Abstract
The expansion in understanding the molecular biology that characterizes cancer cells has led to the rapid development of new agents to target important molecular pathways associated with aberrant activation or suppression of cellular signal transduction pathways involved in gliomagenesis, including epidermal growth factor receptor, vascular endothelial growth factor receptor, mammalian target of rapamycin, and integrins signaling pathways. The use of antiangiogenic agent bevacizumab, epidermal growth factor receptor tyrosine kinase inhibitors gefitinib and erlotinib, mammalian target of rapamycin inhibitors temsirolimus and everolimus, and integrin inhibitor cilengitide, in combination with radiation therapy, has been supported by encouraging preclinical data, resulting in a rapid translation into clinical trials. Currently, the majority of published clinical studies on the use of these agents in combination with radiation and cytotoxic therapies have shown only modest survival benefits at best. Tumor heterogeneity and genetic instability may, at least in part, explain the poor results observed with a single-target approach. Much remains to be learned regarding the optimal combination of targeted agents with conventional chemoradiation, including the use of multipathways-targeted therapies, the selection of patients who may benefit from combined treatments based on molecular biomarkers, and the verification of effective blockade of signaling pathways.
Introduction
Glioblastoma (GBM) is the most common malignant primary brain tumor in adults, with an incidence of approximately 2.8 cases per 100,000 person-years.Citation1 The current standard of care consists of surgical resection followed by radiotherapy (RT), with concomitant and adjuvant chemotherapy using the alkylating agent temozolomide (TMZ); however, the prognosis remains poor with a reported median and 2-year survival rates of 14.6 months and 26.5%, respectively.Citation2
To improve survival, several targeted agents used alone or in combination with RT and/or cytotoxic chemotherapy have been explored as potential inhibitors of the molecular and signal transduction pathways involved in gliomagenesis. Novel therapeutic strategies against newly diagnosed or progressive GBM include tyrosine kinases inhibitors (TKIs) and monoclonal antibodies directed against the epidermal growth factor receptor (EGFR), the vascular endothelial growth factor receptor (VEGFR), the platelet growth factor receptor (PDGFR), inhibitors of mammalian target of rapamycin (mTOR), and integrins molecular pathways.Citation3–Citation14
Bevacizumab (Avastin®; Genentech, Inc, San Francisco, CA, USA), a humanized murine monoclonal antibody directed against vascular endothelial growth factor (VEGF), has received accelerated approval for the treatment of recurrent GBM in 2009 by the US Food and Drug Administration (FDA); however, most of the prospective studies on the use of targeted drugs as single agent for progressive disease have not shown improved clinical outcomes.Citation15 Emerging data show that aberrant expression of a variety of cell and molecular pathways may influence radiation resistance, including growth factor receptor signaling pathways, deoxyribonucleic acid (DNA) damage repair processes, and angiogenesis (). So far, the combination of RT with simultaneous administration of targeted agents that inhibit molecular pathways involved in tumor growth and progression may represent an attractive strategy against cancer. While this multimodal treatment has shown promising results for different solid cancers – including head and neck, as well as non-small-cell lung cancer (NSCLC)Citation16,Citation17 – only limited data are available on the combinations of targeted drugs and RT for GBMs. In this review, we will provide an overview of published studies as well as ongoing trials evaluating the efficacy of targeted therapies in combination with cytotoxic chemotherapy and/or RT for the treatment of newly diagnosed and recurrent GBM.
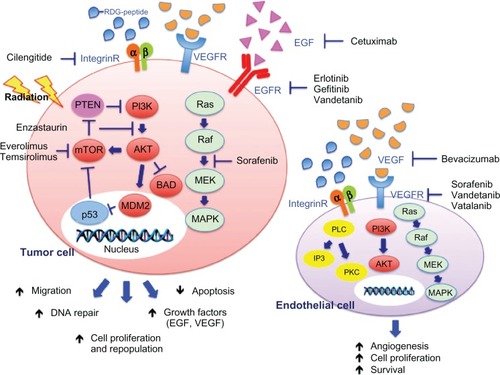
Figure 1 Schematic representation of the effects of radiation and targeted agents on EGFR, VEGFR, and integrin-signaling pathways.
