell nanoparticle design targeting mechanisms in stroke models by.
Liposomes
Liposomes functionalized with specific antibodies or ligands that bind to receptors overexpressed on T cells, such as CD3 or CD4, have been developed. For example, PEGylated liposomes conjugated with an anti-CD4 antibody can specifically bind to CD4+ T cells.Citation124,Citation153 Alternatively, they can be decorated with peptides that home to inflamed tissues where T cells accumulate after stroke. After stroke, inflammation, including the infiltration of T cells into the brain, increases. By incorporating drugs that regulate T-cell function (immunomodulatory agents) into targeted liposomes, they can reach the desired site of action more effectively, modulating the immune response and reducing inflammation.
Micelles
Like liposomes, micelles can be modified with T-cell-specific ligands or antibodies. They can also utilize T-cell-homing peptides or aptamers that recognize unique markers expressed on T cells during stroke. Upon recognition and binding, micelles can encapsulate immunomodulatory agents and release them slowly near T cells, thus minimizing off-target effects. Their small size enhances cellular uptake, making it easier for them to deliver cargo to T cells in the brain microenvironment.Citation144
Polymeric Nanoparticles
Polymers can be engineered to contain T-cell-specific ligands or antibodies directly within the polymer matrix or attached to its surface. For example, PLGA nanoparticles conjugated with anti-CD3 antibodies can selectively target T cells.Citation144,Citation154,Citation155 In the context of stroke, polymeric nanoparticles can transport drugs across the blood‒brain barrier and target activated T cells within the ischemic brain. The controlled release of these particles ensures sustained drug exposure to T cells, potentially reducing inflammation and improving stroke outcomes.
Dendrimers
Dendrimers possess numerous terminal functional groups that can be chemically modified with T-cell-specific ligands. Some dendrimers can also translocate across the BBB and interact with T cells expressing specific receptors. For instance, cationic dendrimers can be efficiently internalized into T cells due to electrostatic interactions.Citation156,Citation157 Dendrimers can be designed to carry and deliver immunomodulatory cargoes directly to infiltrating T cells in the ischemic brain, modulating the immune response and alleviating secondary brain injury.
In summary, the success of T-cell targeting in stroke models depends on the efficient design of nanoparticles that can recognize and bind to T-cell surface markers, overcome biological barriers (such as the BBB), and provide controlled release of immunomodulatory drugs at the site of inflammation. These approaches represent innovative strategies for precision medicine in stroke therapeutics.
One successful example is from the Dr. Roel Hammink group, in which the ex vivo expansion of T cells by artificial antigen-presenting cells (aAPCs) was considered to be a limiting factor for T-cell activation. They engineered nanosized immunofilaments (IFs) with a soluble semiflexible polyisocyanopeptide backbone, which is a major histocompatibility complex (MHC). Thus, this nanosized IF could activate and expand antigen-specific T cells such as APCs.Citation158 Neuroprotective agents help minimize neuronal damage and promote tissue repair, while anti-inflammatory drugs reduce neuroinflammation and mitigate the detrimental effects of excessive immune responses. Immune checkpoint inhibitors enhance T-cell activation and effector functions, and cytokines promote the differentiation and proliferation of T cells. The incorporation of these therapeutics into nanoplatforms allows for controlled release, prolonged release, and targeted delivery to the stroke site, maximizing therapeutic efficacy while minimizing off-target effects.
Overall, multifunctional nanoplatforms hold great promise for simultaneous targeting of neuroinflammation and T-cell-mediated immunodepression in stroke treatment. By integrating therapeutics and immunomodulatory agents, these nanoplatforms provide a comprehensive solution for precise T-cell modulation and effective stroke treatment. Further research and development in this field will pave the way for innovative nanotechnology-based strategies to improve stroke outcomes and promote neurorecovery.
Innovative Approaches for Characterization and Monitoring
In recent years, significant advancements have been made in the field of nanosensors and imaging techniques,Citation159 enabling real-time monitoring and characterization of T-cell responses and immunomodulation in the context of stroke. These innovative approaches offer valuable insights into the dynamic changes occurring in the immune system and provide a basis for personalized and precise treatment options. Nanosensors are highly sensitive devices capable of detecting and measuring specific biological markers or signals at the nanoscale.Citation159,Citation160 By integrating the advantages of nanomaterials and sensing factors, CVD can be rapidly diagnosed.Citation160 By integrating nanosensors into nanomaterial-based systems, it is possible to monitor T-cell responses in real time, providing valuable information about their activation, proliferation, and functional status. For example, the use of nanosensors could provide immediate and impactful detection of acute T-cell-mediated transplant rejection.Citation161 Moreover, nanosensors can be engineered to detect the secretion of cytokines or the expression of specific surface markers on T cells, allowing quantitative assessment of the immune response.Citation162,Citation163 This real-time monitoring of T-cell behavior could help researchers better understand the underlying mechanisms of immunodepression in stroke patients and evaluate the effectiveness of therapeutic interventions.
Imaging techniques play a crucial role in characterizing and monitoring T-cell responses and immunomodulation. Advanced imaging modalities, such as positron emission tomography (PET), magnetic resonance imaging (MRI), or optical imaging, can be combined with nanomaterials to provide detailed visualization of T-cell distribution, migration, and interaction with the stroke-affected region.Citation164–166 For instance, nanomaterials labeled with specific imaging agents could be administered to track T-cell infiltration into the brain and assess their localization within neuroinflammatory sites. Furthermore, molecular imaging techniques can be employed to detect specific biomarkers associated with T-cell activation or immunomodulatory processes, providing insights into the efficacy of nanomaterial-based therapies.
The integration of nanotechnology with biomarkers and imaging modalities offers exciting prospects for personalized and precise treatment options in stroke patients. By identifying specific biomarkers associated with immunodepression or T-cell dysfunction in individual patients, clinicians can tailor treatment strategies to target those specific abnormalities. Nanotechnology-based approaches can then be employed to deliver therapeutics, immunomodulatory agents, or gene therapies directly to the affected areas, ensuring targeted and efficient intervention. Moreover, real-time monitoring of T-cell responses using nanosensors and imaging techniques can guide treatment decisions, enabling clinicians to adjust therapeutic protocols based on the observed immune dynamics.
