
Abstract
Objective
To develop a simple and effective prognostic scoring system to predict the efficacy of drug-eluting bead-transcatheter arterial chemoembolization (DEB-TACE) in the treatment of hepatocellular carcinoma (HCC).
Methods
Data were retrospectively collected from 230 patients with HCC who received DEB-TACE treatment at six medical centers between January 2019 and December 2022. We developed a predictive score based on independent risk factors for overall survival (OS), validated the model using a validation cohort, and compared its prognostic accuracy with commonly used HCC staging systems.
Results
The number of tumors, albumin-bilirubin levels, alpha-fetoprotein levels, and portal vein thrombus grade were identified as independent factors influencing OS. Based on these factors, we established the DEB-TACE treatment of HCC (DTH) scoring system. The DTH score correlated well with OS, which decreased as the DTH score increased. According to the DTH score, patients were categorized into three risk groups: low-risk (DTH-A, 0–4 points), medium-risk (DTH-B, 5–6 points), and high-risk (DTH-A, 7 points). The OS of each risk group was 18.73±0.62 months, 12.73±0.10 months, and 6.93±0.19 months, respectively (p<0.001). The external cohort validation confirmed the accuracy of the DTH score, demonstrating superior predictive performance compared to other commonly used HCC scoring systems.
Conclusion
The DTH-HCC scoring system effectively predicts the outcomes of HCC patients undergoing DEB-TACE as initial treatment. This model can aid in the initial planning and decision-making process for DEB-TACE treatment in HCC patients.
Introduction
Primary hepatocellular carcinoma (PHC) is the sixth most common tumor globally, with over 90% of PHC cases pathologically classified as hepatocellular carcinoma (HCC).Citation1 China is a high-risk country for HCC. Due to the lack of early diagnosis and poor prognosis, HCC has become the leading cause of cancer-related deaths worldwide, with a very high mortality rate. Reports indicate that less than 20% of HCC patients are eligible for surgical resection.Citation2 Therefore, local treatments are particularly important in the management of HCC.
Currently, transcatheter arterial chemoembolization (TACE) is considered a first-line local treatment for patients with non-surgical HCC, due to its advantages of safety, minimal trauma, and good efficacy.Citation3,Citation4 TACE controls tumor growth by injecting chemotherapy drugs and embolic agents into the artery supplying the HCC, further blocking the tumor blood supply, causing ischemia and hypoxia at the tumor site, and ultimately achieving tumor ablation.Citation5 Conventional TACE (cTACE) uses iodinated oil as a carrier for chemotherapy drugs, embolizing the liver tumor blood vessels through the hepatic artery and releasing chemotherapy drugs to kill tumor cells. However, the strong diffusibility of iodinated oil can lead to systemic toxicity and serious complications.Citation6
Drug-eluting bead-TACE (DEB-TACE), a new interventional therapy, uses microspheres as carriers to effectively control the release of chemotherapy drugs, avoiding their diffusion into the systemic circulatory system. This approach maximizes the killing of tumor cells while reducing the toxicity of chemotherapy drugs.Citation7,Citation8 The microcatheter achieves super-selectivity of the blood supply artery, significantly improving the recovery from postoperative liver injury and complications, ensuring good safety and effectiveness.Citation9 However, the benefits of DEB-TACE vary among clinical HCC patients. Repeated treatments of DEB-TACE can damage normal liver cells and aggravate cirrhosis, primarily due to the heterogeneity of patients’ liver function reserve. Therefore, this study aims to develop a prognostic score system based on a combination of liver function parameters and tumor factors to identify suitable candidates for DEB-TACE.
Materials and Methods
Study Participants
We analyzed the clinical data of 233 patients undergoing DEB-TACE treatment at six medical centers in Anhui, China, from January 2019 to December 2022.
