Abstract
Background
Follicular cell thyroid carcinoma is a quite aggressive form of thyroid cancer. About 10% of follicular thyroid carcinoma shows multiple metastases: lung and bone are the most common sites of metastasis. Renal involvement from thyroid primary cancer is very rare with incidence of 4.5%–5.9%.
Purpose
We report the first laparoscopic conservative treatment of renal metastasis from thyroid cancer. This is a new and useful approach in order to delay malignant disease progression and to reduce the surgical discomfort of the patient.
Patients and methods
We present the case of a 67-year-old woman, undergoing total thyroidectomy for follicular thyroid cancer with bone and lung metastasis. During adjuvant radiometabolic treatment, renal metastasis was diagnosed. Renal metastasis showed high metabolic activity, reducing the effectiveness of radioiodine therapy for secondary lesions. For this reason, we performed a laparoscopic simple enucleation of the single renal metastasis using extraperitoneal access and a clampless procedure.
Results
The excision of the renal lesion improved the effectiveness of adjuvant radioiodine therapy: two months after surgery, the patient underwent adjuvant radiometabolic treatment with iodine-131 (150 mCi) and the following whole body scan showed only a small uptaking area at the level of the vertebral metastasis. The lung micrometastases were not detectable. At 36 months follow-up, malignant disease was clinically stable and well controlled.
Conclusion
Minimally invasive renal surgery with preservation of renal function and rapid recovery contributed to the success of radioiodine therapy and delayed the progression of the disease.
Introduction
Despite the high frequency of nodular thyroid disease, malignancies are not common (3%–5%). Thyroid carcinoma represents 1.6% of all male cancers and 5% of female ones.Citation1 The incidence is 41 cases per 10,000,000 men and 100–120 cases per 10,000,000 women between the fifth and eighth decade.Citation2 The American Cancer Society has estimated 56,460 expected new cases of thyroid carcinoma in the US in 2012 and 1780 expected thyroid cancer related deaths.Citation1 In 2009 in the US, about 1600 deaths occurred in about 300,000 patients affected by this tumor.Citation2
Histopathologically, most thyroid cancers are well-differentiated. Generally the prognosis is favorable and the survival rate is over 90% at 10 years after diagnosis. Among the well-differentiated forms, follicular carcinoma is the most aggressive because it has a propensity for vascular invasion and hematogenous spread. The most common sites of metastasis are lung and bone, less frequently brain, liver, skin, kidney, and adrenal gland.Citation3–Citation5 However, overall survival at 5, 10, and 20 years for patients with follicular thyroid cancer is 85%, 80%, and 76%, respectively.Citation5,Citation6
We present the case of a 67-year-old female, undergoing total thyroidectomy for follicular thyroid cancer metastasizing bone. During adjuvant radiotherapy, renal metastasis was diagnosed. We performed laparoscopic extraperitoneal simple enucleation of the renal lesion in order to allow more rapid recovery of general health and to ensure more effective and earlier adjuvant radiometabolic treatment.
Material and methods
Due to chest pain, a 67-year-old woman underwent a chest-abdomen computed tomography (CT) scan, that showed osteolysis of the soma of D3 with complete destruction of the posterior wall, infiltration of the spinal canal, and some low-density nodular opacities in both lungs. The biopsy of the bone injury showed wide infiltration by tumoral cells with the pattern of follicular thyroid cancer. After 16 Gy local radiotherapy, magnetic resonance imaging confirmed the findings of the CT scan and also detected similar injury at the level of D4. Therefore, the patient underwent decompressive laminectomy of the D3–D4 tract and stabilization of the D1–D6 tract. Furthermore, total thyroidectomy was performed due to the presence of a 1.1 cm left lobe thyroid nodule. Histological examination revealed follicular thyroid carcinoma (pT1bN0M1, stage IVC, according to the 2009 tumor, node, metastasis [TNM] classification).Citation7 Immunohistochemical analysis confirmed the histological findings, showing positive results for galectin-3, HBME1, and CK19.