In summary, innovative approaches combining nanosensors, imaging techniques, and biomarkers provide valuable tools for characterizing and monitoring T-cell responses and immunomodulation in stroke patients. These advancements allow real-time assessment of T-cell behavior, localization, and functional status, leading to personalized treatment options and precise interventions. Further research in this area holds great potential for optimizing stroke management and improving patient outcomes.
Challenges and Future Perspectives
While nanomaterial-based strategies for targeting T-cell-mediated immunodepression in stroke patients show great promise, several challenges need to be addressed to facilitate their clinical translation. These challenges include ensuring the biocompatibility, stability, and scalability of nanomaterials, as well as fostering interdisciplinary collaborations for accelerated development and optimization of these strategies.
First, the biocompatibility of nanomaterials is of utmost importance for ensuring their safe use in clinical applications. Comprehensive biocompatibility assessments are necessary to evaluate the potential cytotoxicity, immunogenicity, and long-term effects of nanomaterials on the human body. Understanding the interactions between nanomaterials and biological systems is crucial for mitigating any adverse effects and ensuring their safety profile. Additionally, the stability of nanomaterials, including their physicochemical properties, drug loading efficiency, and controlled release mechanisms, must be optimized to maintain their therapeutic efficacy throughout the treatment duration. Despite promising results in preclinical models, ensuring adequate circulation time and specific accumulation of nanomaterials at targeted T-cell sites remains challenging. Achieving the right balance between stability and biodegradability to avoid rapid clearance and maintain drug concentration at the target is crucial.Citation167
Scalability is also a significant challenge in the clinical translation of nanomaterial-based strategies. The manufacturing processes of nanomaterials need to be scalable and reproducible to meet the demands of large-scale production for clinical applications. This involves developing robust and cost-effective fabrication methods, optimizing formulation parameters, and ensuring batch-to-batch consistency. The scalability of nanomaterials is essential for facilitating their widespread use in clinical settings and enabling their accessibility to patients.
Another important issue is toxicity and body immune response. Nanomaterials may trigger unforeseen immune responses or induce toxicity in the body. Long-term safety evaluations and the use of biocompatible materials are essential before clinical translation. Specifically, our previous study showed that the immune response plays a pivotal role in stroke recovery.Citation168 Inhibiting the proinflammatory response in the acute phase while increasing the anti-inflammatory response in the recovery stage could benefit the recovery process.Citation169 Here, we need to emphasize that immune cells themselves could function as vehicles. Engineering nanoparticles to be taken up by monocytes/macrophages and subsequently transported across the BBB when these cells migrate into brain tissue is another approach. Our published results showed that systemically delivering the nanoparticle Maclpil short interfering RNA (siRNA) could alleviate experimental ischemic stroke by promoting macrophage apoptosis and anti-inflammatory activation.Citation19
Blood‒brain barrier penetration should also be considered when designing nanoparticles to treat stroke. While some nanomaterials can cross the BBB under certain circumstances (eg, after stroke when the BBB is disrupted), designing nanoparticles that can consistently penetrate the healthy or mildly compromised BBB remains a significant challenge.Citation170 Nanoparticles with a diameter of approximately 20–80 nm can potentially cross the BBB more easily than larger particles. Surface modification with polyethylene glycol (PEG) can increase circulation time and reduce clearance from the bloodstream, increasing the chances of BBB penetration. When nanoparticles are functionalized with ligands that bind to receptors expressed on BBB endothelial cells, receptor-mediated transcytosis can be triggered. For example, transferrin, insulin, and low-density lipoprotein (LDL) receptors are commonly targeted to facilitate transport across the BBB.Citation171 Notably, ultrasound and magnetic fields provide a novel method for nanoparticle transport, and utilizing focused ultrasound (US) in combination with microbubbles or magnetic fields with magnetic nanoparticles can transiently disrupt the BBB, creating temporary openings for nanoparticles to pass through.Citation172
Furthermore, regulatory approval for nanomedicine products is complex due to the novelty of the technology. Rigorous characterization, standardization, and quality control measures are necessary to satisfy regulatory requirements.
To overcome these challenges, interdisciplinary collaboration is crucial. Researchers from diverse fields, including materials science, nanotechnology, immunology, neuroscience, and clinical medicine, need to work together to exchange knowledge, share expertise, and collaborate on the development of nanomaterial-based strategies. Interdisciplinary collaborations can foster the design of innovative nanomaterials with enhanced functionality and performance and accelerate preclinical and clinical evaluation of these strategies. By pooling resources and expertise, researchers can address the complex challenges associated with nanomaterial-based immunomodulation in stroke and pave the way for successful clinical translation of these materials.
In conclusion, while nanomaterial-based strategies hold great promise for targeting T-cell-mediated immunosuppression in stroke, several challenges need to be overcome for successful clinical translation of these materials. Addressing the biocompatibility, stability, and scalability of nanomaterials, as well as promoting interdisciplinary collaboration, will be critical for advancing these strategies toward clinical application. By addressing these challenges and fostering collaborative efforts, we can unlock the full potential of nanomaterials in revolutionizing stroke treatment and improving patient outcomes in the future.
Conclusion
Although there are no published reports on the use of T-cell nanoparticles for treating stroke, clinical trials using nanomaterials aimed at treating stroke, including magnetic nanorobots, are ongoing (). Nanomaterials hold promise for targeting neuroinflammation and attenuating T-cell-mediated immunosuppression in stroke patients. However, further research is needed to validate the efficacy and safety of these methods. Preclinical studies should assess therapeutic outcomes and evaluate biodistribution and long-term effects. Clinical trials should focus on relevant outcomes and include long-term follow-up. Standardized protocols are essential for reproducibility. With continued investigation, nanomaterial-based interventions targeting T cells could revolutionize stroke treatment and improve outcomes.