Inclusion criteria: ① Confirmed diagnosis of HCC through pathological examination or based on the American Association for the Study of Liver Diseases (AASLD) practice guideline;Citation10 ② Unresectable HCC after Discussion by the multidisciplinary team; ③ First-line treatment of HCC patients with DEB-TACE; ④ Age between 18–75 years old; ⑤ Ecog score ≤ 1; ⑥ Child‒Pugh class A or B; ⑦ No concomitant other malignancies.
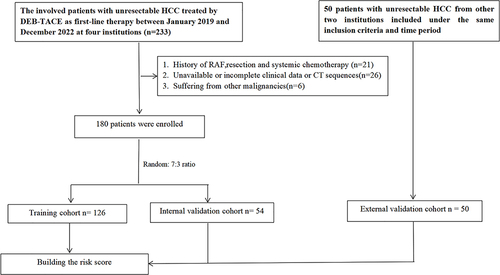
Exclusion criteria: ① obstructive jaundice; ② large amount of ascites; ③ severe hypersplenism with platelets less than 5×109/L; ④ gastrointestinal bleeding in the past 3 months; ⑤ previous liver transplantation, chemotherapy, radiotherapy, systemic treatment, ablation, or other treatments; ⑥ accompanied by severe heart, lung, and renal insufficiency; ⑦ incomplete follow-up data. Finally, 230 patients were included in the final analysis. A total of 150 patients from four institutions with unresectable HCC were randomly assigned to the training and internal validation groups in a ratio of 7:3. Of these, 126 patients were included in the training group, and 54 patients were included in the internal validation group. Additionally, 50 patients diagnosed with unresectable HCC from two other institutions were classified as the external validation groups (). The development of this project complies with the ethical standards of the Helsinki Declaration promulgated in 1975 and was approved by the Ethics Committee of The Second Affiliated Hospital of Anhui Medical University (Approval No. YX2022-094), through the retrospective study design and analysis of clinical data, the ethics committee of the Second Affiliated Hospital of Anhui Medical University formally waived the requirement for informed consent. All patient information is confidential.
Figure 1 Flow diagram of study population.
Treatment and Follow-Up
All DEB-TACE procedures were performed by two interventional radiologists with more than 10 years of TACE experience from each institution. A detailed description of the DEB-TACE procedure is provided in Appendix E. Progression-Free-Survival (PFS) refers to the time from randomization to disease progression. Overall survival (OS) was defined as the time from the date of the first DEB-TACE to the date of death from any cause. Six to eight weeks after DEB-TACE, an enhanced CT scan was performed, and tumor indicators were reviewed. Based on the evaluation of mRECIST criteria (mRECIST criteria as follow: complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). Objective response rate (ORR) refers to the sum of CR and PR, while non-objective response rate (no-ORR) refers to the sum of SD and PD. Disease control rate (DCR) refers to the sum of CR, PR and SD), the patient’s general condition, liver and kidney function, etc., it was determined whether the patient should receive DEB-TACE treatment again. If the patient could not continue to receive DEB-TACE treatment, optimal supportive treatment was recommended, mainly including liver protection, immune enhancement, and nutritional support treatment.
Development of Prognostic Models
The variables selected for the prediction model were derived from univariate and multivariate analyses of patients, tumors, liver function, and treatment-related factors using Cox proportional hazards regression. The model output used to estimate survival probability is expressed as a coefficient for calculating the hazard ratio: S(t)=S0(t)exp(∑Xβ), where X is a vector of independent variables, X=(x1, x2, xk), and β is a vector of regression coefficients for the corresponding variables. S(t) is the probability of survival at time t in the past, and S0 is the baseline survival probability.
Performance Verification
To compared the prognosis performance of the developed scoring system with currently commonly used HCC scoring/staging systems, including BCLC, AJCC, CNLC, CLIP, Okuda, all patients were first scored and staged according to each scoring/staging system. Two methods were used for this comparison: ① Using the Kaplan-Meier method to plot survival curves, and visually observe the ability to differentiate survival curves. ② Using Cox regression analysis to calculate the hazard ratio (HR) of each scoring/staging system, and compare the ability of each scoring system to predict prognosis.
