
Abstract
Background
Recent clinical studies have revealed that sodium glucose co-transporter 2 inhibitors (SGLT2i) reduced cardiovascular events in type 2 diabetes. Here, we investigated whether empagliflozin, as a kind of SGLT2i, could alleviate atherosclerosis progression in non-diabetic mice.
Methods
ApoE-/- mice were fed on a western diet for 12 weeks to induce atherosclerosis. The treatment group of mice was treated with drinking water containing empagliflozin (10mg/kg/day). On the 12th week, the whole aortas of each group were harvested. HE and Movat staining were performed for atherosclerotic lesion area and size. CD 68 and MCP-1 immunohistochemistry were used to evaluate inflammatory cell infiltration. Mouse serum lipid profiles (total cholesterol, triglyceride, low-density lipoprotein-C, and high-density lipoprotein-C), systemic inflammation level (IL-1β, IL-6 and IL-10), renin-angiotensin-aldosterone system (RAAS) and sympathetic activity (norepinephrine and neuropeptide Y) were measured by ELISA.
Results
Empagliflozin could reduce the atherosclerotic lesion areas. Specifically, empagliflozin could significantly decreased inflammatory levels, RAAS and sympathetic activity in vivo. In vitro studies also showed that empagliflozin could inhibit IL-1β expression in oxLDL-treated macrophages by regulating NF-κB signaling.
Conclusion
Empagliflozin could prevent atherosclerosis by repressing inflammation and sympathetic activity.
Introduction
Sodium-glucose cotransporter 2 (SGLT2) is involved in glucose reabsorption and excretion in the renal proximal tubule, making it a newest anti-diabetic target.Citation1,Citation2 Interestingly, large clinical trials have confirmed the safety and efficacy of sodium-glucose cotransporter 2 inhibitor (SGLT2i) in reducing cardiovascular events and hospitalization for heart failure of diabetic patients.Citation3–Citation5 What is more, the cardioprotective and renoprotective role of SGLT2i in non-diabetic patients have been confirmed in some recent clinical trials, such as Dapagliflozin And Prevention of Adverse-outcomes in Heart Failure (DAPA-HF),Citation6 Dapagliflozin in Patients with Chronic Kidney Disease (DAPA-CKD)Citation7 and EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Reduced Ejection Fraction (EMPEROR-Reduced).Citation8 A number of studies speculated that its cardioprotective effect could be related to the inhibition of oxidative stress,Citation9 regulation of inflammatory response,Citation10 and improved cardiac metabolism.Citation11 Preclinical data found that empagliflozin could also reduce arterial stiffness and atherosclerosis.Citation12–Citation14
Atherosclerosis, a common pathologic process implicated in cardiovascular diseases, is characterized by fat deposition and chronic inflammation within the artery wall.Citation15 Myocardial infarction and stroke, as complications of atherosclerosis, are a serious threat to human health, making it necessarily to develop effective treatments.Citation16 Systematic review and meta-analysis also reported that SGLT2i could reduce the major adverse cardiac events in diabetic patients.Citation17,Citation18 However, the potential role and mechanisms of SGLT2i in atherosclerosis without diabetes are not fully understood.
In our study, we hypothesized that empagliflozin can inhibit the progression of atherosclerosis in a non-diabetic model in terms of lipid lowering, anti-inflammation response, and regulation of sympathetic activity and RAAS.
Materials and Methods
Animals
ApoE(−/−) male mice (6–8 weeks) were purchased from Model Animal Research Center of Nanjing University and kept in the animal room of Nanjing Drum Tower Hospital. Mice were kept under 12 h/12 h light/dark cycles with free access to food and water. After 1 week of adaptation to the housing environment, the mice were divided into three groups according to drug administration: (1) the Control group fed a chow diet; (2) the AS group fed a western diet containing 0.2% (wt/wt) cholesterol and 42% fat (#TP26303, TROPHIC Co., Ltd, Jiangsu) for 12 weeks; (3) the EMPA group fed a western diet plus received drinking water containing 10 mg/kg/d of empagliflozin (CAS No: 864070–44-0, MedChemExpress, China) for 12 weeks. Each group had 6 mice. All mouse studies were approved by the Nanjing University Animal Care and Use Committee (No. 2019AE01062) and were in accordance with the ARRIVE guidelines.