Abbreviations: EGFR, epidermal growth factor receptor; VEGFR, vascular endothelial growth factor receptor; RDG-peptide, Arg-Gly-Asp peptide; EGF, epidermal growth factor; VEGF, vascular endothelial growth factor; integrin-R, integrin receptor; PTEN, phosphatase and tensin homologue; PI3K, phosphoinositide 3-kinase; Ras, Ras GTPase; mTOR, mammalian target of rapamycin; AKT, protein kinase B; Raf, rapidly accelerated fibrosarcoma; p53, tumor protein 53; MDM2, mouse double minute 2 homologue; BAD, Bcl-2-associated death promoter; MEK, mitogen-activated protein kinase kinase; MAPK, mitogen-activated protein kinase; PLC, phospholipase C; IP3, inositol trisphosphate; PKC, protein kinase C; DNA, deoxyribonucleic acid.
Combinations of VEGF inhibitors with radiation
Angiogenesis and its major regulator, VEGF, represent one of the most important therapeutic targets in GBM treatment, and the interaction between VEGFR-signaling pathways and RT has been investigated in in vitro and in vivo studies.Citation18–Citation23 Upregulation of VEGF expression has been observed in either irradiated GBM cell lines or xenografts,Citation21,Citation23 and its overexpression correlates with poor prognosis.Citation24 Several tumor cell lines, including U251, U251-NG2, and U87 human GBM cells showed a dose-dependent increase in VEGF levels after single doses of radiation, leading to tumor cell invasion and migration through activation of proto-oncogene tyrosine–protein kinase Src, and focal adhesion kinase. In addition, radiation-induced VEGF secretion may contribute to the high radioresistance of GBM through the reduction of the damaging effect of RT on endothelial cells and increased tumor hypoxia.Citation18,Citation20 Several VEGF/VEGFR inhibitors have been recently developed, including bevacizumab, vatalanib (PTK787/ZK222584; Bayer Schering Pharma AG, Berlin, Germany; Novartis Corporation, East Hanover, NJ, USA), cediranib (Recentin™; AstraZeneca Pharmaceuticals, London, UK), sunitinib (Sutent®; Pfizer, Inc, New York, NY, USA), sorafenib (Nexavar®, Bayer HealthCare Pharmaceuticals, Inc, Wayne, NJ, USA), vandetanib (Caprelsa®; AstraZeneca Pharmaceuticals), and aflibercept (VEGF-Trap; Regeneron Pharmaceuticals, Inc, Tarrytown, NY, USA; Sanofi-Aventis, Paris, France). Clinical studies so far are testing the efficacy of combining VEGFR antagonists with RT, with the potential to improve outcomes by blocking the effects of radiation-induced VEGF expression and by improving tumor oxygenation through vascular normalization.
Bevacizumab
Bevacizumab is a recombinant humanized monoclonal antibody that inhibits tumor angiogenesis by targeting soluble VEGF-A and preventing its interaction with VEGF receptors.Citation25 The antiangiogenic activity of bevacizumab has been demonstrated in several preclinical cancer models.Citation26 Inhibition of angiogenesis may be exerted through different mechanisms, including regression of existing tumor vasculature, normalization of surviving vasculature, and inhibition of new and recurrent tumor vessel growth.Citation27–Citation29 Bevacizumab has been approved in combination with chemotherapy for use in metastatic colorectal cancer, advanced NSCLC, and advanced and/or metastatic renal cell cancer.Citation30–Citation32 Based on the results of two prospective trials,Citation33,Citation34 bevacizumab received US FDA accelerated approval as a single-agent for the treatment of recurrent GBM in May 2009.
