Abstract
Development of nonantibiotic-associated pseudomembranous colitis has been reported in patients receiving chemotherapy. Herein, we report a case of a 70-year-old man with diabetes mellitus and hypertension who received concurrent chemoradiation therapy after surgery for stage III pT3N1M0 rectal cancer. After completion of the therapy, the patient presented with a 2-week history of intermittent watery diarrhea (seven to nine times per day). However, the patient was afebrile and laboratory examination revealed no evidence of leukocytosis. Computed tomography disclosed inflammation of the sigmoid colon, infiltrative changes around the anastomotic site, and edematous changes straddling the serosal surface. Colonoscopic examination revealed multiple whitish patches within the radiation field, a finding suggestive of pseudomembranous colitis. No concomitant antibiotics were used during the period of concurrent chemoradiation therapy. Empirical oral metronidazole (500 mg every 8 hours) was administrated for 2 weeks. At the end of this treatment, stool culture was negative for Clostridium difficile. Physicians should be aware of the potential for the development of pseudomembranous colitis following concurrent chemoradiation therapy.
Introduction
Clostridium difficile, a Gram-positive anaerobic bacillus,Citation1 and its toxin can cause antibiotic-associated pseudomembranous colitis, a superficial necrosis of the colonic mucosa with an accompanying “pseudomembrane” (exudative plaque).Citation2 However, pseudomembranous colitis due to C. difficile has also been diagnosed in patients who have not been exposed to antibiotic therapy, particularly in patients of older age, with diabetes mellitus (DM), renal failure, or intestinal obstruction, and those who have had intestinal surgery.Citation3,Citation4 Pseudomembranous colitis has also been reported in cancer patients after receiving antineoplastic chemotherapy without antibiotics.Citation5
Herein, we report a case of nonantibiotic-associated pseudomembranous colitis that developed within the radiation field after postoperative concurrent chemoradiation therapy (CCRT) for rectal cancer in a patient with underlying DM. The investigation was reviewed and approved by the Institutional Review Board of the Far Eastern Memorial Hospital, Taipei, Taiwan.
Case report
A 70-year-old man with a history of DM and hypertension presented with stage III pT3N1M0 rectal cancer. A lower-anterior gross adeno-carcinoma resection was performed and adjuvant concurrent chemoradiation therapy undertaken from March 2010 to mid-April 2010. Image-guided intensity-modulated radiotherapy was delivered to the surgical bed and pelvic nodal areas simultaneously at 54 Gy and 50 Gy, respectively, in 27 fractions over 6 weeks. The chemotherapy regimens included weekly bolus 5-fluorouracil (450 mg/m2) and leucovorin (30 mg/m2). No concomitant antibiotics were used during the CCRT period.
After CCRT, the patient presented with a 2-week history of intermittent watery diarrhea (seven to nine times per day); however, he was afebrile and laboratory examination revealed no evidence of leukocytosis. Stool sample analysis revealed the presence of occult blood but no evidence of pus cells. Computed tomography (CT) disclosed inflammation of the sigmoid colon, infiltrative changes around the anastomotic site, and edematous changes straddling the serosal surface within the radiation field (). Colonoscopic examination revealed multiple white and yellow pseudomembranes on the wall of the rectum, as well as swelling, suggesting pseudomembranous colitis (). Histopathologic analysis of the biopsy specimens revealed partial or full thickness necrosis of the mucosa, glandular hypersecretion, and pseudomembranes composed of fibrin, mucus, and inflammatory cells with Gram-positive anaerobic bacillus, findings suggestive of pseudomembranous colitis (). Anti-motility medication and empirical oral metronidazole (500 mg every 8 hours) were administered for 1 week as treatment for infectious diarrhea prior to stool testing. A stool sample was taken after antibiotic therapy and the results of the stool culture were negative for C. difficile. His symptoms subsided gradually and the number of yellow pseudomembranes decreased (). At 3-month follow-up, the patient was symptom free and abdominal CT revealed mild inflammatory changes around the anastomotic site ().