Table 2 Clinical Nanomaterial-Based Strategies for Treating Stroke
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics-2020 update: a report from the American heart association. Circulation. 2020;141(9):e139–e596. doi:10.1161/CIR.0000000000000757
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2022 update: a report from the American heart association. Circulation. 2022;145(8):e153–e639. doi:10.1161/CIR.0000000000001052
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics--2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–322. doi:10.1161/CIR.0000000000000152
- Shi K, Wood K, Shi F-D, et al. Stroke-induced immunosuppression and poststroke infection. Stroke Vasc Neurol. 2018;3(1):34–41. doi:10.1136/svn-2017-000123
- Fu Y, Liu Q, Anrather J, et al. Immune interventions in stroke. Nat Rev Neurol. 2015;11(9):524–535. doi:10.1038/nrneurol.2015.144
- Westendorp WF, Dames C, Nederkoorn PJ, et al. Immunodepression, infections, and functional outcome in ischemic stroke. Stroke. 2022;53(5):1438–1448. doi:10.1161/STROKEAHA.122.038867
- Chamorro Á, Meisel A, Planas AM, et al. The immunology of acute stroke. Nat Rev Neurol. 2012;8(7):401–410. doi:10.1038/nrneurol.2012.98
- Iadecola C, Anrather J. The immunology of stroke: from mechanisms to translation. Nat Med. 2011;17(7):796–808. doi:10.1038/nm.2399
- Zhang S, Liu C, Sun J, et al. Bridging the gap: investigating the link between inflammasomes and postoperative cognitive dysfunction. Aging Dis. 2023;14(6):1981–2002. doi:10.14336/AD.2023.0501
- Zhao H, Luan X, Wang Y, et al. Dynamic detection of specific membrane capacitance and cytoplasmic resistance of neutrophils after ischemic stroke. Aging Dis. 2023;14(4):1035–1037. doi:10.14336/AD.2023.0127
- Xiong X, Gu L, Wang Y, et al. Glycyrrhizin protects against focal cerebral ischemia via inhibition of T cell activity and HMGB1-mediated mechanisms. J Neuroinflammation. 2016;13(1):241. doi:10.1186/s12974-016-0705-5
- Gu L, Xiong X, Zhang H, et al. Distinctive effects of T cell subsets in neuronal injury induced by cocultured splenocytes in vitro and by in vivo stroke in mice. Stroke. 2012;43(7):1941–1946. doi:10.1161/STROKEAHA.112.656611
- Yao Y, Li Y, Ni W, et al. Systematic study of immune cell diversity in ischemic postconditioning using high-dimensional single-cell analysis with mass cytometry. Aging Dis. 2021;12(3):812–825. doi:10.14336/AD.2020.1115
- Gu L, Xiong X, Wei D, et al. T cells contribute to stroke-induced lymphopenia in rats. PLoS One. 2013;8(3):e59602.
- Ahmed R, Amreddy N, Babu A, et al. Combinatorial nanoparticle delivery of siRNA and antineoplastics for lung cancer treatment. Methods Mol Biol. 2019;1974:265–290.
- Jyotsana N, Sharma A, Chaturvedi A, et al. Lipid nanoparticle-mediated siRNA delivery for safe targeting of human CML in vivo. Ann Hematol. 2019;98(8):1905–1918. doi:10.1007/s00277-019-03713-y
- Zatsepin TS, Kotelevtsev YV, Koteliansky V. Lipid nanoparticles for targeted siRNA delivery - going from bench to bedside. Int J Nanomed. 2016;11:3077–3086. doi:10.2147/IJN.S106625
- Tsai YC, Vijayaraghavan P, Chiang W-H, et al. Targeted delivery of functionalized upconversion nanoparticles for externally triggered photothermal/photodynamic therapies of brain glioblastoma. Theranostics. 2018;8(5):1435–1448. doi:10.7150/thno.22482
- Wang Y, Liu C, Chen Y, et al. Systemically silencing long non-coding RNAs maclpil with short interfering RNA nanoparticles alleviates experimental ischemic stroke by promoting macrophage apoptosis and anti-inflammatory activation. Front Cardiovasc Med. 2022;9:876087. doi:10.3389/fcvm.2022.876087
- Schmid D, Park CG, Hartl CA, et al. T cell-targeting nanoparticles focus delivery of immunotherapy to improve antitumor immunity. Nat Commun. 2017;8(1):1747. doi:10.1038/s41467-017-01830-8
- Gong N, Sheppard NC, Billingsley MM, et al. Nanomaterials for T-cell cancer immunotherapy. Nat Nanotechnol. 2021;16(1):25–36. doi:10.1038/s41565-020-00822-y
- Wauters AC, Scheerstra JF, Vermeijlen IG, et al. Artificial antigen-presenting cell topology dictates T cell activation. ACS Nano. 2022;16(9):15072–15085. doi:10.1021/acsnano.2c06211
- Meyer RA, Sunshine JC, Perica K, et al. Biodegradable nanoellipsoidal artificial antigen presenting cells for antigen specific T-cell activation. Small. 2015;11(13):1519–1525. doi:10.1002/smll.201402369
- Oh J, Xia X, Wong WKR, et al. The effect of the nanoparticle shape on T cell activation. Small. 2022;18(36):e2107373. doi:10.1002/smll.202107373
- Wang T, Zhang H, Han Y, et al. Reversing T cell dysfunction to boost glioblastoma immunotherapy by paroxetine-mediated GRK2 inhibition and blockade of multiple checkpoints through biomimetic nanoparticles. Adv Sci (Weinh). 2023;10(9):e2204961. doi:10.1002/advs.202204961
- Hey G, Bhutani S, Woolridge MG, et al. immunologic implications for stroke recovery: unveiling the role of the immune system in pathogenesis, neurorepair, and rehabilitation. J Cell Immunol. 2023;5(3):65–81. doi:10.33696/immunology.5.170
- Faura J, Bustamante A, Miró-Mur F, et al. Stroke-induced immunosuppression: implications for the prevention and prediction of post-stroke infections. J Neuroinflammation. 2021;18(1):127. doi:10.1186/s12974-021-02177-0