Preclinical studies have demonstrated that blocking the VEGF pathway with bevacizumab can enhance the sensitivity of both tumor and endothelial cells to the cytotoxic effects of radiation.Citation35,Citation36 In tumor xenograft models, the administration of bevacizumab in combination with RT induces inhibition of tumor growth with an additive effect compared to treatment with bevacizumab or radiation alone.Citation36,Citation37 The main mechanism by which bevacizumab can enhance the radiation response is by increasing tumor oxygenation through vascular normalization and by improving intratumoral perfusion, as shown in GBM cell lines and in orthotopic U87 GBM xenografts.Citation37–Citation39 Interestingly, vascular normalization with improved tumor perfusion and oxygenation was observed only from days 2 to 5 from the start of treatment. Consistent with these findings, the cytotoxic effect of radiation was strongest when RT was delivered within this time interval.
The potential synergistic activity of bevacizumab with RT has been tested in several Phase I and Phase II trials of either newly diagnosed or recurrent gliomas (). Narayana et alCitation40 have assessed the combination of bevacizumab with standard RT and TMZ in a small series of 15 patients with newly diagnosed high-grade gliomas treated at the New York University Medical Center. Bevacizumab was administered intravenously at 10 mg/kg on days 14 and 28 of RT, followed by twelve cycles of adjuvant TMZ and bevacizumab 10 mg/kg every 14 days. At a median follow-up of 12 months, the 1-year progression-free survival and overall survival rates were 59% and 86%, respectively. Grade 3–4 toxicities occurred in seven patients and included thromboembolism, multiple nonhealing ulcers, malignant hypertension, and thrombocytopenia/neutropenia. Following these promising results, a further 51 patients with newly diagnosed GBM were treated at the same institution using the same regimen.Citation41 The 6-month and 12-month progression-free survival rates were 85% and 51%, respectively, and the respective overall survival rates were 85% and 42%. Grade 3 or grade 4 toxicities (thrombocytopenia, deep vein thrombosis, pulmonary embolism, nausea, and fatigue) occurred in 19% of patients, and asymptomatic intracranial bleeding occurred in 10% of patients.
Table 1 Clinical trials of antiangiogenic agents and integrin inhibitors in combination with radiotherapy
Several other prospective studies have assessed the clinical outcomes and toxicity of bevacizumab in association with standard chemoradiation.Citation10,Citation11,Citation42–Citation44 Lai et alCitation11 reported a Phase II study of 70 patients treated with bevacizumab plus TMZ during and after RT until tumor progression, or for a maximum of 24 TMZ cycles. Median overall survival and progression-free survival rates were 19.6 months and 13.6 months, respectively, as compared with survivals of 21.1 months and 7.6 months, respectively, in a control cohort of 110 patients treated with standard treatment at University of California and Kaiser Permanente Los Angeles, indicating that treatment with bevacizumab and TMZ was associated with improved progression-free survival without improved overall survival. The most common nonhematologic treatment-related toxicities were represented by fatigue, venous thrombosis, hypertension, and proteinuria. Presumed toxicities related to bevacizumab included cerebrovascular ischemia in six patients, wound infections in four patients, gastrointestinal perforations in two patients, gastrointestinal bleeding in two patients, and cerebral hemorrhage in two patients.
Vredenburgh et alCitation10 reported on 75 patients with newly diagnosed GBM treated at Duke University with bevacizumab with concomitant RT and TMZ followed by adjuvant bevacizumab, TMZ, and irinotecan. Bevacizumab was administered during RT every 14 days at a dose of 10 mg/kg. Two weeks after completion of chemoradiation, therapy was continued with 6–12 cycles of TMZ, bevacizumab at a dose of 10 mg/kg every 14 days, and irinotecan every 14 days at a dose of 125 mg/m2 for patients not on enzyme-inducing antiepileptic drugs (EIAEDs), and 340 mg/m2 for patients on EIAEDs. At a median follow-up of 23.1 months, median overall survival and progression-free survival rates were 21.2 months and 14.2 months, respectively. Discontinuation of therapy due to treatment-related toxicity occurred in 4% of patients during RT and in 23% of patients during adjuvant chemotherapy. Two patients died, one from neutropenic sepsis and one from pulmonary embolism. Results of the addition of bevacizumab to standard RT and daily TMZ in 125 patients with newly diagnosed GBM have been reported by the same group.Citation43 With a median follow-up of 21 months, the median and 6-month progression-free survival rates were 13.8 months and 87.2%, respectively. RT was discontinued in five patients due to pulmonary embolism in two patients, grade 4 pancytopenia in one patient, grade 2 cerebral hemorrhage in one patient, and wound dehiscence in one patient. Grade 4 thrombocytopenia/neutropenia occurred in four patients, and nonhematologic toxicities occurred in a further four patients (two generalized seizures, one pneumocystis carinii pneumonia, and one bowel perforation).