Statistical Analysis
For baseline data, continuous variables are recorded as mean ± standard deviation, and categorical variables are recorded as median and range. Continuous variables are compared using t-tests, and categorical variables are compared using Pearson chi-square tests or Fisher’s exact tests. For survival analysis, the Kaplan-Meier method is used to calculate OS, and the Log rank test is used to test for statistical differences. For univariate analysis, the Log rank test is used to examine the correlation between all variables and OS. Variables with a P-value less than 0.05 are included in the multivariate analysis. The Cox proportional hazards model is used to identify independent risk factors affecting prognosis. Based on the P-value of each independent risk factor, the prognostic score for each factor is calculated (rounded to the nearest integer). The prognosis score for each individual is then obtained by summing the scores of the corresponding risk factors, establishing the DTH score. The survival period for each DTH score is calculated using the Kaplan-Meier method, and patients are divided into low-risk, medium-risk, and high-risk groups based on their DTH scores. The survival periods for each risk group are also calculated using the Kaplan-Meier method, and differences between groups are tested using the Log rank test. Finally, the validation cohort is used to verify the clinical efficacy of the DTH prognostic score. All statistical analyses were performed using SPSS26.0, and all statistical P-values are two-sided, with P<0.05 indicating statistical significance.
Results
Baseline Data of Research Objects
In the training cohort, the average age of patients was 50.6±11.56 years, with 77.78% being male. Hepatitis (76.19%) and cirrhosis (72.22%) were the primary causes. The average tumor size was approximately 7.24cm, and 49.21% of patients had vascular cancer thrombus. There was no significant difference between the internal validation, external validation and the baseline data of the training cohort. The baseline data of patients are detailed in .
Table 1 Baseline Patient Characteristics
Safety and Efficacy Evaluation
The average number of DEB-TACE treatments received by patients in the training cohort was 2.8 (range: 1–4). The efficacy evaluation, based on RECIST criteria using the initial response, included 6 cases of complete response (CR), 52 cases of partial response (PR), 51 cases of stable disease (SD), 17 cases of progressive disease (PD), The average follow-up time was 17.4 months (range: 2.5–37.2 months), with a median survival time of 13.35 months (95% CI: 11.35–15.06). In the internal validation cohort, the average number of DEB-TACE treatments was 2.1 (range: 1–3). The efficacy evaluation included 2 cases of CR, 27 cases of PR, 21 cases of SD, and 4 cases of PD, with an average follow-up time of 16.96 months (range: 1.5–31 months) and a median survival time of 14.9 months (95% CI: 11.26–15.54). In the external validation cohort, the average number of DEB-TACE treatments was 2.6 (range: 1–4). The efficacy evaluation included 3 cases of CR, 25 cases of PR, 16 cases of SD, 6 cases of PD, with an average follow-up time of 18.1 months (range: 2.2–30.3 months) and a median survival time of 15.3 months (95% CI: 8.6–20.9). There were no treatment-related deaths in this study. The efficacy evaluation of the three cohorts is detailed in .
Table 2 Tumor Response Rate Between the Training Cohort and Validation Cohorts
Prognostic Factors
Univariate analysis Results showed that tumor diameter, ALBI score, PVTT, AFP, tumor number, and PVTT might affect the patient’s survival. Multivariate analysis identified the following independent risk factors influencing the survival of patients with HCC: ALBI grade (1 vs 2, 0.605 (0.438–0.835), P=0.002); PVTT (No vs I–II, 0.556 (0.401–0.772), P<0.001), AFP (<400ng/mL vs ≥400ng/mL, 0.432 (0.451–0.709), P<0.012, Tumor number (<3 vs ≥3, 0.503 (0.353–0.716), P<0.001. These findings are summarized in .