- Luckheeram RV, Zhou R, Verma AD, et al. CD4 + T cells: differentiation and functions. Clin Dev Immunol. 2012;2012:925135. doi:10.1155/2012/925135
- Laidlaw BJ, Craft JE, Kaech SM. The multifaceted role of CD4(+) T cells in CD8(+)T cell memory. Nat Rev Immunol. 2016;16(2):102–111. doi:10.1038/nri.2015.10
- Gill D, Veltkamp R. Dynamics of T cell responses after stroke. Curr Opin Pharmacol. 2016;26:26–32. doi:10.1016/j.coph.2015.09.009
- Zhang D, Ren J, Luo Y, et al. T cell response in ischemic stroke: from mechanisms to translational insights. Front Immunol. 2021;12:707972. doi:10.3389/fimmu.2021.707972
- Seder RA, Ahmed R. Similarities and differences in CD4+ and CD8+ effector and memory T cell generation. Nat Immunol. 2003;4(9):835–842. doi:10.1038/ni969
- Braun M, Vaibhav K, Saad N, et al. Activation of Myeloid TLR4 mediates T lymphocyte polarization after traumatic brain injury. J Immunol. 2017;198(9):3615–3626. doi:10.4049/jimmunol.1601948
- Ferrick DA, Schrenzel MD, Mulvania T, et al. Differential production of interferon-gamma and interleukin-4 in response to Th1- and Th2-stimulating pathogens by gamma delta T cells in vivo. Nature. 1995;373(6511):255–257. doi:10.1038/373255a0
- Li J, Zeng Z, Wu Q, et al. Immunological modulation of the Th1/Th2 shift by ionizing radiation in tumors (Review). Int J Oncol. 2021;59(1). doi:10.3892/ijo.2021.5230
- Walker JA, McKenzie ANJ. TH2 cell development and function. Nat Rev Immunol. 2018;18(2):121–133. doi:10.1038/nri.2017.118
- Brennan PJ, Brigl M, Brenner MB. Invariant natural killer T cells: an innate activation scheme linked to diverse effector functions. Nat Rev Immunol. 2013;13(2):101–117. doi:10.1038/nri3369
- Rana J, Biswas M. Regulatory T cell therapy: current and future design perspectives. Cell Immunol. 2020;356:104193. doi:10.1016/j.cellimm.2020.104193
- Vignali DA, Collison LW, Workman CJ. How regulatory T cells work. Nat Rev Immunol. 2008;8(7):523–532. doi:10.1038/nri2343
- Wang H, Wang Z, Wu Q, et al. Regulatory T cells in ischemic stroke. CNS Neurosci Ther. 2021;27(6):643–651. doi:10.1111/cns.13611
- Stubbe T, Ebner F, Richter D, et al. Regulatory T cells accumulate and proliferate in the ischemic hemisphere for up to 30 days after MCAO. J Cereb Blood Flow Metab. 2013;33(1):37–47. doi:10.1038/jcbfm.2012.128
- Kleinschnitz C, Kraft P, Dreykluft A, et al. Regulatory T cells are strong promoters of acute ischemic stroke in mice by inducing dysfunction of the cerebral microvasculature. Blood. 2013;121(4):679–691. doi:10.1182/blood-2012-04-426734
- Ruhnau J, Schulze J, von Sarnowski B, et al. Reduced numbers and impaired function of regulatory T cells in peripheral blood of ischemic stroke patients. Mediators Inflamm. 2016;2016:2974605. doi:10.1155/2016/2974605
- Song J, Kim YK. Animal models for the study of depressive disorder. CNS Neurosci Ther. 2021;27(6):633–642. doi:10.1111/cns.13622
- Offner H, Subramanian S, Parker SM, et al. Splenic atrophy in experimental stroke is accompanied by increased regulatory T cells and circulating macrophages. J Immunol. 2006;176(11):6523–6531. doi:10.4049/jimmunol.176.11.6523
- Stoll G, Nieswandt B. Thrombo-inflammation in acute ischaemic stroke - implications for treatment. Nat Rev Neurol. 2019;15(8):473–481. doi:10.1038/s41582-019-0221-1
- Guardalupi F, Sorrentino C, Corradi G, et al. A pro-inflammatory environment in bone marrow of Treg transplanted patients matches with graft-versus-leukemia effect. Leukemia. 2023;37(7):1572–1575. doi:10.1038/s41375-023-01932-x
- Zhang W, Xiao D, Mao Q, et al. Role of neuroinflammation in neurodegeneration development. Signal Transduct Target Ther. 2023;8(1):267. doi:10.1038/s41392-023-01486-5
- Oparaugo NC, Ouyang K, Nguyen NP, et al. Human regulatory T cells: understanding the role of tregs in select autoimmune skin diseases and post-transplant nonmelanoma skin cancers. Int J Mol Sci. 2023;24(2):1527.
- Wang M, Thomson AW, Yu F, et al. Regulatory T lymphocytes as a therapy for ischemic stroke. Semin Immunopathol. 2023;45(3):329–346. doi:10.1007/s00281-022-00975-z
- Halvorson T, Tuomela K, Levings MK. Targeting regulatory T cell metabolism in disease: novel therapeutic opportunities. Eur J Immunol. 2023;53(9):e2250002. doi:10.1002/eji.202250002
- Leijte GP, Rimmelé T, Kox M, et al. Monocytic HLA-DR expression kinetics in septic shock patients with different pathogens, sites of infection and adverse outcomes. Crit Care. 2020;24(1):110. doi:10.1186/s13054-020-2830-x
- Asmussen A, Busch H-J, Helbing T, et al. Monocyte subset distribution and surface expression of HLA-DR and CD14 in patients after cardiopulmonary resuscitation. Sci Rep. 2021;11(1):12403. doi:10.1038/s41598-021-91948-z
- Ziqing Z, Yunpeng L, Yiqi L, et al. Friends or foes: the mononuclear phagocyte system in ischemic stroke. Brain Pathol. 2023;33(2):e13151. doi:10.1111/bpa.13151
- Chapman NM, Chi H. Metabolic adaptation of lymphocytes in immunity and disease. Immunity. 2022;55(1):14–30. doi:10.1016/j.immuni.2021.12.012
- Achmus L, Ruhnau J, Grothe S, et al. Stroke-induced modulation of myeloid-derived suppressor cells (MDSCs) and IL-10-producing regulatory monocytes. Front Neurol. 2020;11:577971. doi:10.3389/fneur.2020.577971