Hainsworth et alCitation44 evaluated the efficacy and safety of the combination of standard RT and TMZ with bevacizumab followed by maintenance therapy with bevacizumab and the mTOR inhibitor, everolimus, in 68 patients with newly diagnosed GBM. The treatment was well tolerated, although median progression-free survival and overall survival rates were 11.3 months and 13.9 months, respectively, which were similar to those reported with standard chemoradiation.Citation2
More recently, preliminary results of a Phase III, randomized, double blind, placebo-controlled trial that assessed the efficacy and safety profile of bevacizumab in combination with RT and TMZ chemotherapy following surgery or biopsy in patients with newly diagnosed GBM (the AVAglio study) have been reported.Citation45 Patients were randomized to receive: bevacizumab plus RT and TMZ chemotherapy, followed by bevacizumab and TMZ for up to six cycles, followed by bevacizumab alone until disease progression; or RT, TMZ, and placebo for 6 weeks, followed by TMZ and placebo for up to six cycles, followed by placebo until disease progression. Primary endpoints were progression-free survival and overall survival. A 4.4-month improvement in median progression-free survival was observed in patients who received bevacizumab in combination with RT and TMZ compared to those who received radiation and TMZ plus placebo (10.6 months versus 6.2 months, respectively, P < 0.0001). However, interim results for overall survival did not reach statistical significance (hazard ratio = 0.89; P = 0.2135). The 1-year survival rates were 66% for the placebo arm versus 72% in the bevacizumab arm (P = 0.052). Final data on overall survival are expected by the end of 2013. An important finding of the study was that bevacizumab in combination with standard chemoradiation significantly improved the duration of functional independence and a number of selected health-related quality of life domains, and significantly decreased corticosteroid doses.
The clinical activity of bevacizumab with RT in the retreatment setting has been evaluated in a few studies.Citation46–Citation49 Gutin et alCitation46 reported on 24 patients with recurrent high-grade glioma treated with hypofractionated stereotactic RT (30 Gy in five fractions over 2.5 weeks) and bevacizumab administered at a dose of 10 mg/kg every 14 days of 28-day cycles until tumor progression. The median progression-free survival and overall survival rates were 7.3 months and 12.5 months for patients with GBM, and 7.5 months and 16.5 months for patients with grade 3 glioma, respectively. Severe treatment-related toxicity occurred in three patients and included central nervous system intratumoral hemorrhage, bowel perforation, and wound dehiscence. Similar encouraging data were reported in a retrospective analysis by Niyazi et alCitation48 in 30 patients with recurrent high-grade glioma treated with fractionated stereotactic RT (36 Gy in 18 fractions) alone or in combination with bevacizumab (10 mg/kg on days 1 and 15 during RT). The addition of bevacizumab to reirradiation resulted in significant improvement of overall survival (367.6 days versus 187.4 days) and progression-free survival (244 days versus 143 days), as compared with reirradiation alone. Toxicity included one grade 3 deep vein thrombosis, one grade 4 wound healing complication, and two cases of radiation necrosis. Overall, the results of these studies suggest that reirradiation in combination with bevacizumab is a feasible and well tolerated treatment in selected patients with recurrent GBM, although survival benefits are modest.