Histological and Immunohistochemical Analysis
After 12 weeks, mice were killed after cervical dislocation. After perfusion of phosphate buffer saline, the heart and the whole aorta were exposed and separated. To measure the atherosclerotic lesion area in aortic sinus, the lower ventricular portion of heart was removed at the site of 0.5 cm below the line connecting the left and right auricles. The remaining part of heart and proximal aorta was fixed in 4% paraformaldehyde for 24 hours at room temperature and embedded in paraffin. Serial 10-μm-thick sections from the ascending aortic segment to the aortic sinus were collected. Slides were stained with hematoxylin-eosin or Movat (Sevicebio, Wuhan). For immunohistochemistry, slides were incubated with CD68 (Abcam, ab125212) and MCP-1 (R&D, AF479) overnight and subsequent goat anti-mouse secondary antibody. Images were captured using the high-resolution camera. A person blind to treatment group measured aortic atherosclerosis lesion. Lesion size was analyzed with Images J software (NIH, USA) by averaging 3 sections of each aorta (n=6).
Enzyme-Linked Immunosorbent Assay
At the end of study, blood samples were collected and biochemical variables were measured using standard methods after mice had been fasted for 8 h. Lipids (triacylglycerol [TG; JEB-12909], total-cholesterol [TC; JEB-12596], HDL-cholesterol [HDL-C; JEB-12844] and LDL-cholesterol [LDL-C; JEB-12978]), inflammatory factors (IL-1β [JEB-12786], IL-6 [JEB-12267] and IL-10 [JEB-12260]), RAAS mediators (renin [JEB-12525], angiotensin II [JEB-12350] and aldosterone [JEB-15659]), sympathetic mediators (norepinephrine [JEB-12971] and neuropeptide Y [JEB-12756]) and glucose (JEB-15224) were measured by mouse ELISA kits (Jin Yibai Biological Technology Co. Ltd, Nanjing) according to the manufacturer’s instructions using standard curve. The sensitivities for these indexes were 0.16 mmol/L (TC), 0.32 mmol/L (TG), 0.2 mmol/L (LDL-C), 0.2 mmol/L (HDL-C), 5 ng/L (IL-1β), 5 pg/mL (IL-6), 30 pg/mL (IL-10), 5 ng/L (renin), 20 ng/L (AngII), 5 ng/L (ALD), 5 ng/L (NE), and 4.5 ng/L (NPY). The optical densities of the samples were detected using a microplate reader (BIOTEK, USA) at a wavelength of 450 nm. All results are shown in .
Table 1 The Results of ELISA Between Sham, AS and EMPA Group
Cell Culture
The RAW 264.7 macrophages were obtained from ATCC and cultured in DMEM medium supplemented with 10% fetal bovine serum and 1% penicillin/streptomycin in humidified air, 5% CO2 at 37°C. A group of cells was treated with oxLDL (50 ug/mL) for 24 hours while treatment group was incubated with oxLDL (50 ug/mL) and EMPA (10 μM) for 24 hours. The group of cells incubated with PBS was set as control.
Lipid Uptake Assay
When reaching a good growth condition, macrophages were cultured in starvation medium without serum for 16 hours and then treated with fluorescence-labeled oxLDL (Dil-oxLDL; 30 μg/mL) for an additional 4 hours. Cells were then washed and examined by flow cytometry. The uptake of oxLDL was measured as mean fluorescent intensity by flowJo.
MTT Assay
The viability of cells was determined using the standard MTT [3-(4,5-dimethylthiazol2-yl)-2,5-diphenyltetrazolium bromide] assay. All treatments were done using 1×104 cells/well in 96 wells plate and allowed to grow for 24 h. On the last day, the supernatant of each well was removed and washed twice with PBS. Then, 20 µL of MTT solution and 100 µL of medium were added. After incubation for 1h, dimethyl sulfoxide (100 µL) was added and the absorbance intensity measured by a microplate reader (BioTek, USA) at 490 nm with a reference wavelength of 620 nm. All experiments were performed in triplicate, and the relative cell viability (%) was expressed as a percentage relative to the untreated control cells.
