
Abstract
A 62-year-old Caucasian male was referred to retina for choroiditis and uveitis. Multiple areas of yellow irregularities were noted on fundus exam throughout the periphery of both eyes, corresponding to lesions at the sclerochoroidal junction on OCT. A diagnosis of sclerochoroidal calcifications (SCC) was confirmed by B-ultrasonography, fundus photography, OCT imaging, and fluorescein and indocyanine green angiography. Systemic metabolic studies were performed, which showed reduced renal function with increased serum calcium; however, SCC lesions in this case were most likely idiopathic. In this work, we report the clinical findings, appearance on multimodal imaging, and systemic associations of sclerochoroidal calcification. Sclerochoroidal calcifications are an unusual clinical finding that tends to be idiopathic, but a focused workup and specialist referral may be warranted to exclude systemic conditions associated with abnormal calcium-phosphate metabolism or hypokalemic metabolic alkalosis syndromes.
Introduction
Sclerochoroidal calcification (SCC) is an uncommon, benign ophthalmic finding occurring in predominantly elderly, Caucasian patients of either gender.Citation1 Histologically, calcium pyrophosphate is deposited within the sclera, choroid, or both. The peripheral retina has been defined by Duke-Elder and Rutnin, respectively, as either outside the macula or anterior to the vortex veins entrances.Citation2 In this work, the former definition will be used. SCC is characterized by yellow-white sub-retinal lesions, classically located in the superotemporal or superonasal quadrants and mid-peripheral region of the fundus, often between the equator and retinal arcades or alongside the arcades.Citation1,Citation3 Despite well-known features, this condition is often misdiagnosed as a choroidal metastasis, nevus, melanoma, osteoma, or lymphoma and has resulted in unnecessary intervention.Citation4 In the setting of concomitant cancer, differentiating the presence of incidental SCC from metastasis is especially important.Citation5 SCC is most commonly idiopathic, around 79% of cases,Citation6 but it may be associated with recurrent episodes of inflammation or disorders of calcium metabolism or the renal tubulopathies, Bartter and Gitelman syndromes.Citation4
Case Report
A 62-year-old Caucasian male with a history of hypertension, hypercholesterolemia, type 2 diabetes without ocular complications, and arthritis was referred to retina for choroiditis and uveitis. The patient had no ocular complaints besides an occasional “eye itch.” Systemic medications included metformin, allopurinol, losartan, atorvastatin, and Vitamin D. Social and family history were noncontributory. At presentation, corrected visual acuity by Snellen chart was 20/60-2 right eye and 20/60 left eye. On exam, bilateral mild nuclear sclerotic and trace cortical cataracts were noted with rare flare in the anterior chamber. Trace cells and 1+ flare was noted in the left eye at a 3-week follow-up. Fundus examination revealed yellow-white lesions predominantly in the superotemporal near-peripheral and mid-peripheral regions of the fundus bilaterally. The exam was otherwise normal. Fundus photos, fluorescein angiography (FA), Indocyanine green angiography (ICGA), macula OCT, and B-scan ultrasonography were obtained. Fundus photography demonstrated extensive bilateral lesions ( and ). B-scan ultrasonography revealed multiple hyperechoic lesions at the sclerochoroidal junction ( and ). Fundus autofluorescence showed hyperautofluorescence of the lesions (). Late-phase FA revealed peripheral staining without obvious leakage, and ICGA revealed multifocal, scattered hypocyanescent lesions in the peripheral retina of both eyes in all phases with some hypervascularity of the macular area (). The FA also appear to demonstrate hypofluorescent lesions corresponding to areas of choroidal compression. Macular OCT showed scleral thickening with a “rocky-rolling” contour and compression of overlying choroid at and surrounding lesions (). Calcium metabolism and renal function labs were obtained, revealing reduced renal function with increased serum calcium (). The diagnosis of sclerochoroidal calcification was made and additional hematologic, infectious, and autoimmune (HLA-A29) testing was negative for causes of uveitis. Upon 6 month follow-up, the examination and OCT imaging results were unchanged.