Table 3 Multivariable Cox Regression Analysis of Predictors of OS
Establishment and Validation of the Scoring System
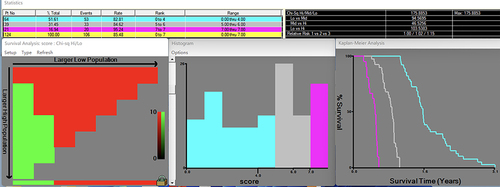
According to the multivariate Cox proportional hazards model, the number of tumors, ALBI grade, AFP, and portal vein thrombus grade are independent risk factors that affect prognosis. Utilizing the β Partial regression coefficient × 2, we obtained the prognostic score (rounded to the nearest integer) for each factor. Each patient was assigned a score based on the presence or absence of these four risk factors. This scoring system is named the DEB-TACE treatment of HCC Score (DTH score). The DTH score is the sum of the scores for the four factors, with a score range of 0 to 7 (see ). Based on the relationship between patient survival time and DTH score, it can be observed that as the DTH score increases, the patient’s OS gradually decreases. Using the X-tile software to set the cutoff value, the patient’s DTH score is divided into low-risk (DTH-A, 0–4 points), medium-risk (DTH-B, 5–6 points) and high-risk groups (DTH-C, 7 points) ().
Table 4 DEB-TACE Treatment of HCC Score System (DTH Score)
Figure 2 X-tile plots of the DTH score in the training cohort. Coloration of the plot represents the strength of the association at each division, ranging from low (dark, black) to high (bright, red, or green). Red represents inverse association between DTH scores and overall survival. The x-axis represents all potential cutoff points, from low to high (left to right), that define a low subset, whereas the y-axis represents cutoff points from high to low (top to bottom) that define a high subset. The results show that there are 64 patients with low-risk, 39 patients with medium-risk and 21 patients with high-risk.
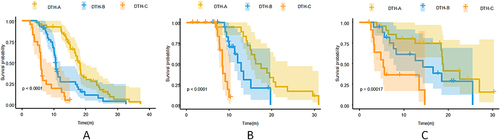
To verify the accuracy of the DTH scoring system, we applied it to the training, internal, and external validation data. According to the classification of the scoring system, it can be seen that the median PFS (13.51 months, 6.54 months, and 2.15 months, P<0.001) and OS (18.73 months, 13.73 months, and 6.93 months, P<0.001) of each risk group (DTH-A, DTH-B, DTH-C) in the training cohort were statistical differences ( and ), respectively. The median PFS (12.72 months, 8.53 months, and 4.19 months, P<0.001) and OS (18.67 months, 13.31 months, and 8.62 months, P<0.001) of each risk group (DTH-A, DTH-B, DTH-C) in the internal validation cohort were statistical differences ( and ), respectively The median PFS (14.51 months, 10.02 months, and 1.67 months, P<0.001) and OS (19.35 months, 14.82 months, and 7.66 months, P<0.001) of each risk group (DTH-A, DTH-B, DTH-C) in the external validation cohort were statistical differences ( and ), respectively. The DTH scoring system demonstrated good predictive performance across all patients cohorts. To further clarify the correlation of tumor response and PFS, OS and DTH score, this study integrated the three groups together and then observed ORR and DCR in different scores and found differences in ORR and DCR in different DTH scores of patients, either PFS or OS, see .
Table 5 Correlation of Tumor Response and PFS, OS, and DTH Scores
Figure 3 Kaplan-Meier survival curves according to DTH score. PFS according to DTH scores in the training cohort (A), internal validation cohort (B), External validation cohort (C).
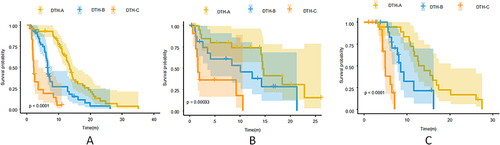
Figure 4 Kaplan-Meier survival curves according to DTH score. Overall survival according to DTH scores in the training cohort (A), internal validation cohort (B), External validation cohort (C).