Vandetanib
Vandetanib is an oral anilinoquinazoline compound with a low molecular weight that acts as a potent multitargeted inhibitor of VEGFR-2,Citation50 EGFR, and the REarranged during Transfection (RET) tyrosine kinases.Citation51,Citation52 Therefore, by simultaneous inhibition of both VEGFR and EGFR pathways, vandetanib may exhibit antitumor activity through blockade of multiple mechanisms that are essentials for tumor angiogenesis and proliferation. Several clinical trials evaluated vandetanib as a single agent or in combination with chemotherapy in solid tumors, although with modest survival benefit.Citation53–Citation56 Currently, vandetanib has been approved by the US FDA for the treatment of unresectable locally advanced or metastatic medullary thyroid cancer.Citation57
Preclinical studies have shown that vandetanib combined with radiation inhibits tumor growth in a dose-dependent manner. The mechanism by which the inhibition of VEGFR-2 may potentiate the cytotoxic effect of ionizing radiation is by reducing tumor hypoxia through vascular normalization,Citation35 and through decreasing tumor cell oxygen consumption,Citation58 as demonstrated in either human GBM cell lines or nude mice xenografts,Citation59 as well as in orthotopic rat glioma models.Citation60 The optimal timing of the administration of vandetanib with RT has not yet been established, as enhanced inhibition of tumor growth has been shown in different tumor models with both concurrentCitation61 and sequentialCitation62 combined treatment, as well as irrespective of sequencing of both agents.Citation63,Citation64
Based on this preclinical evidence, few Phase I studies have investigated the combination of vandetanib with RT in both newly diagnosed and recurrent gliomas (). Drappatz et alCitation65 enrolled 13 patients with newly diagnosed GBM into a Phase I trial testing the combination of vandetanib with standard RT and TMZ. In the initial cohort, six patients were treated with vandetanib at 200 mg/day. Three patients developed dose-limiting toxicities (DLTs), including one patient with grade 5 gastrointestinal hemorrhage and grade 4 thrombocytopenia, one patient with grade 4 neutropenia, and one patient with grade 4 diverticulitis with gastrointestinal perforation. Grade 3 rash and grade 3 diarrhea occurred in two patients requiring dose reduction. No DLTs were observed in seven patients treated at the lower dose of 100 mg/day, establishing this dose as the maximum-tolerated dose (MTD). Of the ten patients evaluable for tumor response, nine had stable disease (90%) and one had progressive disease (10%). The median overall survival and progression-free survival rates were 11 months and 8 months, respectively. Fields et alCitation8 reported results of a Phase I dose-escalation study for patients with recurrent high-grade glioma treated with fractionated stereotactic radiosurgery (36 Gy in three fractions) and vandetanib given at a dose of 100 mg or 200 mg daily during radiation and thereafter, until a DLT occurred or until disease progression. Of the ten patients evaluable for toxicity, DLTs were observed in one patient receiving vandetanib at a dose of 100 mg daily and in two patients receiving 200 mg daily. At a median follow-up time of 4 months, the median overall survival and progression-free survival rates were 6 months and 3 months, respectively.
The combination of vandetanib with RT was also addressed in children with newly diagnosed diffuse intrinsic pontine gliomas.Citation66 In a Phase I study, vandetanib was administered daily from the first day of RT and continued for up to 2 years. The initial dosage was 50 mg/m2 and subsequent dose levels were 65 mg/m2, 85 mg/m2, 110 mg/m2, and 145 mg/m2 per day. Of the 21 patients evaluated, grade 3 toxicity (diarrhea) was observed in one patient at the dose of 145 mg/m2. Therefore, an expanded cohort of 14 patients was treated at 110 mg/m2 (n = 10) and 145 mg/m2 (n = 4). Two of ten patients treated with 145 mg/m2 developed grade 4 hypertension and posterior reversible encephalopathy syndrome; therefore, the recommended Phase II dose of vandetanib in children was 145 mg/m2 per day. The 1-year and 2-year overall survival rates for all patients were 37.5% and 21.4%, respectively, with only three patients who remained alive and free of disease progression for more than 2 years.