- Platzer C, Döcke W-D, Volk H-D, et al. Catecholamines trigger IL-10 release in acute systemic stress reaction by direct stimulation of its promoter/enhancer activity in monocytic cells. J Neuroimmunol. 2000;105(1):31–38. doi:10.1016/S0165-5728(00)00205-8
- Qin C, Yang S, Chu Y-H, et al. Signaling pathways involved in ischemic stroke: molecular mechanisms and therapeutic interventions. Signal Transduct Target Ther. 2022;7(1):215. doi:10.1038/s41392-022-01064-1
- Jiang M, Yin P, Bai X, et al. Proinflammatory and anti-inflammatory genes in stroke pathogenesis. Curr Pharm Des. 2020;26(34):4220–4233. doi:10.2174/1381612826666200701212859
- Meisel C, Schwab JM, Prass K, et al. Central nervous system injury-induced immune deficiency syndrome. Nat Rev Neurosci. 2005;6(10):775–786. doi:10.1038/nrn1765
- Anrather J, Iadecola C. Inflammation and Stroke: an Overview. Neurotherapeutics. 2016;13(4):661–670. doi:10.1007/s13311-016-0483-x
- Piepke M, Clausen BH, Ludewig P, et al. Interleukin-10 improves stroke outcome by controlling the detrimental Interleukin-17A response. J Neuroinflammation. 2021;18(1):265. doi:10.1186/s12974-021-02316-7
- Alsbrook DL, Di Napoli M, Bhatia K, et al. Neuroinflammation in acute ischemic and hemorrhagic stroke. Curr Neurol Neurosci Rep. 2023;23(8):407–431. doi:10.1007/s11910-023-01282-2
- Dong C. Cytokine regulation and function in T cells. Annu Rev Immunol. 2021;39:51–76. doi:10.1146/annurev-immunol-061020-053702
- Wang YR, Cui W-Q, Wu H-Y, et al. The role of T cells in acute ischemic stroke. Brain Res Bull. 2023;196:20–33. doi:10.1016/j.brainresbull.2023.03.005
- Bishop EL, Gudgeon N, Dimeloe S. Control of T cell metabolism by cytokines and hormones. Front Immunol. 2021;12:653605. doi:10.3389/fimmu.2021.653605
- Dirnagl U, Klehmet J, Braun JS, et al. Stroke-induced immunodepression: experimental evidence and clinical relevance. Stroke. 2007;38(2 Suppl):770–773. doi:10.1161/01.STR.0000251441.89665.bc
- Urra X, Obach V, Chamorro A. Stroke induced immunodepression syndrome: from bench to bedside. Curr Mol Med. 2009;9(2):195–202. doi:10.2174/156652409787581574
- Stanzione R, Forte M, Cotugno M, et al. Role of DAMPs and of leukocytes infiltration in ischemic stroke: insights from animal models and translation to the human disease. Cell Mol Neurobiol. 2022;42(3):545–556. doi:10.1007/s10571-020-00966-4
- Li LZ, Huang -Y-Y, Yang Z-H, et al. Potential microglia-based interventions for stroke. CNS Neurosci Ther. 2020;26(3):288–296. doi:10.1111/cns.13291
- Zeng J, Bao T, Yang K, et al. The mechanism of microglia-mediated immune inflammation in ischemic stroke and the role of natural botanical components in regulating microglia: a review. Front Immunol. 2022;13:1047550. doi:10.3389/fimmu.2022.1047550
- Karakas M, Koenig W. Sympathetic nervous system: a crucial player modulating residual cardiovascular risk. Circ Res. 2013;112(1):13–16. doi:10.1161/CIRCRESAHA.112.281097
- Winklewski PJ, Radkowski M, Demkow U. Cross-talk between the inflammatory response, sympathetic activation and pulmonary infection in the ischemic stroke. J Neuroinflammation. 2014;11:213. doi:10.1186/s12974-014-0213-4
- Heeg M, Kaech S. Sympathetic nerves suppress T-cell responses in infection and in cancer. Nature. 2023;2023:1. doi:10.1038/d41586-023-02776-2
- Mueller SN. Neural control of immune cell trafficking. J Exp Med. 2022;219(3). doi:10.1084/jem.20211604
- Franceschini R, Tenconi GL, Zoppoli F, et al. Endocrine abnormalities and outcome of ischaemic stroke. Biomed Pharmacother. 2001;55(8):458–465. doi:10.1016/S0753-3322(01)00086-5
- Datta A, Saha C, Godse P, et al. Neuroendocrine regulation in stroke. Trends Endocrinol Metab. 2023;34(5):260–277. doi:10.1016/j.tem.2023.02.005
- Elkind MSV, Boehme AK, Smith CJ, et al. Infection as a stroke risk factor and determinant of outcome after stroke. Stroke. 2020;51(10):3156–3168. doi:10.1161/STROKEAHA.120.030429
- Divani AA, Andalib S, Di Napoli M, et al. Coronavirus Disease 2019 and stroke: clinical manifestations and pathophysiological insights. J Stroke Cerebrovasc Dis. 2020;29(8):104941. doi:10.1016/j.jstrokecerebrovasdis.2020.104941
- Poisson SN, Johnston SC, Josephson SA. Urinary tract infections complicating stroke: mechanisms, consequences, and possible solutions. Stroke. 2010;41(4):e180–4. doi:10.1161/STROKEAHA.109.576413
- Ahmed R, Mhina C, Philip K, et al. Age- and sex-specific trends in medical complications after acute ischemic stroke in the United States. Neurology. 2023;100(12):e1282–e1295. doi:10.1212/WNL.0000000000206749
- Donkor ES. Stroke in the 21st Century: a Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res Treat. 2018;2018:3238165. doi:10.1155/2018/3238165
- Muñoz Venturelli P, Li X, Middleton S, et al. Impact of evidence-based stroke care on patient outcomes: a multilevel analysis of an international study. J Am Heart Assoc. 2019;8(13):e012640. doi:10.1161/JAHA.119.012640
- Minhas JS, Wang X, Lavados PM, et al. Blood pressure variability and outcome in acute ischemic and hemorrhagic stroke: a post hoc analysis of the HeadPoST study. J Hum Hypertens. 2019;33(5):411–418. doi:10.1038/s41371-019-0193-z
- Group GNDC, Abajobir AA, Abate KH. Global, regional, and national burden of neurological disorders during 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet Neurol. 2017;16(11):877–897. doi:10.1016/S1474-4422(17)30299-5