Model Performance and Discrimination Ability
Comparison of Overall Survival
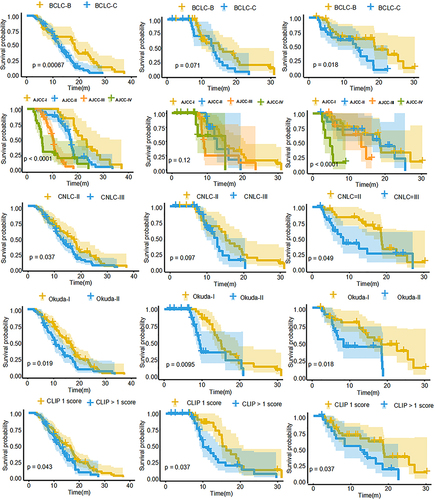
All patients in the training and validation cohorts were scored/staged according to commonly used tumor staging/scoring systems (BCLC, AJCC, CNLC, Okuda, CLIP). The median survival time of patients in each stage was calculated using the Kaplan-Meier method. In the training cohort, although there are statistical differences in survival time between different stages in each staging system (all P < 0.05), there is some overlap in survival time among the BCLC, CNLC, AJCC, and CLIP systems, resulting in poor discrimination. Similarly, this pattern is observed in the internal and external validation cohorts (see ).
Figure 5 Kaplan-Meier survival curves of training cohort (left), internal validation cohort (middle) and external validation cohort (right) categorized by the different scoring/staging systems.
Comparison of Model Performance and Risk Coefficient
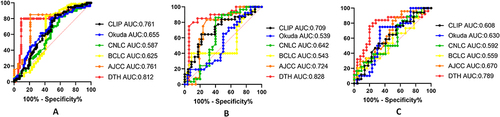
To evaluate the performance of the DTH model, we compared it with several previous staging systems for predicting the efficacy of DEB-TACE in the treatment of advanced HCC using time-dependent receiver operating characteristic curve analysis. It was found that in three study cohorts, the DTH model had a ROC area of 0.812, 0.828, and 0.789 in predicting the survival time of advanced HCC treated with DEB-TACE. The ROC areas in the training group, internal validation group, and external validation group were all higher than those of other staging systems, demonstrating good predictive performance (see ).
Figure 6 Time-dependent ROC curves to estimate OS. AUCs were calculated to assess the prognostic accuracy within the DTH model and other staging systems in training cohort (A), internal validation cohort (B) and external validation cohort (C).
Using multivariate Cox regression analysis (see ), we explored the correlation between various staging systems and OS. In the training cohort, the Cox analysis results suggest that DTH is significantly correlated with OS (P<0.001), while BCLC, CNLC, Okuda, AJCC, and CLIP have no clear correlation with OS. The HR’s of DTH-A, DTH-B, and DTH-C were 1.66, 3.75, and 6.02, respectively, which were significantly higher than other scoring/staging systems, indicating good predictive ability for mortality risk. Similarly, in the internal validation cohort, Cox regression analysis revealed significant associations between DTH, BCLC, CNLC, and OS, while no clear association was observed between AJCCC, Okuda, CLIP, and OS. The HR’s of DTH-B and DTH-C were 3.22 and 4.95, respectively, which were significantly higher than those of BCLC and CNLC, indicating good predictive ability for mortality risk. In the external validation cohort, Cox regression analysis revealed significant associations between DTH, CNLC, and OS, while no clear association was observed between BCLC, AJCCC, Okuda, CLIP, and OS. The HR’s of DTH-A, DTH-B, and HAP-C were 1.78, 3.22, and 4.95, respectively, which were higher than those of the CNLC staging system, also indicating good predictive ability for mortality risk.