Table 1 Laboratory Workup
Figure 1 Fundus photography and B-scan ultrasonography of sclerochoroidal calcification lesions. (A) There are dense yellow-white lesions in the superotemporal region near the superior retinal arcades in the right eye. (B) Fundus photography shows scattered calcifications in the superotemporal region of the fundus in the left eye. (C and D) Ultrasonography in both eyes shows hyperechoic lesions at the level of the choroid-scleral junction with posterior shadowing.
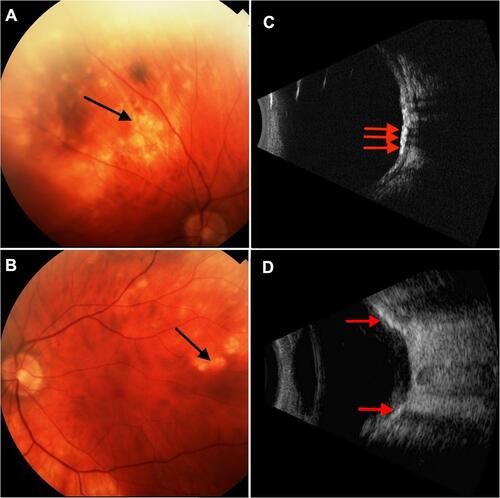
Figure 2 Blue-light autofluorescence of the right eye (left eye not shown) displaying an autofluorescent lesion adjacent to the superior and inferior retinal arcades.
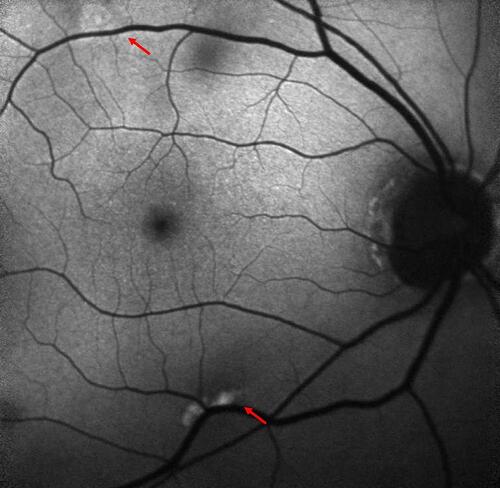
Figure 3 Fluorescein angiography of right (A) and left (B) eyes displays mild-moderate late phase staining with no obvious leakage. Indocyanine green angiography (ICGA) of right (C) and left (D) eyes shows extensive, multifocal hypofluorescent lesions in the near-peripheral and mid-peripheral fundus with choroidal vascular hyperpermeability of the macular area.
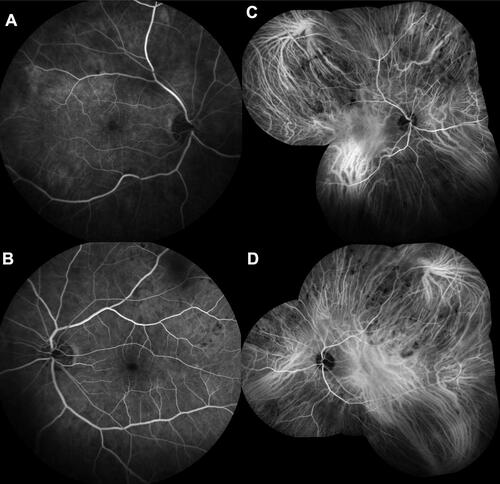
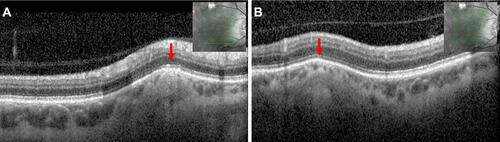
Figure 4 OCT imaging of representative SCC lesions in the right eye (left eye not shown) near the (A) superior and (B) inferior retinal arcades. The sclera appears to have a “rocky-rolling” surface with thinning of overlying choroid.