After thyroidectomy, serum thyroglobulin was 1339 ng/mL, thyroid-stimulating hormone (TSH) under the lack of L-thyroxine was 0.3 mU/L (range 0.4–4.0 mU/L), and antithyroglobulin antibody was negative.
After 3 months, the patient underwent radiometabolic treatment with 1852 MBq (50.05 mCi) of iodine-131 (131I). The following single-photon emission CT and 131I whole body scan (WBS) showed two large foci of increased uptake at the D3 vertebral soma and the lower pole of the left kidney, both reported to be metastases ( and ). An abdominal CT scan showed a hypodense area of 2 cm × 2 cm at the lower pole of the left kidney with obvious contrast enhancement. In order to obtain a debulking of the surgically removable tumor mass, we performed a laparoscopic simple enucleation of the renal tumor (), using extraperitoneal access and a clampless procedure: the renal artery was only isolated and dissected, avoiding ischemia of the healthy tissue. Hemostasis was achieved using a combination of radiolucent clips (Weck Hem-o-lock clips; Teleflex Incorporated, Limerick, PA, USA), intracorporeal suturing, and hemostatic material. Surgery was considered necessary in order to reduce the tumor burden to be treated by radioactive iodine and to increase the chance of its efficacy of vertebral and lung metastases treatment.
Figure 1 SPECT.
Abbreviation: SPECT, single-photon emission computed tomography.
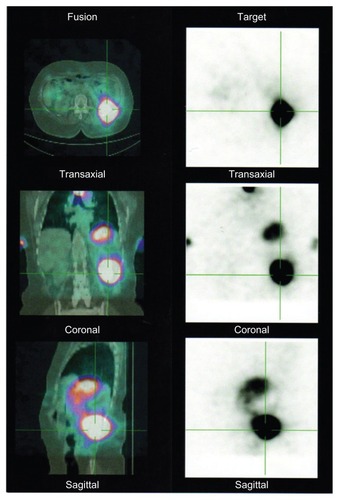
Figure 2 Preoperative 131I-WBS.
Abbreviations:131I, iodine-131; WBS, whole body scan.
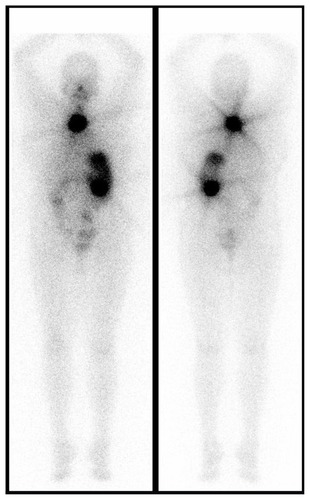
Figure 3 Surgical specimen of renal metastasis.

Results
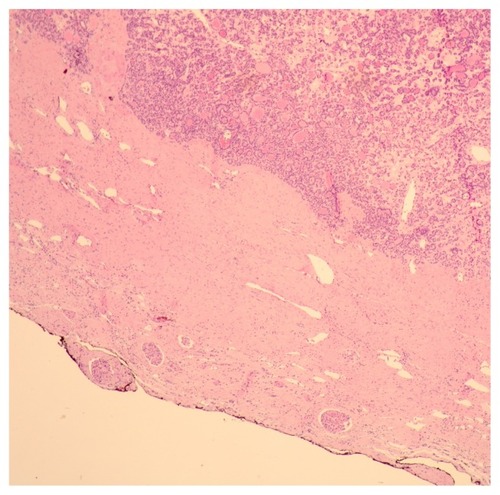
Estimated blood loss during surgery was 100 mL and the operative time was 180 minutes. The length of stay was 6 days. Serum creatinine was constantly 0.7 mg/dL and the estimated glomerular filtration rate was 88.61 mL/minute. There were no postoperative complications. Histological examination confirmed the presence of follicular thyroid cancer with negative surgical margins (). Furthermore, immunohistochemical analysis showed positive results for galectin-3, HBME1, and CK19.