Table 6 Comparison of Each of the Different Scoring/Staging Systems
Discussion
In this study, we explored the efficacy and safety of DEB-TACE in the treatment of unresectable HCC. The results demonstrated that the median survival time of the training cohort was 13.68 months, with 6-month, 12-month, and 24-month survival rates were 68%, 52%, and 33%, respectively. Overall, these results were comparable to those reported in other literature on the treatment of unresectable HCC with DEB-TACE.Citation11,Citation12 However, they were significantly better than previously reported survival of c-TACE in the treatment of advanced HCC.Citation13,Citation14 The primary objective of this study was to identify factors that affect the prognosis of DEB-TACE in the treatment of unresectable HCC and to establish a simple, practical, and reliable prognostic scoring system to predict the efficacy and survival benefit of DEB-TACE in HCC patients. Analysis of the data from 136 cases of unresectable HCC undergoing DEB-TACE treatment in the training cohort revealed that the number of tumors, ALBI grade, AFP, and portal vein thrombus grade were independent factors affecting patient survival, as determined through a multivariate Cox proportional hazards model.
The number of HCC tumors is a well-known important indicator affecting the prognosis of HCC patients.Citation15,Citation16 The number of tumors not only reflects the liver tumor burden but also indicates intrahepatic metastasis and tumor staging of HCC. Multiple tumor staging systems, such as BCLC, CNLC, AJCC, and CLIP, use the number of tumors as a critical basis for staging.Citation17–20 Therefore, the greater the number of tumors, the later the stage and the worse the prognosis. The ALBI score, comprising bilirubin and albumin, serves as an indicator of liver function and parenchyma reserve, directly impacting HCC prognosis. Studies have shown that the ALBI classification has higher prognostic value than the Child-Pugh classification.Citation21–23 The presence of portal vein thrombosis increases the risk of metastasis and portal hypertension, leading to a higher likelihood of gastrointestinal bleeding, ascites, and liver failure. It is a significant factor affecting the prognosis of HCC patients. AFP is not only a reliable tumor marker for the diagnosis of hepatocellular carcinoma but also reflects tumor burden, portal vein thrombosis, and tumor biological characteristics.Citation24,Citation25 Changes in AFP can reliably predict the therapeutic effect, including TACE, surgery, chemotherapy, and systemic therapy. Multiple HCC staging systems and scoring models have incorporated AFP as a main indicator, demonstrating good predictive performance.Citation26
In addition to identifying independent factors affecting the efficacy and prognosis of DEB-TACE for HCC, the main goal of this study was to establish a DTH scoring system based on tumor number, ALBI grade, AFP, and PVTT. The survival time based on this scoring system shows a strong correlation between the DTH score and prognosis. As the DTH score increases, survival time gradually decreases. According to the DTH score, patients are divided into low-risk (DTH-A, 0–4 points), medium-risk (DTH-B, 5–6 points) and high-risk groups (HAP-C, 7 points), with median survival time of 18.73 months, 13.73 months and 8.62 months, respectively (P<0.001). The external validation cohort also confirmed the good predictive performance of the DTH scoring system. Therefore, the DTH scoring system constructed in this study can accurately predict the efficacy and prognosis of DEB-TACE for HCC.
Compared with BCLC, CNLC, CLIP, OKA and AJCC scoring systems, the DTH score demonstrated superior predictive ability for OS in two main aspects. First, from the survival curve plot (), it is evident that the survival curves for each DTH score group (A/B/C) are distinct and non-overlapping, whereas the survival curves for patients in each stage of BCLC, CNLC, CLIP, OKA and AJCC systems exhibit varying degrees of overlap, resulting in poor discrimination between groups. Second, based on the area under the ROC curve, the area under the ROC curve predicted by the DHT model for survival time is higher than that of other staging systems in all three cohorts (). Finally, multivariate Cox analysis comparing each scoring/stage system with patient survival rates at different stages shows that the DTH score has the strongest correlation with prognosis and the highest hazard ratio coefficient, indicating a robust ability to predict mortality (see ).
However, this study has several limitations: First, as a retrospective study, it is subject to inherent shortcomings such as selection bias and inconsistent follow-up. Currently, multidisciplinary treatment is advocated for advanced HCC, and the inconsistency of multidisciplinary treatment plans may affect the outcome. Second, the sample size is small, and constructing a predictive model with limited data may result in insufficient representation of clinical scenarios and introduce bias. Therefore, further multi-center, large-sample, prospective data verification is needed. Finally, due to individual patient differences and tumor complexity, even a predictive model with proven good performance may still have some uncertainty in real-world application. Thus, incorporating more tumor biological information or imaging genomics data could improve the accuracy of the predictive model.