- Santos Samary C, Pelosi P, Leme Silva P, et al. Immunomodulation after ischemic stroke: potential mechanisms and implications for therapy. Crit Care. 2016;20(1):391. doi:10.1186/s13054-016-1573-1
- Shim R, Wong CHY. Complex interplay of multiple biological systems that contribute to post-stroke infections. Brain Behav Immun. 2018;70:10–20. doi:10.1016/j.bbi.2018.03.019
- Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017;34(3):599–610. doi:10.1007/s12325-017-0478-y
- Marto JP, Strambo D, Livio F, et al. Drugs associated with ischemic stroke: a review for clinicians. Stroke. 2021;52(10):e646–e659. doi:10.1161/STROKEAHA.120.033272
- Liu L, Xiong X-Y, Zhang Q, et al. The efficacy of prophylactic antibiotics on post-stroke infections: an updated systematic review and meta-analysis. Sci Rep. 2016;6:36656. doi:10.1038/srep36656
- Wechsler LR, Bates D, Stroemer P, et al. Cell therapy for chronic stroke. Stroke. 2018;49(5):1066–1074. doi:10.1161/STROKEAHA.117.018290
- Richards LG, Cramer SC. Advances in stroke recovery therapeutics. Stroke. 2022;53(1):260–263. doi:10.1161/STROKEAHA.121.038018
- Duncan PW, Bushnell C, Sissine M, et al. Comprehensive stroke care and outcomes: time for a paradigm shift. Stroke. 2021;52(1):385–393. doi:10.1161/STROKEAHA.120.029678
- Shcharbina N, Shcharbin D, Bryszewska M. Nanomaterials in stroke treatment: perspectives. Stroke. 2013;44(8):2351–2355. doi:10.1161/STROKEAHA.113.001298
- Song G, Zhao M, Chen H, et al. The role of nanomaterials in stroke treatment: targeting oxidative stress. Oxid Med Cell Longev. 2021;2021:8857486. doi:10.1155/2021/8857486
- Yuan J, Li L, Yang Q, et al. Targeted treatment of ischemic stroke by bioactive nanoparticle-derived reactive oxygen species responsive and inflammation-resolving nanotherapies. ACS Nano. 2021;15(10):16076–16094. doi:10.1021/acsnano.1c04753
- Bonnard T, Gauberti M, Martinez de Lizarrondo S, et al. Recent advances in nanomedicine for ischemic and hemorrhagic stroke. Stroke. 2019;50(5):1318–1324. doi:10.1161/STROKEAHA.118.022744
- Dong X, Gao J, Su Y, et al. Nanomedicine for ischemic stroke. Int J Mol Sci. 2020;21(20):7600. doi:10.3390/ijms21207600
- Amani H, Habibey R, Shokri F, et al. Selenium nanoparticles for targeted stroke therapy through modulation of inflammatory and metabolic signaling. Sci Rep. 2019;9(1):6044. doi:10.1038/s41598-019-42633-9
- Hua S, de Matos MBC, Metselaar JM, et al. Current trends and challenges in the clinical translation of nanoparticulate nanomedicines: pathways for translational development and commercialization. Front Pharmacol. 2018;9:790. doi:10.3389/fphar.2018.00790
- Wu D, Chen Q, Chen X, et al. The blood-brain barrier: structure, regulation, and drug delivery. Signal Transduct Target Ther. 2023;8(1):217. doi:10.1038/s41392-023-01481-w
- Pinheiro RGR, Coutinho AJ, Pinheiro M, et al. Nanoparticles for targeted brain drug delivery: what do we know? Int J Mol Sci. 2021;22(21):11654. doi:10.3390/ijms222111654
- Hajal C, Offeddu GS, Shin Y, et al. Engineered human blood-brain barrier microfluidic model for vascular permeability analyses. Nat Protoc. 2022;17(1):95–128. doi:10.1038/s41596-021-00635-w
- Fang RH, Gao W, Zhang L. Targeting drugs to tumours using cell membrane-coated nanoparticles. Nat Rev Clin Oncol. 2023;20(1):33–48. doi:10.1038/s41571-022-00699-x
- Est-Witte SE, Livingston NK, Omotoso MO, et al. Nanoparticles for generating antigen-specific T cells for immunotherapy. Semin Immunol. 2021;56:101541. doi:10.1016/j.smim.2021.101541
- Sohn HS, Choi JW, Jhun J, et al. Tolerogenic nanoparticles induce type II collagen-specific regulatory T cells and ameliorate osteoarthritis. Sci Adv. 2022;8(47):eabo5284. doi:10.1126/sciadv.abo5284
- Patel SK, Billingsley MM, Frazee C, et al. Hydroxycholesterol substitution in ionizable lipid nanoparticles for mRNA delivery to T cells. J Control Release. 2022;347:521–532. doi:10.1016/j.jconrel.2022.05.020
- Bagchi S, Yuan R, Engleman EG. Immune checkpoint inhibitors for the treatment of cancer: clinical impact and mechanisms of response and resistance. Annu Rev Pathol. 2021;16:223–249. doi:10.1146/annurev-pathol-042020-042741
- Billingsley MM, Singh N, Ravikumar P, et al. Ionizable lipid nanoparticle-mediated mRNA delivery for human CAR T cell engineering. Nano Lett. 2020;20(3):1578–1589. doi:10.1021/acs.nanolett.9b04246
- Ying N, Lin X, Xie M, et al. Effect of surface ligand modification on the properties of anti-tumor nanocarrier. Colloids Surf B Biointerfaces. 2022;220:112944. doi:10.1016/j.colsurfb.2022.112944
- Sanità G, Carrese B, Lamberti A. Nanoparticle surface functionalization: how to improve biocompatibility and cellular internalization. Front Mol Biosci. 2020;7:587012. doi:10.3389/fmolb.2020.587012
- Kosmides AK, Sidhom J-W, Fraser A, et al. Dual targeting nanoparticle stimulates the immune system to inhibit tumor growth. ACS Nano. 2017;11(6):5417–5429. doi:10.1021/acsnano.6b08152
- Myers JA, Miller JS. Exploring the NK cell platform for cancer immunotherapy. Nat Rev Clin Oncol. 2021;18(2):85–100. doi:10.1038/s41571-020-0426-7
- Zhou F, Wang M, Luo T, et al. Photo-activated chemo-immunotherapy for metastatic cancer using a synergistic graphene nanosystem. Biomaterials. 2021;265:120421. doi:10.1016/j.biomaterials.2020.120421