Figure 4 Histological findings.
After renal enucleation and stimulation with recombinant TSH, thyroglobulin was 82 ng/mL, TSH was 15 mU/L, and antithyroglobulin antibody was negative.
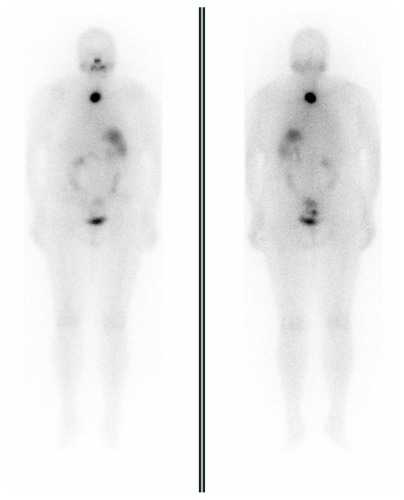
After 2 months, the patient underwent adjuvant radiometabolic treatment with 131I (150 mCi) and the following WBS showed only a small uptaking area at the level of the vertebral metastasis (). This finding proved a partial response of the bone lesions to radioiodine therapy. At 30 months, an abdominal CT scan did not detect any renal recurrence of tumor. At 36 months follow-up, the lung metastases were not detectable and the malignant disease was clinically stable and well-controlled. The clinical stage was T1bN0M1stage IVC according to the 2009 TNM classification.Citation7
Figure 5 Post-partial nephrectomy 131I-WBS.
Abbreviations:131I, iodine-131; WBS, whole body scan.
Discussion
10%–15% of patients with follicular carcinoma present with metastatic disease, most commonly involving the lung followed by bone. Brain, liver, and skin are less common sites of systemic metastases.Citation5 Renal involvement from thyroid primary cancer is very rare (4.5%–5.9%). Only 18 cases of renal metastasis from thyroid carcinoma have been reported in the English literature and over 30 cases in the Japanese literature.Citation8–Citation12
Thyroid carcinoma accounts for only 2.5%–2.7% of all primary tumors that metastasize to the kidney.Citation4 However, renal metastases are found more often at autopsy than during life. It could be related to a variable expression of sodium iodide symporter (NIS) among different metastatic sites or to the selective loss of function of the NIS.Citation13 In our case, the metastatic focus was single and unilateral, contrary to what commonly occurs: the thyroid cancer metastasizes predominantly by a hematogenous path, resulting in multiple and bilateral renal metastases. This apparent anomaly may be related to the presence of venous and/or lymphatic minor collaterals between the thyroid gland and kidney.Citation4 These metastases are often asymptomatic and their diagnosis may be delayed, especially if radiometabolic treatment is not performed or if the metastatic foci are not concentrating radioiodine. It is important to stress that a strong radiometabolic uptake in the upper abdominal tract should never be considered as a false positive or as physiological activity of the gastrointestinal tract, since biliary, gastrointestinal, and urinary radioiodine activity is much more diffuse. Therefore, any radioiodine activity detected by the radioiodine WBS should always be investigated further by anterior and posterior scans. Lateral views may also be obtained, as they could be helpful in distinguishing gastric or hepatic uptake from renal/adrenal uptake, which should be more posteriorly located. In our case, the strong uptake of radioiodine in the kidney not only allowed for the diagnosis of metastatic renal involvement, but also it significantly reduced the effectiveness of radiometabolic treatment of the secondary vertebral and lung injuries ().