Real-Time Quantitative Polymerase Chain Reaction Analysis
Total RNA was extracted from the RAW 264.7 macrophages using RNAiso plus (TaKaRa; Japan) according to the manufacturer’s instructions. 1 μg of RNA was reverse transcribed into cDNA with HiScriptII Q RT SuperMix (Vazyme; China) and quantitative RT-PCR was performed with ChamQ SYBR qPCR Master Mix (Vazyme; China) according to the protocol. All the results were normalized against glyceraldehyde-3-phosphate dehydrogenase (GAPDH) expression.
Western Blotting
Total protein was extracted from RAW 264.7 cells using a RIPA buffer. The protein concentrations were determined using a BCA kit (Thermo Fisher Scientific, USA). Protein lysate was subjected to SDS‐PAGE, and the separated proteins were transferred to polyvinylidene fluoride (PVDF) membranes (Millipore, USA) as previously described. After blocking for 2 hours with 5% non‐fat milk at room temperature, the PVDF membranes were incubated with the corresponding primary antibodies overnight at 4°C before being incubated with goat anti‐rabbit IgG secondary antibodies for 1 hour at room temperature.
Statistical Analysis
Data was presented as mean± standard deviation. One-way analysis of variance with the Bonferroni post hoc test was used for multiple comparisons. P<0.05 was considered statistically significant. P<0.05 was considered as statistical significance. All statistical analyses were performed using Prism 8 (GraphPad Software, USA).
Results
SGLT2i Attenuated Atherosclerotic Lesion Area and Size
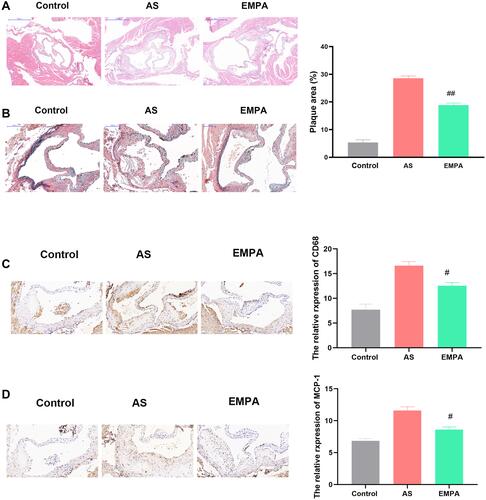
HE () and Movat staining () analysis showed that AS group had significant plaque accumulating in the aortic sinus, while empagliflozin treatment at a dose of 10 mg/kg/day for 12 weeks significantly reduced lesion size in EMPA group (~29% vs 19%, p<0.01). Immunohistochemistry results also showed that the expression of CD68 () and MCP-1 (), markers of inflammatory cells infiltration, were downregulated in EMPA group. These results suggested that SGLT2i significantly inhibited inflammation response and mitigated atherogenesis process.
Figure 1 Empagliflozin attenuated atherosclerotic lesion areas. Representative HE staining (A), Movat staining (B), CD68 immunohistochemistry (C) ang MCP-1 immunohistochemistry (D) of Sham, AS and EMPA group. #p<0.05, ##p<0.01.
SGLT2i Minimally Decreased Lipid Level in Atherosclerosis
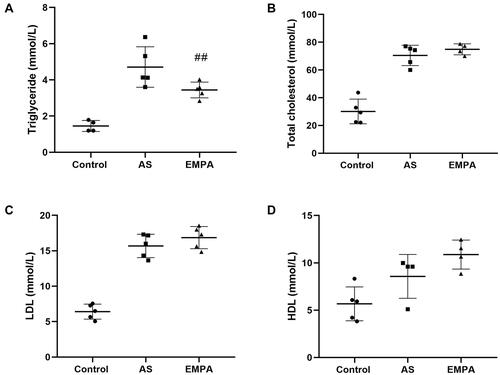
Excess lipid deposits contributed to the initiation of atherosclerosis. Therefore, we evaluated the effect of empagliflozin on lipid profiles. Our results showed that the mice in the EMPA groups appeared a significant reduction in triglyceride levels (3.44 mmol/L in the EMPA group vs 4.71 mmol/L in the AS group, p<0.01) after 12 weeks of treatment (). While total-cholesterol () and LDL-cholesterol () in EMPA group were not significantly different between groups. HDL-cholesterol levels () in empagliflozin-treated mice were higher than those in the control or AS groups (10.88 vs 8.57 mmol/L, p=0.12).