Vatalanib
Vatalanib is an anilino phthalazine compound that displays submicromolar antagonistic activity against all three isoforms of VEGFR, with a higher affinity toward VEGFR-2. In addition, vatalanib selectively inhibits the PDGFR-β and c-kit at higher concentrations,Citation67 resulting in an additive antitumor effect.Citation68,Citation69 The addition of vatalanib to radiation resulted in significantly greater tumor control than either RT or vatalanib treatment alone in either GBM cell lines or tumor xenografts in a dose-dependent manner.Citation70–Citation72
Vatalanib combined with RT in newly diagnosed GBM has been evaluated in two Phase I trials (). The European Organization for Research and Treatment of Cancer performed a Phase I/II trial in 19 patients with newly diagnosed GBM treated with vatalanib combined with standard RT and TMZ.Citation73 The starting dose of vatalanib was 500 mg from the first day of RT and subsequent dose levels were 1,000 mg and 1,250 mg. During adjuvant TMZ therapy, the drug was administered at a dose of 750 mg twice daily until disease progression. No DLTs were observed in the 500 mg arm, while grade 3 hyponatremia (n = 1) and grade 3 liver dysfunction (n = 1) were observed in the 1,000 mg group, and grade 3 diarrhea (n = 1), grade 3 liver transaminases increases (n = 2), and grade 4 thrombocytopenia and/or neutropenia were observed in the 1,250 mg group. Daily vatalanib at 1,000 mg was the recommended dose for the Phase II study. Despite a promising median progression-free survival and overall survival rates of 6.8 months and 17.3 months, the planned randomized Phase II trial was discontinued right at its onset due to the decision of the industry to discontinue the drug, mainly due to the disappointing results from two Phase III trials in patients with metastatic colorectal cancer.Citation74,Citation75 In another Phase I study, 19 patients with newly diagnosed GBM received vatalanib combined with standard RT, TMZ, and an EIAED.Citation9 Seven patients were treated with vatalanib 250 mg daily, six patients with 250 mg twice daily, and six patients with 500 mg twice daily. Thereafter, during adjuvant chemotherapy patients received a dose of 750 mg of vatalanib twice daily, until tumor progression, patient withdrawal, or unacceptable toxicity. Only two DLTs were reported, including thrombocytopenia in one patient at 250 mg daily and elevated transaminases in one patient at 500 mg twice daily. Other grade 3/4 adverse events included elevated liver transaminases, leukopenia, neutropenia, lymphopenia, and hand–foot syndrome, all in one patient. Of the 13 patients evaluable for a radiographic response, two had a partial response and nine had stable disease. At a median follow-up of 14.9 months, the median progression-free survival and overall survival rates were 7.2 months and 16.2 months, respectively.