Management of renal metastasis from thyroid cancer includes radical nephrectomy combined with repeated high-dose radioiodine therapies, possibly guided by whole body and blood dosimetry.Citation14–Citation17
Niederle et al reported on a total of 45 patients affected by cancer (41 follicular and 4 papillary carcinomas) that received surgical treatment for distant metastases.Citation14 Fifty-four metastatic lesions were removed, but no renal metastasis was reported. A total of 25 metastases (17 bone, eight soft tissue) were removed by resection. They reported that the estimated cumulative survival rate (Kaplan–Meier) was 44.8% ± 11.2% for 5 years and 32.7% ± 11.0% for 10 years after removal of a solitary metastasis. The study highlighted that the surgical removal of resectable metastases can be a valuable complement to nuclear medical therapy.Citation14
Wood et al found that the 5-year survival period of well-differentiated thyroid carcinoma patients with resectable metastatic lesions was 67%.Citation18
Xu et al reported a case of a 64-year-old woman with metastatic thyroid follicular carcinoma presenting as a primary renal tumor; they performed radical nephrectomy and, after 6 months, a total thyroidectomy with a lymphadenectomy.Citation8 They recommend that the treatment for well-differentiated follicular carcinoma with distant metastasis is maximal excision of the tumors followed by thyroid hormone supplementation and 131I therapy, because complete surgical excision of the distant metastatic lesion and primary tumor can still offer a good prognosis.Citation8
Kumar et al treated renal metastasis by performing only high-dose radioiodine therapy as the patient refused surgery.Citation4 When surgical excision is not possible, high-dose radioiodine therapy followed by a suppressive dose of L-thyroxine is a favorable approach because it prolongs survival by delaying disease progression.Citation4
In our opinion, surgical exeresis of renal metastasis was necessary in this case in order to improve the effectiveness of radiometabolic treatment on bone and lung metastases. Indeed, surgery allowed a debulking of the surgical removable metastases, reducing the tumor burden to be treated by radioactive iodine. Moreover, it is estimated that 131I therapy is effective in only 55% of patients with bone metastases and only 17% of them develops remission.Citation19,Citation20 Radiometabolic treatment can be curative in 35%–45% of micronodular pulmonary metastases with a reported 10-year survival rate of 90%.Citation21
Therefore, in our case, the mini-invasive surgical management of the renal metastasis increased the chance that radioiodine therapy would be effective on the vertebral and lung metastases. Moreover, surgery has an important role in the management of metastatic disease: macroscopic metastases that are isolated to lung, bone, or brain that can be resected result in improved survival.Citation5 In our case, after the combined approach with surgical removal of renal metastasis and radiometabolic treatment, the patient developed a remission of lung metastases, that were not detectable, and a stabilization of bone metastases. The WBS following adjuvant radioiodine therapy pointed out partial response of bone lesions to radiometabolic treatment with only a small uptaking area at the level of the vertebral lesions.
Despite a previous extended left hemicolectomy for colon rectal cancer, we performed a retroperitoneal laparoscopy to minimize intraoperative bleeding, to not stop bowel peristalsis, and to reduce postoperative pain. Consequently, this surgical strategy decreased the discomfort of the patient and the length of stay. We did not clamp the renal hilum to avoid damage related to ischemia of healthy renal parenchyma. As already demonstrated in the literature, the absence of intraoperative ischemia allows for better preservation of renal function in the long term.Citation22
Moreover, longer warm ischemia time during partial nephrectomy is associated with an increased risk of short and long-term renal injuries, including acute renal failure in the postoperative period and new-onset development of stage IV chronic kidney disease during follow-up.Citation23 Preservation of renal function could be useful to the following therapies. The mini-invasive surgery allowed mobilization of the patient at the first postoperative day, earlier recovery of general health, and earlier reinstatement of high-dose radioiodine treatment of the other metastases. To our knowledge, there are no studies about laparoscopic enucleation of renal metastasis from thyroid cancer. The complicated surgical treatment of metastasis is justified by the favorable effect on prognosis and the patient’s quality of life.
Conclusion
To our knowledge, this is the first case of laparoscopic extraperitoneal simple enucleation of renal metastasis from thyroid cancer. This therapeutic management preserves renal function and improves the effectiveness of the following radioiodine treatment. When thyroid carcinoma metastasizes to the kidney, minimally invasive renal enucleation associated with repeated high-dose radioiodine treatment could be a new and useful approach to delay malignant disease progression, reducing the surgical discomfort of the patient. However, further studies with larger series are needed.