- Lenders V, Koutsoumpou X, Sargsian A, et al. Biomedical nanomaterials for immunological applications: ongoing research and clinical trials. Nanoscale Adv. 2020;2(11):5046–5089. doi:10.1039/D0NA00478B
- Alshawwa SZ, Kassem AA, Farid RM, et al. Nanocarrier drug delivery systems: characterization, limitations, future perspectives and implementation of artificial intelligence. Pharmaceutics. 2022;14(4):883. doi:10.3390/pharmaceutics14040883
- Wu P, Han J, Gong Y, et al. Nanoparticle-based drug delivery systems targeting tumor microenvironment for cancer immunotherapy resistance: current advances and applications. Pharmaceutics. 2022;14(10):1990. doi:10.3390/pharmaceutics14101990
- Nikitin MP, Zelepukin IV, Shipunova VO, et al. Enhancement of the blood-circulation time and performance of nanomedicines via the forced clearance of erythrocytes. Nat Biomed Eng. 2020;4(7):717–731. doi:10.1038/s41551-020-0581-2
- Azevedo C, Macedo MH, Sarmento B. Strategies for the enhanced intracellular delivery of nanomaterials. Drug Discov Today. 2018;23(5):944–959. doi:10.1016/j.drudis.2017.08.011
- Mena-Giraldo P, Pérez-Buitrago S, Londoño-Berrío M, et al. Photosensitive nanocarriers for specific delivery of cargo into cells. Sci Rep. 2020;10(1):2110. doi:10.1038/s41598-020-58865-z
- Ashley CE, Carnes EC, Phillips GK, et al. The targeted delivery of multicomponent cargos to cancer cells by nanoporous particle-supported lipid bilayers. Nat Mater. 2011;10(5):389–397. doi:10.1038/nmat2992
- Qin YT, Li Y-P, He X-W, et al. Biomaterials promote. Front Immunol. 2023;14:1165576. doi:10.3389/fimmu.2023.1165576
- Saini S, Dagar P, Gupta S, et al. Nano-enabled immunomodulation. Nat Nanotechnol. 2021;16(1):1. doi:10.1038/s41565-020-00842-8
- Zhang B, Sun J, Wang Y, et al. Site-specific PEGylation of interleukin-2 enhances immunosuppression via the sustained activation of regulatory T cells. Nat Biomed Eng. 2021;5(11):1288–1305. doi:10.1038/s41551-021-00797-8
- Bruch GE, Fernandes LF, Bassi BLT, et al. Liposomes for drug delivery in stroke. Brain Res Bull. 2019;152:246–256. doi:10.1016/j.brainresbull.2019.07.015
- Fukuta T, Asai T, Yanagida Y, et al. Combination therapy with liposomal neuroprotectants and tissue plasminogen activator for treatment of ischemic stroke. FASEB J. 2017;31(5):1879–1890. doi:10.1096/fj.201601209R
- Campos-Martorell M, Cano-Sarabia M, Simats A, et al. Charge effect of a liposomal delivery system encapsulating simvastatin to treat experimental ischemic stroke in rats. Int J Nanomed. 2016;11:3035–3048. doi:10.2147/IJN.S107292
- Fukuta T, Ishii T, Asai T, et al. Applications of liposomal drug delivery systems to develop neuroprotective agents for the treatment of ischemic stroke. Biol Pharm Bull. 2019;42(3):319–326. doi:10.1248/bpb.b18-00683
- Lu Y, Li C, Chen Q, et al. Microthrombus-targeting micelles for neurovascular remodeling and enhanced microcirculatory perfusion in acute ischemic stroke. Adv Mater. 2019;31(21):e1808361. doi:10.1002/adma.201808361
- Lu H, Li S, Dai D, et al. Enhanced treatment of cerebral ischemia-Reperfusion injury by intelligent nanocarriers through the regulation of neurovascular units. Acta Biomater. 2022;147:314–326. doi:10.1016/j.actbio.2022.05.021
- Wu H, Peng B, Mohammed FS, et al. Brain targeting, antioxidant polymeric nanoparticles for stroke drug delivery and therapy. Small. 2022;18(22):e2107126. doi:10.1002/smll.202107126
- Bernardo-Castro S, Albino I, Barrera-Sandoval ÁM, et al. Therapeutic nanoparticles for the different phases of ischemic stroke. Life. 2021;11(6). doi:10.3390/life11060482
- Wu H, Gao X, Luo Y, et al. Targeted delivery of chemo-sonodynamic therapy via brain targeting, glutathione-consumable polymeric nanoparticles for effective brain cancer treatment. Adv Sci. 2022;9(28):e2203894. doi:10.1002/advs.202203894
- Chis AA, Dobrea C, Morgovan C, et al. Applications and limitations of dendrimers in biomedicine. Molecules. 2020;25(17):3982. doi:10.3390/molecules25173982
- Hong J, Kang M, Jung M, et al. T-cell-derived nanovesicles for cancer immunotherapy. Adv Mater. 2021;33(33):e2101110. doi:10.1002/adma.202101110
- Kang M, Hong J, Jung M, et al. T-cell-mimicking nanoparticles for cancer immunotherapy. Adv Mater. 2020;32(39):e2003368. doi:10.1002/adma.202003368
- Zha S, Liu H, Li H, et al. Functionalized nanomaterials capable of crossing the blood-brain barrier. ACS Nano. 2024;18(3):1820–1845. doi:10.1021/acsnano.3c10674
- Hoshyar N, Gray S, Han H, et al. The effect of nanoparticle size on in vivo pharmacokinetics and cellular interaction. Nanomedicine. 2016;11(6):673–692. doi:10.2217/nnm.16.5
- Fröhlich E. The role of surface charge in cellular uptake and cytotoxicity of medical nanoparticles. Int J Nanomed. 2012;7:5577–5591. doi:10.2147/IJN.S36111
- Zhang D, Wei L, Zhong M, et al. The morphology and surface charge-dependent cellular uptake efficiency of upconversion nanostructures revealed by single-particle optical microscopy. Chem Sci. 2018;9(23):5260–5269. doi:10.1039/C8SC01828F
- Yetisgin AA, Cetinel S, Zuvin M, et al. Therapeutic nanoparticles and their targeted delivery applications. Molecules. 2020;25(9):2193.