Figure 2 The serum level of triglyceride (A), total cholesterol (B), LDL (C) and HDL (D) between Sham, AS and EMPA group. ##p<0.01.
SGLT2i Alleviated Systemic Inflammation in Atherosclerosis
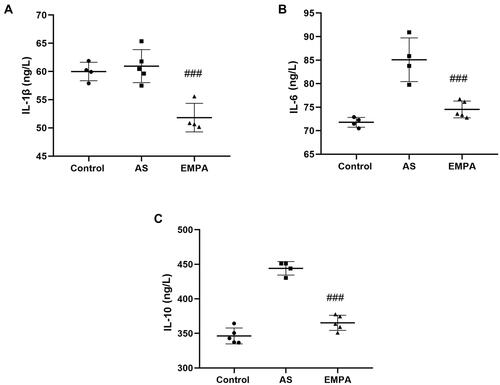
Chronic inflammation is also an important trigger of atherosclerosis. To evaluate the effect of EMPA treatment on the expression of inflammatory factors (IL-1β, IL-6, IL-10), total RNAs were isolated and analyzed using real-time quantitative RT-PCR. We found that EMPA treatment significantly reduced IL-1β (51.8 ng/L vs 61.0 ng/L, p<0.001; ), IL-6 (74.5 pg/mL vs 85.1 pg/mL, p<0.001; ), and IL-10 (365.3 pg/mL vs 444.1 pg/mL, p<0.001; ) expression compared to AS group. These results suggested that EMPA played a great anti-inflammation role.
Figure 3 The serum level of IL-1β (A), IL-6 (B), and IL-10 (C) between Sham, AS and EMPA group. ###p<0.001.
SGLT2i Inhibited Renin-Angiotensin-Aldosterone System (RAAS) and Reduces Sympathetic Activity in Atherosclerosis
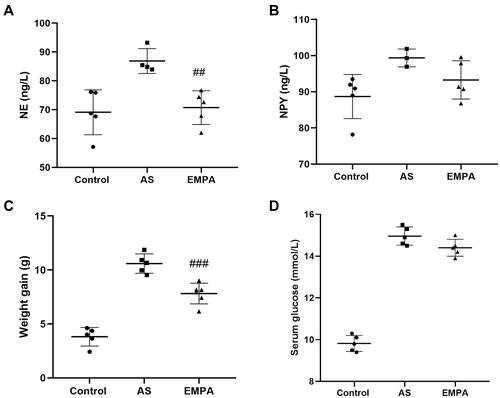
The chronic activation of RAAS was a detrimental factor in the cardiovascular diseases. Our results showed that renin (), angiotensin II () and aldosterone () were increased in AS group while they were inhibited in EMPA group (143.0 ng/L vs 158.3 ng/L for Renin, p<0.01; 113.5 ng/L vs 132.5 ng/L for ALD, p<0.01) other than angiotensin II. It indicated that empagliflozin could alleviate the activation of RAAS. In addition to RAAS, sympathetic activation also speeds up the progression of atherosclerosis. We found that norepinephrine (70.7 ng/L vs 86.9 ng/L, p<0.01; ) and neuropeptide Y (93.3 ng/L vs 99.4 ng/L, p<0.01; ) were partially inhibited in the EMPA group. Interestingly, empagliflozin also decreased the body weight gain () of AS mice to a degree (−2.78 g, p<0.001). Additionally, empagliflozin administration did not affect glucose levels ().
Figure 4 The serum level of renin (A), angiotensin II (B) and aldosterone (C) between groups. ##p<0.01 and ###p<0.001.
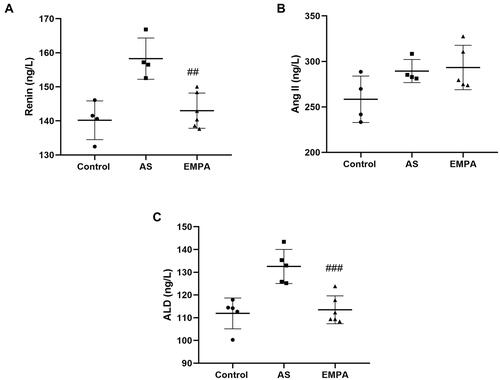
Figure 5 The serum level of norepinephrine (A) and neuropeptide Y (B) and body weight (C) and glucose (D) between Sham, AS and EMPA group. ##p<0.01 and ###p<0.001.