Discussion
SCC is characterized by calcium deposition within the sclera, eventually invading the choroid and manifesting as a yellow-white choroidal mass. Lesions are bilateral in approximately 52% of cases.Citation1 Patients with SCC are typically Caucasian with a mean age of 69 years-old and have a slight female predominance (60%).Citation1 SCC is most often asymptomatic; however, a relative scotoma in areas of corresponding chorioretinal atrophy overlying SCC lesions may be seen.Citation7 Rarely, visual deterioration is seen in SCC due to the development of choroidal neovascularization (CNV) with exudation extending to the macula.Citation8,Citation9 The differential includes choroidal metastasis, melanoma, nevus, osteoma, chorioretinitis, and intraocular lymphoma which may be differentiated upon exam, imaging, and angiography.Citation4 SCC findings on multimodal imaging are summarized in .
Table 2 Sclerochoroidal Calcification Findings on Multimodal Imaging
Diagnosis of SCC can be made with fundoscopic examination. Ancillary testing may confirm the diagnosis.Citation4 However, extensive testing and imaging for incidental findings of SCC is unnecessary. Hasanreisoglu et alCitation6 have classified these calcium deposits based on enhanced depth imaging optical coherence tomography (EDI-OCT) appearance. They described four types of lesions (flat, rolling, rocky-rolling, or table mountain) based on scleral contour, and the “rocky-rolling” appearance may be unique to SCC, helping differentiate it from more concerning lesions. However, the exact utility of classifying these lesions in this way requires further research. On OCT imaging, the choroid is thin above these lesions, and there may be thinning of the retina with an absence of the external limiting membrane and disruption of the ellipsoid zone.Citation3 The RPE may be thin, normal, or thickened above the lesion.Citation3,Citation6 “Rocky-rolling” type lesions have a significantly higher rate of RPE and ellipsoid zone abnormalities compared to the other types.Citation6 B-Scan ultrasonography will demonstrate a dense echogenic mass with posterior shadowing.Citation6 If the calcium deposits are located within the outer sclera, ultrasonography may uncover hyperechoic plaques in eyes with mild RPE alterations or an otherwise normal appearance.Citation4
On FAF, lesions may be hyperautofluorescent, but hypoautofluorescent lesions with a hyperautofluorescent halo have also been observed.Citation3,Citation10,Citation11 Fung et alCitation3 hypothesized the hyperautofluorescence was due to thinning of the choroid, revealing hyperautofluorescent sclera or calcific tissue. Another explanation has been proposed by Caminal-Mitjana et alCitation10 based on correlating FAF and spectral domain-OCT findings. The authors assert that choriocapillaris compression by scleral lesions leads to RPE dysfunction and accumulation of lipofuscin, a fluorophore, within the RPE. As RPE-choriocapillaris outpouching develops on SD-OCT, there is diminished autofluorescence likely corresponding to RPE atrophy and lipofuscin loss. Where the RPE is healthy, the FAF is isoautofluorescent. FA findings over lesions may demonstrate hypofluorescence in the arterial phase followed by progressively intensifying hyperfluorescence, possibly due to increased scleral staining around the lesions.Citation10 In areas of RPE atrophy, the transmission of choroidal vasculature through window defects may be seen. FA may also reveal CNV, a rare association with SCC.Citation4
ICGA findings vary and are somewhat lacking in the literature. It may show hypocyanescence in all phasesCitation12 or hypocyanescence during early phases with mild and progressive hypercyanescence in later phases.Citation5 Mitamura et alCitation11 described a case of bilateral SCC in the setting of secondary hyperparathyroidism with ICGA findings similar to our patient’s. Their patient displayed choroidal vascular hyperpermeability in the macular area with scattered hypocyanescent lesions in the peripheral fundus on ICGA with dilated Haller layer veins on OCT. They hypothesize this was due to multiple points of choroidal circulation impairment due to scleral lesions causing compression and subsequent vascular congestion. However, their patient had dialysis-dependent chronic kidney disease, which also causes systemic vascular dysfunction. Lastly, orbital computer tomography will show a radiodense scleral lesion, confirming the presence of calcification.Citation3
The pathogenesis of SCC may be either dystrophic, idiopathic, or metastatic.Citation4,Citation12 Dystrophic calcification occurs after chronic tissue damage or necrosis, such as senile degeneration, chronic inflammation, or severe trauma in the setting of normal calcium-phosphorus metabolism.Citation4 Idiopathic cases of SCC typically seen in elderly patients may be related to the dystrophic changes caused by chronic movement of the oblique muscles, which has its insertion near a common location for SCC, the temporal arcades. Evidencing this hypothesis is that the calcified plaques near insertion sites of horizontal recti muscles are histologically identical to SCC.Citation4 Metastatic calcification develops in normal tissue due to an abnormal calcium-phosphorus metabolism seen in hyperparathyroidism, pseudohypoparathyroidism, sarcoidosis, hypervitaminosis D, and chronic renal failure.