The DTH scoring system proposed in this study includes the most commonly used data in clinical practice: imaging data (enhanced CT or MRI, with grading of the most important risk factor, portal vein tumor thrombus) and laboratory tests (tumor biomarker AFP). These factors can be simply classified to predict the efficacy of DEB-TACE treatment and guide physicians in selecting treatment options. It is a cost-effective, practical clinical tool with straightforward operation and accurate results. This system plays an important role in predicting the efficacy of DEB-TACE treatment, guiding treatment decisions, and improving the survival rate of patients with HCC.
Abbreviations
DEB-TACE, drug-eluting bead-transcatheter arterial chemoembolization; HCC, hepatocellular carcinoma; PVTT, portal vein tumor thrombus; ALBI, Albumin-bilirubin; AASLD, American Association for the Study of Liver Diseases; mRECIST, modified Response Evaluation Criteria In Solid Tumors; Ecog, Eastern Cooperative Oncology Group; CTCAE, Common Terminology Criteria for Adverse Events; BCLC, Barcelona Clinic Liver Cancer; PS, performance status; PHC, Primary hepatocellular carcinoma; OS, overall survival.
Disclosure
The authors declare that they have no conflict of interest.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Lortet-Tieulent J, Soerjomataram I, Lin CC, et al. Burden of cancer by race and ethnicity according to disability-adjusted life years. Am J Prev Med. 2016;51(5):673–681. doi:10.1016/j.amepre.2016.07.039
- Arii S, Tobe R. Treatment of liver cancer. Gan. 1957;1(5027):1110–1111.
- Chen J, Zhang Y, Cai H, et al. Comparison of the effects of postoperative prophylactic transcatheter arterial chemoembolization (TACE) and transhepatic arterial infusion (TAI) after hepatectomy for primary liver cancer. JBUON. 2018;23(3):629–634.
- Liu KC, Zhou CZ, Lv WF, et al. Factors to transcatheter arterial chemoembolization liver cancer stage C. Minimally Invasive Ther Allied Technol. 2020;29(1):49–55. doi:10.1080/13645706.2019.1575241
- Wu B, Zhou J, Ling G, et al. CalliSpheres drug-eluting beads versus lipiodol transarterial chemoembolization in the treatment of hepatocellular carcinoma: a short-term efficacy and safety study. World J Surg Oncol. 2018;16(1):69. doi:10.1186/s12957-018-1368-8
- Bargellini I, Lorenzoni V, Lorenzoni G, et al. Duration of response after DEB-TACE compared to lipiodol-TACE in HCC-nave patients: a propensity score matching analysis[J]. Eur Radiol. 2021;31(10):7512–7522. doi:10.1007/s00330-021-07905-x
- Xiang H, Long L, Yao Y, et al. CalliSpheres drug-eluting bead transcatheter arterial chemoembolization presents with better efficacy and equal safety compared to conventional TACE in treating patients with hepatocellular carcinoma. Technol Cancer Res Treat. 2019;1(18):1533033819830751.
- Shi ZX, Wang DQ, Kang TR, et al. Comparison of CalliSpheres® microspheres drug-eluting beads and conventional transarterial chemoembolization in hepatocellular carcinoma patients: a randomized controlled trial. Radiol Oncol. 2023;57(1):70–79. doi:10.2478/raon-2023-0001
- Melchiorre F, Patella F, Pescatori L, et al. DEB-TACE: a standard review. Future Oncol. 2018;14(28):2969–2984. doi:10.2217/fon-2018-0136
- Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380.