SGLT2i Reduced the Expression of IL-1β by Inhibiting NF-κB Signaling in Macrophages
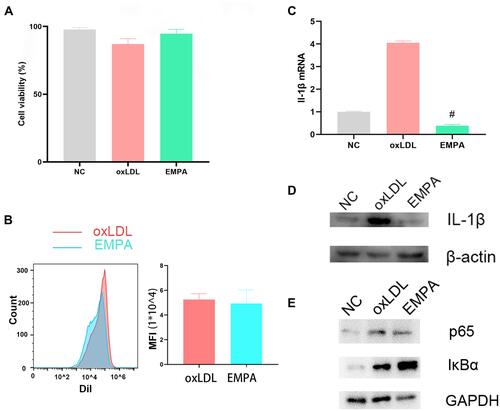
To observe the effect of SGLT2i on macrophage, we treated oxLDL-stimulated macrophages with empagliflozin. MTT results showed that cell viability was not significantly different between groups (), excluding the possibility of affecting the cell number. Besides, flow cytometry showed that empagliflozin had no effect on the uptake of Dil-labeled oxLDL in macrophage (). Interestingly, empagliflozin could significantly reduce the expression of IL-1β mRNA and protein ( and ). It was observed that IκBα was decreased while p65 was upregulated upon empagliflozin treatment, suggesting of an anti-inflammatory role by modulating NF-κB signaling pathway ().
Figure 6 The cell viability of each group was examined by MTT assay (A). Qualitative (B; Left) and quantitative (B; Right) intensity of Dil-labeled oxLDL taken by macrophages between groups was examined by flow cytometry. The expression of IL-1β mRNA (C) and IL-1β protein (D) after empagliflozin treatment. (E) The protein expression of IκBα and p65. #p<0.05.
Discussion
This study demonstrated that empagliflozin could alleviate atherosclerosis progression by mitigating systemic and local inflammation, RAAS and sympathetic activity in ApoE-/- mice. However, the lipid-lowering effect was not significant. In vitro results also showed that empagliflozin inhibited inflammation by downregulating NF-κB signaling.
A magnitude of investigations supported that inflammatory cells and mediators promoted the atherosclerosis progression, while anti-inflammatory treatments could reduce the risk of atherosclerosis.Citation19,Citation20 The inflammatory mediators contribute to virtually all stages of the atherosclerotic process, including endothelial dysfunction, lipid oxidation and plaque destabilization/rupture.Citation21 Our study found that inflammatory cytokines were decreased in the serum of atherosclerotic mouse treated with empagliflozin, indicating the anti-inflammatory property of empagliflozin. In vitro experiments also show that IL-1β was significantly decreased after empagliflozin treatment. CANTOS trial showed that IL-1β antibody exerted cardioprotective effects.Citation22 So, we speculated that IL-1β reduction by empagliflozin may be of additional value in terms of atherosclerosis progression. In consistent with our results, Lee et al reported that SGLT2i could modulate inflammation response by Toll-like receptor 4/nuclear factor-kappa B signaling pathway in a normoglycemic rabbit model.Citation23 Other studies also demonstrated that SGLT2i could attenuate inflammation by promoting M2 polarization and inhibiting inflammasome activity.Citation24–Citation27
The chronic activation of Renin-Angiotensin-Aldosterone System (RAAS)Citation28 and sympathetic activationCitation29 were detrimental factors in the progression of atherosclerosis. We also showed that empagliflozin significantly reduced expressions of norepinephrine as well as renin, and aldosterone. However, angiotensin II was not statistically changed by empagliflozin treatment, which could be supplemented from other source. Maybe it was better to measure the urine Ang II and angiotensinogen levels.Citation30 What is more, body weight of the empagliflozin-treated group was also lower than those of the untreated group. Weight-loss effects of canagliflozin, another type of SGLT2i, have been demonstrated in clinical trials,Citation31 and our data supported their results. SGLT2i could regulate the differentiation of epicardial adipose tissue and perivascular adipose tissue, as well as improve insulin resistance and fat distribution.Citation32 So, we speculated that empagliflozin could decrease fat mass induced by a high fat diet.