Disorders of abnormal calcium-phosphorus metabolism are commonly found in patients with SCC (). A review of 179 eyes from 118 patients by Shields et alCitation1 found 27% of patients had hyperparathyroidism, and 15% had a parathyroid adenoma. SCC is also seen in secondary hyperparathyroidism due to chronic renal failure, wherein phosphate retention and decreased vitamin D activation lead to hypocalcemia and elevated parathyroid compensation.Citation1 Increased serum calcium, phosphate, and calcium-phosphate products inducing soft tissue calcification, and SCC has been observed in hypervitaminosis D-related disorders such as sarcoidosis producing 1,25-dihydroxy-cholecalciferol and vitamin D intoxication from ingesting large doses of vitamin D.Citation12,Citation13 Two cases of SCC associated with hypovitaminosis D have also been reported. Sierra-Rodriguez et alCitation14 and Ale & DavidCitation15 describe a case of SCC associated with isolated vitamin D deficiency of 4 ng/mL and 8.9 ng/mL, respectively. As with hypervitaminosis D, the exact mechanism of calcification development is unclear, but hypovitaminosis D may lead to calcification by disinhibiting PTH secretion or causing dysfunction of inflammatory pathways.Citation13
Table 3 Diseases Associated with Sclerochoroidal Calcification
Pseudohypoparathyroidism (PHP) includes several related disorders involving resistance to parathyroid hormone and subsequent hypocalcemia and hyperphosphatemia. Extensive SCC has been reported in several cases of type 1a PHP, known as Albright hereditary osteodystrophy. This disease is due to the inactivation of the GNAS1 gene, and it presents with characteristic facies, brachydactyly, renal dysfunction, electrolyte abnormalities, subcutaneous calcifications, and developmental delay.Citation16,Citation17
In 118 patients with SCC, Shields et alCitation1 found primary Bartter syndrome was present in 2% and Gitelman syndrome secondary to diuretic use in 11%. SCC in primary Gitelman syndrome has also been described.Citation18 It is important to determine the presence of these diseases because electrolyte abnormalities, and potential cardiac arrhythmias, can be fatal without appropriate management.Citation19 Although Bartter and Gitelman syndromes have different etiologies, the clinical presentation—normotensive hypokalemic metabolic alkalosis—is often similar.
There are five variants of Bartter syndrome with defects of different channels located in the thick ascending limb of the nephron. Most variants present antenatally with polyhydramnios and postnatally with characteristic facies, salt wasting, polyuria, polydipsia, marked hypokalemia, metabolic alkalosis, hypercalciuria, and failure to thrive.Citation19 Classic Bartter’s syndrome, type III, may display some or all of these features, but it is historically considered a milder variant and may present in adulthood with or without developmental delay.Citation20 With its milder features, classic Bartter syndrome is often confused with Gitelman syndrome. The presence of normal or high urine calcium found in Bartter syndrome will differentiate it from Gitelman syndrome, where urine calcium is always low. Gitelman syndrome is caused by an autosomal recessively inherited mutation of the thiazide-sensitive sodium chloride cotransporter in the distal convoluted tubule. It usually presents after the age of 6 years old with metabolic alkalosis, hypomagnesemia, hypokalemia, hypocalciuria, and chondrocalcinosis. Hypomagnesemia may be present in Bartter syndrome but is more characteristic of Gitelman syndrome.Citation20
Bartter and Gitelman syndromes and other causes of hypomagnesemia have been associated with calcium pyrophosphate dihydrate deposition disease (CPPD), also called pseudogout.Citation21 CPPD, particularly familial disease,Citation22 has been associated with SCC as well.Citation23 Although the mechanisms behind these associations are unclear, hypomagnesemia has been implicated in the development of CPPD and may also contribute to SCC development via the formation of calcium pyrophosphate dihydrate crystal.Citation20,Citation21 Magnesium inhibits crystal formation by several mechanisms; it increases crystal solubility, decreases inorganic pyrophosphate production, and acts as a cofactor of alkaline phosphatase, which hydrolyzes inorganic pyrophosphate.Citation12,Citation21
After finding incidental SCC, further laboratory screening for calcium-phosphate metabolism dysfunction and renal tubulopathies is warranted with a prompt nephrology referral if concerning abnormalities are detected. A list of possible testing includes renal function tests; serum levels of parathyroid hormone, calcitonin, vitamin D, and alkaline phosphatase; and blood and urine levels of calcium, potassium, phosphate, and magnesium.Citation1,Citation9 In our case, workup revealed mild hypercalcemia and mildly impaired renal function. Our patient was also taking vitamin D. However, our patient’s overall clinical gestalt suggests idiopathic SCC.