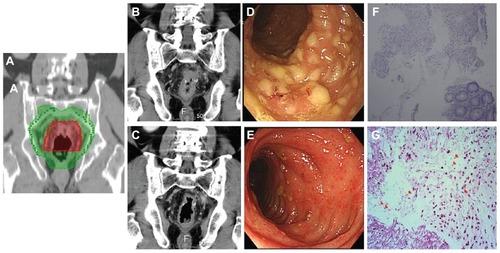
Figure 1 (A) The irradiation fields in radiation plan. Fifty-four Gray (Gy) and 50 Gy was delivered in red and green area, respectively. (B) The first evaluative CT scans after concurrent chemoradiation therapy. Inflammation of the sigmoid colon showing infiltrative changes around the site of anastomosis, edematous changes on the serosal surface, and marked thickening of the colonic wall. (C) The second evaluative CT performed at 3-month follow-up reveals mild inflammatory changes around the anastomotic site. (D) Endoscopic examination showed multiple white and yellow pseudomembranes on the wall of the rectum, as well as swelling, suggesting pseudomembranous colitis. (E) After a 2-week course of antibiotics, the number of pseudomembranes decreased and the severity of diarrhea gradually improved. (F) Histolopathologic analysis revealed partial or full thickness necrosis of the mucosa, glandular hypersecretion, and pseudomembranes composed of fibrin, mucus, and inflammatory cells (hematoxylin and eosin stain, ×100), findings suggestive of pseudomembranous colitis. (G) Gram-positive bacilli were identified in the suppurative exudate over the colonic mucosa (red arrows, Gram stain, ×400).
Discussion
C. difficile and its toxins are the most common causes of pseudomembranous colitis.Citation6 Although disruption of the normal bowel flora due to antibiotic exposure is most often the cause of inflammation caused by C. difficile and its toxins, studies have shown that surgery following chemotherapyCitation7 or chemotherapeutic agentsCitation5 can also cause extensive intestinal inflammatory changes by altering the normal bowel flora, leading to the growth of C. difficile and production of its toxins in the absence of antibiotic therapy.
However, to the best of our knowledge, the development of pseudomembranous colitis in the radiation field after CCRT in patients who have not been exposed to antibiotics has never been reported. Hautmann et al noted that radio-oncological patients were also patients at risk of C. difficile infection and that the incidence was 1.6%, especially for head and neck cancer patients.Citation8 Prendergast et al reported that irradiation-associated reductions in normal beef surface flora influenced survival of nonpathogenic Escherichia coli and pathogenic E. coli, suggesting that irradiation may affect the chemical or physical composition of flora.Citation9 In addition, Rowe et al reported that free radical-induced oxidation of proteins and lipids may contribute to bacterial survival.Citation10 This suggests that normal gastrointestinal flora may also be altered by irradiation.Citation10
Development of pseudomembranous colitis has also been reported in patients of advanced age with DM after intestinal surgery in the absence of antibiotic treatment.Citation3,Citation4 One possible reason for changes in the normal flora in patients with diabetes is that diabetes results in decreased numbers of normal inhibitory bacteria in the oropharynx.Citation11 Moreover, pseudomembranous colitis is also associated with high mortality and has a high rate of recurrence, especially in older and debilitated persons.Citation12 In our patient, who had DM and had had intestinal surgery followed by CCRT, the CT () and colonoscopic findings () correlated with the radiotherapy target volume (), indicating that the pseudomembranous colitis within the radiation field after CCRT was caused by the synchronous effects of radiation therapy and chemotherapy.
The patient was prescribed oral metronidazole according to the CT scan (), pathologic (), and colonoscopic findings () – initially without stool culture. C. difficile colitis may be diagnosed by sigmoidoscopy and/or stool tests.Citation13 Bergstein et alCitation14 reported that patients underwent lower gastrointestinal endoscopy with endoscopic confirmation of pseudomembranes but four (14%) had only nonspecific colitis. Following pathologic and imaging findings for C. difficile colitis similar to our own, Kelly et al also reported a characteristic diagnosis.Citation15 Oral metronidazole and vancomycin are equally effective in treating diarrhea caused by C. difficile infection.Citation16 After receiving metronidazole, our patient’s diarrhea improved and CT () and colonoscopy () images showed recovery. However, stool tests are still the most sensitive and specific for diagnosis of C. difficile infection.Citation17,Citation18 Therefore, we suggest that even when images and pathologic reports confirm pseudomembranous colitis, a stool test should be performed before treatment to confirm which antibiotics to administer.