Disclosure
The authors report no conflicts of interest in this work.
References
- SiegelRNaishadhamDJemalACancer statistics, 2012CA Cancer J Clin2012621102922237781
- WartofskyLIncreasing world incidence of thyroid cancer: increased detection or higher radiation exposure?Hormones (Athens)20109210310820687393
- MaxonHR3rdSmithHSRadioiodine-131 in the diagnosis and treatment of metastatic well differentiated thyroid cancerEndocrinol Metab Clin North Am19901936857182261912
- KumarANadigMPatraVSrivastavaDNVermaKBalCSAdrenal and renal metastases from follicular thyroid cancerBr J Radiol2005789351038104116249606
- McHenryCRPhitayakornRFollicular adenoma and carcinoma of the thyroid glandOncologist201116558559321482585
- ShahaARImplications of prognostic factors and risk groups in the management of differentiated thyroid cancerLaryngoscope2004114339340215091208
- SobinLHComptonCCTNM seventh edition: what’s new, what’s changed: communication from the International Union Against Cancer and the American Joint Committee on CancerCancer2010116225336533920665503
- XuHZengWTangYMetastatic thyroid follicular carcinoma presenting as a primary renal tumorIntern Med201251162193219622892502
- IwaiHOhnoYItoHKiyokawaTAokiNRenal rupture associated with a poorly differentiated follicular thyroid carcinoma metastasizing to the thigh muscle, lung and kidneyIntern Med20054484885216157985
- MoudouniSMEn-NiaIRioux-LeclerqNFollicular carcinoma of the thyroid metastasis to the kidney nine years after resection of the primary tumorAnn Urol2002363637
- LiouMJLinJDChungMHRenal metastasis from papillary thyroid microcarcinomaActa Otolaryngol200512543844415823819
- DjekidelMGordonMShahRBRenal metastasis from Hurthle cell thyroid carcinoma and its evaluation with hybrid imagingThyroid20102042943320373987
- SmallridgeRCCastroMRMorrisJCRenal metastases from papillary thyroid carcinoma: study of sodium iodide symporter expressionThyroid200111879580411525275
- NiederleBRokaRSchemperMFritschAWeisselMRamachWSurgical treatment of distant metastases in differentiated thyroid cancer: indication and resultsSurgery19861006108810973787464
- PakHSkarulisMCSchrumpDAlexanderHRLibuttiSKSarlisNJThe role of extensive metastatectomy in the long term management of clinically aggressive thyroid carcinomaThe NIH experienceProceedings of the 11th International Congress of Endocrinology2000Sydney, AustraliaP803 [Abstract].
- ReynoldsJCRobbinsJThe changing role of radioiodine in the management of differentiated thyroid cancerSemin Nucl Med19972721521649144857
- MaxonHRQuantitative radioiodine therapy in the treatment of differentiated thyroid cancerQ J Nucl Med199943431332310731782
- WoodWJSingletarySEHickeyRCCurrent result of treatment for distant metastatic well-differentiated thyroid carcinomaArch Surg1989124137413772589960
- DuranteCHaddyNBaudinELong-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapyJ Clin Endocrinol Metab20069182892289916684830
- ProyeCADromerDHCarnailleBMIs it still worthwhile to treat bone metastases from differentiated thyroid carcinoma with radioactive iodine?World J Surg19921646406451384244
- SchlumbergerMTubianaMDe VathaireFLong-term results of treatment of 283 patients with lung and bone metastases from differentiated thyroid carcinomaJ Clin Endocrinol Metab1986639609673745409
- AronMGillISCampbellSCA nonischemic approach to partial nephrectomy is optimal. YesJ Urol2012187238738822177156
- ThompsonRHLaneBRLohseCMEvery minute counts when the renal hilum is clamped during partial nephrectomyEur Urol201058334034520825756