Strikingly, lipid-lowering effect was not obvious in our results. Serum lipid profiles were not significant changed except triglyceride, which was consistent with previous results that SGLT2i lead to decreased levels of triglyceride and increased levels of LDL-C in human,Citation33 which was due to reduced clearance of LDL from the circulation and greater lipolysis of triglyceride-rich lipoproteins. In terms of HDL-cholesterol, our data were in line with previous results that empagliflozin, resulted in increased HDL.Citation34 Our in vitro results also showed that empagliflozin had no effect on lipid uptake of macrophages. Additionally, empagliflozin administration did not affect glucose levels. Our results were in consistent with a previous study.Citation35
The mechanisms underlying the vascular beneficial effect of SGLT2i have attracted much attention. In diabetic states, SGLT2i might enhance glycemic control and lipoprotein clearance,Citation36 while lowering sympathetic activation.Citation37 While in non-diabetic conditions, SGLT2i protected atherosclerosis possibly via the prevention of inflammation rather than of hyperlipidemia.Citation38 Also, SGLT2i could increase adiponectin levels and reduce expression of adhesion molecules and cytokine.Citation39 Besides, Gaspari et al found SGLT2i attenuated human vascular endothelial cell activation and induced vasorelaxation to inhibit atherogenesis.Citation40 SGLT2i had a beneficial effect on the progression of atherosclerosis, partially explaining its cardioprotective effect. The molecular mechanism deserved to be investigated in the future experiments. Besides, this study was an animal experiment, and further clinical trials should be conducted for its application in atherosclerosis.
In summary, SGLT2i could mitigate the progression of atherosclerotic plaques in ApoE-/- mice by inhibiting systematic inflammation and local inflammatory cells infiltration, which laid a foundation for the prevention and treatment of atherosclerosis in the clinical practice.
Data Sharing Statement
All data are available from the corresponding author upon reasonable request.
Ethical Approval
The study was approved by the Nanjing University Animal Care and Use Committee (No. 2019AE01062)
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Funding
References
- Cuypers J, Mathieu C, Benhalima K. SGLT2-inhibitors: a novel class for the treatment of type 2 diabetes introduction of SGLT2-inhibitors in clinical practice. Acta Clin Belg. 2013;68(4):287–293. doi:10.2143/ACB.3349
- Marsenic O. Glucose control by the kidney: an emerging target in diabetes. Am J Kidney Dis. 2009;53(5):875–883. doi:10.1053/j.ajkd.2008.12.031
- Fitchett D, Inzucchi SE, Cannon CP, et al. Empagliflozin reduced mortality and hospitalization for heart failure across the spectrum of cardiovascular risk in the EMPA-REG OUTCOME trial. Circulation. 2019;139(11):1384–1395. doi:10.1161/CIRCULATIONAHA.118.037778
- Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–657. doi:10.1056/NEJMoa1611925
- Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–357. doi:10.1056/NEJMoa1812389
- McMurray JJV, DeMets DL, Inzucchi SE, et al. The dapagliflozin and prevention of adverse-outcomes in heart failure (DAPA-HF) trial: baseline characteristics. Eur J Heart Fail. 2019;21(11):1402–1411. doi:10.1002/ejhf.1548
- Heerspink HJL, Stefansson BV, Correa-Rotter R, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436–1446. doi:10.1056/NEJMoa2024816
- Packer M, Anker SD, Butler J, et al. Empagliflozin in patients with heart failure, reduced ejection fraction, and volume overload: EMPEROR-reduced trial. J Am Coll Cardiol. 2021;77(11):1381–1392. doi:10.1016/j.jacc.2021.01.033