Conclusion
Elderly patients with DM who require CCRT after intestinal surgery are at risk of developing pseudomembranous colitis, especially if all three of these factors exist simultaneously. Stool tests should be routinely performed to establish whether there is pseudomembranous colitis, so that the appropriate antibiotics can be administered.
Acknowledgment
This study was supported by a grant from the Far Eastern Memorial Hospital (FEMH-2012-C-055).
Disclosure
The authors report no conflicts of interest in this work. Written informed consent was obtained from the patient to publish data and figures from his medical file.
References
- HallICO’TooleEIntestinal flora in new-born infants with a description of a new pathogenic anaerobe, Bacillus difficilisArch Pediatr Adolesc Med1935492390402
- BartlettJGChangTTaylorNSOnderdonkABColitis induced by Clostridium difficileRev Infect Dis197912370378549188
- MoskovitzMBartlettJGRecurrent pseudomembranous colitis unassociated with prior antibiotic therapyArch Intern Med198114156636647224749
- DosikGMLunaMValdiviesoMNecrotizing colitis in patients with cancerAm J Med1979674646656495635
- AnandAGlattAEClostridium difficile infection associated with antineoplastic chemotherapy: a reviewClin Infect Dis19931711091138353229
- BartlettJGChangTWGurwithMGorbachSLOnderdonkABAntibiotic-associated pseudomembranous colitis due to toxin-producing clostridiaN Engl J Med197829810531534625309
- Morales ChamorroRSerrano BlanchRMéndez VidalMJPseudomembranous colitis associated with chemotherapy with 5-fluorouracilClin Transl Oncol20057625826116131450
- HautmannMGHippMKölblOClostridium difficile-associated diarrhea in radiooncology: an underestimated problem for the feasibility of the radiooncological treatment?Radiat Oncol201168921806799
- PrendergastDMCrowleyKMMcDowellDASheridanJJSurvival of Escherichia coli O157:H7 and non-pathogenic E. coli on irradiated and non-irradiated beef surfacesMeat Sci200983346847320416678
- RoweLJMaddockKRLonerganSMHuff-LonerganEInfluence of early postmortem protein oxidation on beef qualityJ Anim Sci200482378579315032435
- MackowiakPAMartinRMSmithJWThe role of bacterial interference in the increased prevalence of oropharyngeal gram-negative bacilli among alcoholics and diabeticsAm Rev Respir Dis1979120358959339482
- MoshkowitzMBen-BaruchEKlineZShimoniZNivenMKonikoffFRisk factors for severity and relapse of pseudomembranous colitis in an elderly populationColorectal Dis20079217317717223943
- FeketyRShahABDiagnosis and treatment of Clostridium difficile colitisJAMA1993269171758416409
- BergsteinJMKramerAWittmanDHAprahamianCQuebbemanEJPseudomembranous colitis: how useful is endoscopy?Surg Endosc1990442172192291163
- KellyCPPothoulakisCLaMontJTClostridium difficile colitisN Engl J Med199433042572628043060
- TeasleyDGGerdingDNOlsonMMProspective randomised trial of metronidazole versus vancomycin for Clostridium-difficile-associated diarrhoea and colitisLancet198328358104310466138597
- De GirolamiPCHanffPAEichelbergerKMulticenter evaluation of a new enzyme immunoassay for detection of Clostridium difficile enterotoxin AJ Clin Microbiol1992305108510881583104
- DoernGVCoughlinRTWuLLaboratory diagnosis of Clostridium difficile-associated gastrointestinal disease: comparison of a monoclonal antibody enzyme immunoassay for toxins A and B with a monoclonal antibody enzyme immunoassay for toxin A only and two cytotoxicity assaysJ Clin Microbiol1992308204220461500512