

Abstract
Background
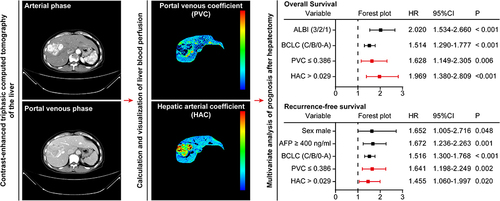
The dominant artery blood supply is a characteristic of hepatocellular carcinoma (HCC). However, it is not known whether the blood supply can predict the post-hepatectomy prognosis of patients with HCC. This retrospective study investigated the prognostic value of the portal venous and arterial blood supply estimated on triphasic liver CT (as a portal venous coefficient, PVC, and hepatic arterial coefficient, HAC, respectively) in patients with HCC following hepatectomy.
Methods
HCC patients who were tested by triphasic liver CT 2 weeks before hepatectomy and received R0 hepatectomy at the Second Affiliated Hospital, Kunming Medical University between January 1, 2016 and December 31, 2020, were retrospectively screened. Their PVC and HAC, and other variables were analyzed for the prediction of overall survival (OS) and recurrence-free survival (RFS) using the least absolute shrinkage and selection operator and Cox proportional hazard regression models.
Results
Four hundred and nineteen patients (53.2 ± 10.6 years of age and 370 men) were evaluated. A shorter OS was independently associated with higher blood albumin and total bilirubin grade [hazard ratio (HR) 2.020, 95% confidence interval (CI) 1.534–2.660], higher Barcelona Clinic Liver Cancer (BCLC) stage (HR 1.514, 95% CI 1.290–1.777), PVC ≤ 0.386 (HR 1.628, 95% CI 1.149–2.305), and HAC > 0.029 (HR 1.969, 95% CI 1.380–2.809). A shorter RFS was independently associated with male (HR 1.652, 95% CI 1.005–2.716), higher serum α-fetoprotein ≥ 400 ng/mL (HR 1.672, 95% CI 1.236–2.263), higher BCLC stage (HR 1.516, 95% CI 1.300–1.768), tumor PVC ≤ 0.386 (HR 1.641, 95% CI 1.198–2.249), and tumor HAC > 0.029 (HR 1.455, 95% CI 1.060–1.997).
Conclusion
Tumor PVC or HAC before hepatectomy is valuable for independently predicting postoperative survival of HCC patients.
Graphical Abstract
Abbreviations
ALBI grade, albumin, and total bilirubin grade; BCLC stage, Barcelona Clinic Liver Cancer stage; CI, confident interval; CT, computed tomography; HAC, hepatic arterial coefficient; HCC, hepatocellular carcinoma; HR, hazards ratio; IQR, inter-quartile range; LASSO, least absolute shrinkage selection operator; PVC, portal venous coefficient; OS, overall survival; RFS, recurrence-free survival; ROI, regions of interest; TACE, transcatheter arterial chemoembolization.
Data Sharing Statement
The datasets used and/or analyzed during the current study and the CALVIS LIVER PERFUSION software are available from the corresponding author Y.K. upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Committee of Ethics at the Second Affiliated Hospital, Kunming Medical University (Shen-PJ-Ke-2022-60). Written informed consent was waived by the Committee of Ethics as its retrospective collection.
Acknowledgments
The current affiliation of Dr. Yu-Shan Wu is Department of Gastroenterology, West China Hospital, Sichuan University, Chengdu 610041, SC, China. The current affiliation of Dr. Wei-Hu Zhang is Department of Radiology, Northeast Yunnan Regional Central Hospital, Zhaotong 657000, YN, China.
Disclosure
All authors declare that they have no competing interests in this work.