- Andreadou I, Efentakis P, Balafas E, et al. Empagliflozin limits myocardial infarction in vivo and cell death in vitro: role of STAT3, mitochondria, and redox aspects. Front Physiol. 2017;8:1077. doi:10.3389/fphys.2017.01077
- Leng W, Ouyang X, Lei X, et al. The SGLT-2 inhibitor dapagliflozin has a therapeutic effect on atherosclerosis in diabetic ApoE(-/-) mice. Mediators Inflamm. 2016;2016:6305735. doi:10.1155/2016/6305735
- Garcia-Ropero A, Santos-Gallego CG, Zafar MU, et al. Metabolism of the failing heart and the impact of SGLT2 inhibitors. Expert Opin Drug Metab Toxicol. 2019;15(4):275–285. doi:10.1080/17425255.2019.1588886
- Lamacchia O, Sorrentino MR. Diabetes mellitus, arterial stiffness and cardiovascular disease: clinical implications and the influence of SGLT2i. Curr Vasc Pharmacol. 2020;19(2):233–240. doi:10.2174/1570161118666200317150359
- Hidalgo Santiago JC, Maraver Delgado J, Cayon Blanco M, et al. Effect of dapagliflozin on arterial stiffness in patients with type 2 diabetes mellitus. Med Clin. 2020;154(5):171–174. doi:10.1016/j.medcli.2019.05.028
- Al-Sharea A, Murphy AJ, Huggins LA, et al. SGLT2 inhibition reduces atherosclerosis by enhancing lipoprotein clearance in Ldlr(-/-) type 1 diabetic mice. Atherosclerosis. 2018;271:166–176. doi:10.1016/j.atherosclerosis.2018.02.028
- Hansson GK, Libby P. The immune response in atherosclerosis: a double-edged sword. Nat Rev Immunol. 2006;6(7):508–519. doi:10.1038/nri1882
- Wang C, Niimi M, Watanabe T, et al. Treatment of atherosclerosis by traditional Chinese medicine: questions and quandaries. Atherosclerosis. 2018;277:136–144. doi:10.1016/j.atherosclerosis.2018.08.039
- Palmer SC, Tendal B, Mustafa RA, et al. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2021;372:m4573. doi:10.1136/bmj.m4573
- Li CX, Liang S, Gao L, et al. Cardiovascular outcomes associated with SGLT-2 inhibitors versus other glucose-lowering drugs in patients with type 2 diabetes: a real-world systematic review and meta-analysis. PLoS One. 2021;16(2):e0244689. doi:10.1371/journal.pone.0244689
- Raggi P, Genest J, Giles JT, et al. Role of inflammation in the pathogenesis of atherosclerosis and therapeutic interventions. Atherosclerosis. 2018;276:98–108. doi:10.1016/j.atherosclerosis.2018.07.014
- Shah PK. Inflammation, infection and atherosclerosis. Trends Cardiovasc Med. 2019;29(8):468–472. doi:10.1016/j.tcm.2019.01.004
- Prattichizzo F, De Nigris V, Micheloni S, et al. Increases in circulating levels of ketone bodies and cardiovascular protection with SGLT2 inhibitors: is low-grade inflammation the neglected component? Diabetes Obes Metab. 2018;20(11):2515–2522. doi:10.1111/dom.13488
- Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
- Lee SG, Lee SJ, Lee JJ, et al. Anti-inflammatory effect for atherosclerosis progression by sodium-glucose cotransporter 2 (SGLT-2) inhibitor in a normoglycemic rabbit model. Korean Circ J. 2020;50(5):443–457. doi:10.4070/kcj.2019.0296
- Lee TM, Chang NC, Lin SZ. Dapagliflozin, a selective SGLT2 inhibitor, attenuated cardiac fibrosis by regulating the macrophage polarization via STAT3 signaling in infarcted rat hearts. Free Radic Biol Med. 2017;104:298–310. doi:10.1016/j.freeradbiomed.2017.01.035
- Xu L, Nagata N, Nagashimada M, et al. SGLT2 inhibition by empagliflozin promotes fat utilization and browning and attenuates inflammation and insulin resistance by polarizing M2 macrophages in diet-induced obese mice. EBioMedicine. 2017;20:137–149. doi:10.1016/j.ebiom.2017.05.028