Treatment for SCC is conservative with the management of any underlying disease. SCC lesions have been shown in some cases to slowly enlarge over the span of years with, as of yet, unknown consequences.Citation22,Citation24 Given the rare yet possible development of CNV, some authors recommend regular visits every couple of years with imaging.Citation24 In cases of CNV requiring treatment, anti-VEGF intravitreal injections, argon laser photocoagulation, and photodynamic therapy have shown success.Citation9 Clinical prognosis will vary depending on systemic associations, but visual prognosis, especially in idiopathic cases, is generally good as parafoveal or foveal involvement or CNV development is rare.Citation4
Conclusion
Although SCC association with underlying systemic conditions is rare, excluding systemic disease with a detailed examination, laboratory workup, and ancillary multimodal imaging may be warranted. Imaging such as OCT (preferably EDI-OCT), FA, ICGA, or B-scan ultrasonography and laboratory testing such as parathyroid, renal function, calcium, and vitamin D testing along with assessing diuretic use, may elucidate this rare, incidental finding and rule out concerning disease or prevent unnecessary intervention.
Informed Consent/Institutional Approval
Informed consent to publish their case details and images was obtained from the patient. This case report did not require institutional approval for publication.
Acknowledgments
We would like to thank Olivia Crowley for her contribution.
Disclosure
All authors report no conflicts of interest in this work.
References
- Shields CL, Hasanreisoglu M, Saktanasate J, Shields PW, Seibel I, Shields JA. Sclerochoroidal calcification: clinical features, outcomes, and relationship with hypercalcemia and parathyroid adenoma in 179 eyes. Retina. 2015;35(3):547–554. doi:10.1097/IAE.0000000000000450
- Quinn N, Csincsik L, Flynn E, et al. The clinical relevance of visualising the peripheral retina. Prog Retin Eye Res. 2019;68(June 2018):83–109. doi:10.1016/j.preteyeres.2018.10.001
- Fung AT, Arias JD, Shields CL, Shields JA. Sclerochoroidal calcification is primarily a scleral condition based on enhanced depth imaging optical coherence tomography. JAMA Ophthalmol. 2013;131(7):960–963. doi:10.1001/jamaophthalmol.2013.67
- Shields JA, Shields CL. CME review: sclerochoroidal calcification. The 2001 Harold Gifford lecture. Retina. 2002;22(3):251–261. doi:10.1097/00006982-200206000-00001
- Lassandro NV, Danieli L, Nicolai M, Pirani V, Pelliccioni P, Mariotti C. Sclerochoroidal calcification as an incidental finding during oncological staging of a patient with parotid malignancy: a case report. Eur J Ophthalmol. 2021;112067212199962. doi:10.1177/1120672121999629
- Hasanreisoglu M, Saktanasate J, Shields PW, Shields CL. Classification of sclerochoroidal calcification based on enhanced depth imaging optical coherence tomography mountain-like features. Retina. 2015;35(7):1407–1414. doi:10.1097/IAE.0000000000000468
- Hara K, Tanito M, Kodama T, Ohira A. A case of chorioretinal atrophy due to sclerochoroidal calcification. Acta Ophthalmol. 2013;91(2):e167–e168. doi:10.1111/j.1755-3768.2012.02470.x