- Li N, Chen J. Efficacy and safety of drug-eluting bead transarterial chemoembolization (DEB-TACE) plus apatinib versus DEB-TACE alone in treating huge hepatocellular carcinoma patients. Irish J Med Sci. 2022;191(6):2611–2617. doi:10.1007/s11845-021-02884-w
- Zhu D, Yuan D, Wang Z, et al. Efficacy of drug-eluting bead transarterial chemoembolization (DEB-TACE) combined with radiofrequency ablation versus DEB-TACE alone in Chinese hepatocellular carcinoma patients[J]. Medicine. 2019;98(26):e15682. doi:10.1097/MD.0000000000015682
- Liu SS, Han YW, Zhang ZH, et al. Effectiveness of c-TACE combined with sorafenib versus c-TACE monotherapy in advanced hepatocellular carcinoma: a retrospective study. Clin Med Insights Oncol. 2023;17:117955492211466. doi:10.1177/11795549221146648
- Gu H, Li J, You N, et al. Efficacy and safety of apatinib combined with transarterial chemoembolization (TACE) in treating patients with recurrent hepatocellular carcinoma[J]. Ann Translat Med. 2020;8(24):1677. doi:10.21037/atm-20-7244
- Nam JY, Lee YB, Lee JH, et al. A prognostic prediction model of transarterial radioembolization in hepatocellular carcinoma: SNAP-HCC. Dig Dis Sci. 2022;67(1):329–336. doi:10.1007/s10620-021-06843-4
- Mazzaferro V, Sposito C, Zhou J, et al. Metroticket 2.0 model for analysis of competing risks of death following liver transplantation for hepatocellular carcinoma. Gastroenterology. 2017;154(1):128–139. doi:10.1053/j.gastro.2017.09.025
- Forner A, Reig ME, Lope CRD, et al. Current strategy for staging and treatment: the BCLC update and future prospects. Semin Liver Disease. 2010;30(1):61–74. doi:10.1055/s-0030-1247133
- Edge SB, Compton CC. The American joint committee on cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-4
- Perrone F, Daniele B, Gaeta GB, et al. Prospective validation of the CLIP score: a new prognostic system for patients with cirrhosis and hepatocellular carcinoma. Hepatology. 2000;31:840–845.
- Zhou J, Sun H, Wang Z, et al. Guidelines for the diagnosis and treatment of hepatocellular carcinoma (2019 edition). Liver Cancer. 2020;9(6):682–720. doi:10.1159/000509424
- Liu KC, Lv WF, Lu D, et al. Initial experience of drug-eluting bead-transcatheter arterial chemoembolization after lipiodol-based transcatheter arterial chemoembolization failure for patients with advanced hepatocellular carcinoma. Cancer Manag Res. 2021;19(13):7973–7980. doi:10.2147/CMAR.S332571
- Zou H, Yang X, Li QL, et al. A comparative study of albumin-bilirubin score with child-Pugh score, model for end-stage liver disease score and indocyanine green r15 in predicting posthepatectomy liver failure for hepatocellular carcinoma patients. Dig Dis. 2018;36(3):236–243. doi:10.1159/000486590
- Wang YY, Zhong JH, Su ZY, et al. Albumin-bilirubin versus child-Pugh score as a predictor of outcome after liver resection for hepatocellular carcinoma. Br J Surg. 2016;103(6):725–734. doi:10.1002/bjs.10095
- Tian M, Zhang X, Huang G, et al. Alpha-fetoprotein assessment for hepatocellular carcinoma after transarterial chemoembolization[J]. Abdom Radiol. 2019;44(10):3304–3311. doi:10.1007/s00261-019-02116-x
- Nicola P, Silvia B, Tiziana P, et al. Usefulness of alpha-fetoprotein response in patients treated with sorafenib for advanced hepatocellular carcinoma. J Hepatol. 2012;57(1):101–107. doi:10.1016/j.jhep.2012.02.016
- Kadalayil L, Benini R, Pallan L, et al. A simple prognostic scoring system for patients receiving transarterial embolisation for hepatocellular cancer[J]. Ann Oncol. 2013;24(10):2565–2570. doi:10.1093/annonc/mdt247