- Weng J, Tong HHY, Chow SF. In vitro release study of the polymeric drug nanoparticles: development and validation of a novel method. Pharmaceutics. 2020;12(8):732. doi:10.3390/pharmaceutics12080732
- Herdiana Y, Wathoni N, Shamsuddin S, et al. Drug release study of the chitosan-based nanoparticles. Heliyon. 2022;8(1):e08674. doi:10.1016/j.heliyon.2021.e08674
- Mitchell MJ, Billingsley MM, Haley RM, et al. Engineering precision nanoparticles for drug delivery. Nat Rev Drug Discov. 2021;20(2):101–124. doi:10.1038/s41573-020-0090-8
- Zhao J, Roberts A, Wang Z, et al. Emerging Role of PD-1 in the central nervous system and brain diseases. Neurosci Bull. 2021;37:1188–1202. doi:10.1007/s12264-021-00683-y
- Chauhan P, Lokensgard JR. Glial cell expression of PD-L1. Int J Mol Sci. 2019;20(7):1677. doi:10.3390/ijms20071677
- Bodhankar S, Chen Y, Vandenbark AA, et al. PD-L1 enhances CNS inflammation and infarct volume following experimental stroke in mice in opposition to PD-1. J Neuroinflammation. 2013;10:111. doi:10.1186/1742-2094-10-111
- Bodhankar S, Chen Y, Lapato A, et al. PD-L1 monoclonal antibody treats ischemic stroke by controlling central nervous system inflammation. Stroke. 2015;46(10):2926–2934. doi:10.1161/STROKEAHA.115.010592
- Wang JJ, Jiang L-Q, He B, et al. The association of CTLA-4 and CD28 gene polymorphisms with idiopathic ischemic stroke in the paediatric population. Int J Immunogenet. 2009;36(2):113–118. doi:10.1111/j.1744-313X.2009.00833.x
- Ma J, Shen L, Bao L, et al. A novel prognosis prediction model, including cytotoxic T lymphocyte-associated antigen-4, ischemia-modified albumin, lipoprotein-associated phospholipase A2, glial fibrillary acidic protein, and homocysteine, for ischemic stroke in the Chinese hypertensive population. J Clin Lab Anal. 2021;35(5):e23756. doi:10.1002/jcla.23756
- Han B, Song Y, Park J, et al. Nanomaterials to improve cancer immunotherapy based on ex vivo engineered T cells and NK cells. J Control Release. 2022;343:379–391. doi:10.1016/j.jconrel.2022.01.049
- Zhu X, Li S. Nanomaterials in tumor immunotherapy: new strategies and challenges. Mol Cancer. 2023;22(1):94. doi:10.1186/s12943-023-01797-9
- Mohamed M, Abu Lila AS, Shimizu T, et al. PEGylated liposomes: immunological responses. Sci Technol Adv Mater. 2019;20(1):710–724. doi:10.1080/14686996.2019.1627174
- Jang SF, Liu WH, Song WS, et al. Nanomedicine-based neuroprotective strategies in patient specific-iPSC and personalized medicine. Int J Mol Sci. 2014;15(3):3904–3925.
- Khalil NM, Mainardes RM. Colloidal polymeric nanoparticles and brain drug delivery. Curr Drug Deliv. 2009;6(3):261–273. doi:10.2174/156720109788680912
- Knauer N, Pashkina E, Aktanova A, et al. Effects of cationic dendrimers and their complexes with microRNAs on immunocompetent cells. Pharmaceutics. 2022;15(1):148. doi:10.3390/pharmaceutics15010148
- Apartsin EK. Dendrimers for drug delivery: where do we stand in 2023? Pharmaceutics. 2023;15(12):2740. doi:10.3390/pharmaceutics15122740
- Reisch A, Klymchenko AS. Fluorescent polymer nanoparticles based on dyes: seeking brighter tools for bioimaging. Small. 2016;12(15):1968–1992. doi:10.1002/smll.201503396
- Tang X, Zhu Y, Guan W, et al. Advances in nanosensors for cardiovascular disease detection. Life Sci. 2022;305:120733. doi:10.1016/j.lfs.2022.120733
- Asl SK, Rahimzadegan M. The recent progress in the early diagnosis of acute myocardial infarction based on myoglobin biomarker: nano-aptasensors approaches. J Pharm Biomed Anal. 2022;211:114624. doi:10.1016/j.jpba.2022.114624
- Allison SJ. Nanosensors enable early detection of acute T cell-mediated rejection of transplants. Nat Rev Nephrol. 2019;15(5):253. doi:10.1038/s41581-019-0134-7
- Ma B, Liu X, Zhang Z, et al. A digital nanoplasmonic microarray immunosensor for multiplexed cytokine monitoring during CAR T-cell therapy from a leukemia tumor microenvironment model. Biosens Bioelectron. 2023;230:115247. doi:10.1016/j.bios.2023.115247
- Allen GM, Frankel NW, Reddy NR, et al. Synthetic cytokine circuits that drive T cells into immune-excluded tumors. Science. 2022;378(6625):eaba1624. doi:10.1126/science.aba1624
- Woźniak M, Płoska A, Siekierzycka A, et al. Molecular imaging and nanotechnology-emerging tools in diagnostics and therapy. Int J Mol Sci. 2022;23(5):2658. doi:10.3390/ijms23052658
- Li C, Han C, Duan S, et al. Visualizing T-cell responses: the T-Cell PET imaging toolbox. J Nucl Med. 2022;63(2):183–188. doi:10.2967/jnumed.121.261976
- Bhatnagar P, Alauddin M, Bankson JA, et al. Tumor lysing genetically engineered T cells loaded with multi-modal imaging agents. Sci Rep. 2014;4:4502. doi:10.1038/srep04502
- Ezike TC, Okpala US, Onoja UL, et al. Advances in drug delivery systems, challenges and future directions. Heliyon. 2023;9(6):e17488. doi:10.1016/j.heliyon.2023.e17488
- Aljabali AA, Obeid MA, Bashatwah RM, et al. Nanomaterials and their impact on the immune system. Int J Mol Sci. 2023;24(3):2008. doi:10.3390/ijms24032008
- Wang Y, Yin Q, Yang D, et al. LCP1 knockdown in monocyte-derived macrophages: mitigating ischemic brain injury and shaping immune cell signaling and metabolism. Theranostics. 2024;14(1):159–175. doi:10.7150/thno.88678
- Xie J, Shen Z, Anraku Y, et al. Nanomaterial-based blood-brain-barrier (BBB) crossing strategies. Biomaterials. 2019;224:119491. doi:10.1016/j.biomaterials.2019.119491
- Pawar B, Vasdev N, Gupta T, et al. Current update on transcellular brain drug delivery. Pharmaceutics. 2022;14(12):2719. doi:10.3390/pharmaceutics14122719
- Fisher DG, Price RJ. Recent advances in the use of focused ultrasound for magnetic resonance image-guided therapeutic nanoparticle delivery to the central nervous system. Front Pharmacol. 2019;10:1348. doi:10.3389/fphar.2019.01348