- Bessette AP, Singh AD. Multimodal imaging of choroidal neovascularization associated with sclerochoroidal calcification. Ocul Oncol Pathol. 2016;2(4):234–238. doi:10.1159/000446214
- Goerlitz-Jessen M, Ali MH, Grewal DS. Rare Complication of Sclerochoroidal Calcifications. JAMA Ophthalmol. 2019;137(1):111–112. doi:10.1001/jamaophthalmol.2018.2457
- Caminal-Mitjana JM, Padrón-Pérez N, Arias-Barquet L, Rubio-Caso MJ, Catala-Mora J. Correlation between spectral-domain optical coherence tomography and autofluorescence findings in sclerochoroidal calcification. Can J Ophthalmol. 2013;48(4):331–334. doi:10.1016/j.jcjo.2013.01.024
- Mitamura M, Kase S, Ishida S. Multimodal imaging in sclerochoroidal calcification: a case report and literature review. BMC Ophthalmol. 2020;20(1). doi:10.1186/s12886-020-01520-y
- Honavar SG, Shields CL, Demirci H, Shields JA. Sclerochoroidal calcification: clinical manifestations and systemic associations. Arch Ophthalmol. 2001;119(6):833–840. doi:10.1001/archopht.119.6.833
- Wang J, Zhou JJ, Robertson GR, Lee VW. Vitamin D in vascular calcification: a double-edged sword? Nutrients. 2018;10(5):652. doi:10.3390/nu10050652
- Sierra-Rodríguez MA, Bailez Fidalgo C, Sáenz-Francés F, Gonzalez Romero JC, Muñoz Bellido L. Calcificaciones esclerocoroideas asociadas a hipovitaminosis D. Arch Soc Esp Oftalmol. 2014;89(7):290–292. doi:10.1016/j.oftal.2012.12.016
- Ali ZC, David VP. Sclerochoroidal calcification associated with hypovitaminosis D. Can J Ophthalmol. 2017;52(4):e121–e122. doi:10.1016/j.jcjo.2017.02.001
- Lee H, Kumar P, Deane J. Sclerochoroidal calcification associated with Albright’s hereditary osteodystrophy. BMJ Case Rep. 2012;2012:bcr0320126022–bcr0320126022. doi:10.1136/bcr-03-2012-6022
- Wong S, Zakov ZN, Albert DM. Scleral and choroidal calcifications in a patient with pseudohypoparathyroidism. Br J Ophthalmol. 1979;63(3):177–180. doi:10.1136/bjo.63.3.177
- Gupta R, Hu V, Reynolds T, Harrison R. Sclerochoroidal calcification associated with Gitelman syndrome and calcium pyrophosphate dihydrate deposition. J Clin Pathol. 2005;58(12):1334–1335. doi:10.1136/jcp.2005.027300
- Fulchiero R, Seo-Mayer P. Bartter Syndrome and Gitelman Syndrome. Pediatr Clin North Am. 2019;66(1):121–134. doi:10.1016/j.pcl.2018.08.010
- Rodríguez-Soriano J. Bartter and related syndromes: the puzzle is almost solved. Pediatr Nephrol. 1998;12(4):315–327. doi:10.1007/s004670050461
- Joshi A, Chokkalingam S. Magnesium disorders can cause calcium pyrophosphate deposition disease: a case report and literature review. Eur J Rheumatol. 2018;5(1):53–57. doi:10.5152/eurjrheum.2017.16116
- Boutboul S, Bourcier T, Heligon JP, et al. Familial pseudotumoral sclerochoroidal calcification associated with chondrocalcinosis. Br J Ophthalmol. 2004;88(8):1094–1095. doi:10.1136/bjo.2003.039925
- Ciaffi J, Borlandelli E, Mancarella L, Brusi V, Meliconi R, Ursini F. Sclerochoroidal calcifications associated with early-onset calcium pyrophosphate deposition disease. Clin Rheumatol. 2020;39(9):2825–2826. doi:10.1007/s10067-020-05148-7
- Slean GR, Kalevar A, Chen J, Johnson R. Enlargement of sclerochoroidal calcifications: multimodal imaging update. Retin Cases Brief Rep. 2018;12(1):S122–S124. doi:10.1097/ICB.0000000000000644