- Miyachi Y, Tsuchiya K, Shiba K, et al. A reduced M1-like/M2-like ratio of macrophages in healthy adipose tissue expansion during SGLT2 inhibition. Sci Rep. 2018;8(1):16113. doi:10.1038/s41598-018-34305-x
- Kim SR, Lee SG, Kim SH, et al. SGLT2 inhibition modulates NLRP3 inflammasome activity via ketones and insulin in diabetes with cardiovascular disease. Nat Commun. 2020;11(1):2127. doi:10.1038/s41467-020-15983-6
- de Souza P, da Silva LM, de Andrade SF, et al. Recent advances in the knowledge of naturally-derived bioactive compounds as modulating agents of the renin-angiotensin-aldosterone system: therapeutic benefits in cardiovascular diseases. Curr Pharm Des. 2019;25(6):670–684. doi:10.2174/1381612825666190329122443
- Liu L, Zhao M, Yu X, et al. Pharmacological modulation of vagal nerve activity in cardiovascular diseases. Neurosci Bull. 2019;35(1):156–166. doi:10.1007/s12264-018-0286-7
- Shin SJ, Chung S, Kim SJ, et al. Effect of sodium-glucose co-transporter 2 inhibitor, dapagliflozin, on renal renin-angiotensin system in an animal model of type 2 diabetes. PLoS One. 2016;11(11):e0165703. doi:10.1371/journal.pone.0165703
- Cefalu WT, Leiter LA, Yoon KH, et al. Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, phase 3 non-inferiority trial. Lancet. 2013;382(9896):941–950. doi:10.1016/S0140-6736(13)60683-2
- Neeland IJ, McGuire DK, Chilton R, et al. Empagliflozin reduces body weight and indices of adipose distribution in patients with type 2 diabetes mellitus. Diab Vasc Dis Res. 2016;13(2):119–126. doi:10.1177/1479164115616901
- Basu D, Huggins LA, Scerbo D, et al. Mechanism of increased LDL (low-density lipoprotein) and decreased triglycerides with SGLT2 (sodium-glucose cotransporter 2) inhibition. Arterioscler Thromb Vasc Biol. 2018;38(9):2207–2216. doi:10.1161/ATVBAHA.118.311339
- Dimitriadis GK, Nasiri-Ansari N, Agrogiannis G, et al. Empagliflozin improves primary haemodynamic parameters and attenuates the development of atherosclerosis in high fat diet fed APOE knockout mice. Mol Cell Endocrinol. 2019;494:110487. doi:10.1016/j.mce.2019.110487
- Ortega R, Collado A, Selles F, et al. SGLT-2 (Sodium-Glucose Cotransporter 2) Inhibition Reduces Ang II (Angiotensin II)-Induced Dissecting Abdominal Aortic Aneurysm in ApoE (Apolipoprotein E) Knockout Mice. Arterioscler Thromb Vasc Biol. 2019;39(8):1614–1628. doi:10.1161/ATVBAHA.119.312659
- Pennig J, Scherrer P, Gissler MC, et al. Glucose lowering by SGLT2-inhibitor empagliflozin accelerates atherosclerosis regression in hyperglycemic STZ-diabetic mice. Sci Rep. 2019;9(1):17937. doi:10.1038/s41598-019-54224-9
- Gragnano F, Calabro P. Role of dual lipid-lowering therapy in coronary atherosclerosis regression: evidence from recent studies. Atherosclerosis. 2018;269:219–228. doi:10.1016/j.atherosclerosis.2018.01.012
- Nakatsu Y, Kokubo H, Bumdelger B, et al. The SGLT2 inhibitor luseogliflozin rapidly normalizes aortic mRNA levels of inflammation-related but not lipid-metabolism-related genes and suppresses atherosclerosis in diabetic ApoE KO mice. Int J Mol Sci. 2017;18(8). doi:10.3390/ijms18081704
- Han JH, Oh TJ, Lee G, et al. The beneficial effects of empagliflozin, an SGLT2 inhibitor, on atherosclerosis in ApoE (-/-) mice fed a western diet. Diabetologia. 2017;60(2):364–376. doi:10.1007/s00125-016-4158-2
- Gaspari T, Spizzo I, Liu H, et al. Dapagliflozin attenuates human vascular endothelial cell activation and induces vasorelaxation: a potential mechanism for inhibition of atherogenesis. Diab Vasc Dis Res. 2018;15(1):64–73. doi:10.1177/1479164117733626