Sorafenib
Sorafenib is a small-molecule TKI that blocks phosphorylation of VEGFR, PDGFR, c-kit, and Raf serine kinase by competing with adenosine triphosphate (ATP) for the ATP-binding site.Citation76 Thus, sorafenib prevents the activation of the intracellular signaling pathways, which leads to angiogenesis and induces apoptosis in several tumor cell lines.Citation77 Sorafenib has been approved by the US FDA for the treatment of advanced unresectable hepatocellular carcinoma,Citation78 as well as for advanced renal cell cancer.Citation79
In vitro, sorafenib displays antitumor activity in a dose-dependent manner by inhibition of proliferation, and induction of apoptosis and autophagy in several glioma cell lines,Citation80,Citation81 with selective action on cancer stem cells.Citation82 In orthotopic GBM xenografts, treatment with sorafenib suppresses tumor growth and angiogenesis, and induces tumor cell apoptosis.Citation80 More recently, it has been shown that a combination of sorafenib, TMZ, and irradiation significantly reduces cell viability of human GBM cell lines with a methylated O-6-methylguanine-DNA methyltransferase (MGMT) promoter.Citation83 Based on these preclinical data, a Phase I dose escalation trial was conducted to evaluate the safety and efficacy of sorafenib in combination with TMZ and standard RT in patients with newly diagnosed high-grade gliomas, or in combination with hypofractionated stereotactic RT alone (35 Gy in ten fractions) in patients with recurrent high-grade gliomas ().Citation83 Sorafenib was administered orally from the night before the first day of RT, with escalation of dosing from 200 mg twice daily to 400 mg twice daily. Treatment with sorafenib was continued for an additional 30 days after completion of RT at the physician’s discretion. The most common grade 3 and 4 toxicities were hematologic (lymphopenia thromboctopenia, anemia) fatigue, and rash, and required discontinuation of treatment with sorafenib in 22% of patients in the 200 mg arm and in 55% of patients in the 400 mg arm. The recommended MTD and Phase II dose of sorafenib was 200 mg twice daily when combined with TMZ and RT, and 400 mg twice daily with RT alone. The median survival time was 18 months for all 18 patients, being 18 months for patients with newly diagnosed gliomas, and 24 months for those with recurrent high-grade gliomas.
Enzastaurin
Protein kinase C (PKC) is a family of at least twelve isoforms of serine–threonine kinases, which play a central role in regulating cell proliferation, differentiation, apoptosis, and secretion.Citation84,Citation85 Increased PKC expression and/or activation have been observed in several tumors.Citation86 Among the PKC family members, PKC beta (PKC-β) is a key mediator of the VEGFR-signaling pathway that is specifically involved in tumor-induced angiogenesis and endothelial cell proliferation.Citation87,Citation88 Enzastaurin (LY317615; Eli Lilly and Company, Indianapolis, IN, USA) is an acyclic bisindolylmaleimide that selectively blocks the activation of the PKC-β at low nanomolar concentrations and suppresses VEGF expression in human tumor xenografts.Citation89,Citation90 In addition to its antiangiogenic activity, enzastaurin has also direct proapoptotic and antiproliferative effects through inhibition of the phosphatidylinositol 3-kinase (PI3K/Akt) on various human cancer cells, including GBM cell lines and xenograft tumor tissues.Citation91 In vitro and in vivo models have shown that enzastaurin combined with RT synergistically reduces tumor volume and radiation-induced tumor satellite formation, upregulates VEGF expression, and induces tumor–vasculature destruction.Citation92–Citation94 In nude mice with orthotopic LNT-229 glioma cells, the addition of enzastaurin to RT reduced radiation-induced tumor satellite formation, thus supporting the crucial role of enzastaurin in preventing the proangiogenic effect of RT.
The safety and clinical activity of enzastaurin in association with standard RT and TMZ treatment in patients with newly diagnosed GBM have been explored in a few clinical trials (). Butowski et alCitation95 reported a single-institution Phase I dose-escalation trial of enzastaurin with standard chemoradiation in patients with newly diagnosed GBM or gliosarcoma. Enzastaurin was administered at doses of 250 mg (n = 6) or 500 mg (n = 6) daily from the night before the beginning of RT. Thereafter, patients received enzastaurin at 250 mg or 500 mg daily and TMZ for up to twelve cycles until tumor progression or unacceptable toxicity. No DLTs were observed among patients receiving the 250 mg dose, while one grade 3 and one grade 4 thrombocytopenia was observed in the 500 mg arm. On the basis of this toxicity profile, a Phase II study using enzastaurin at 250 mg daily was conducted in 66 patients with newly diagnosed GBM or gliosarcoma.Citation96 Combination therapy was well tolerated and discontinuation of treatment was required in 9% of patients. Median overall survival and progression-free survival rates were 74 weeks and 36 weeks, respectively. Results were comparable to those observed in historical Phase II studies of erlotinib in association with standard RT and TMZ treatment,Citation4 and better than those observed with either thalidomideCitation97 or cis-retinoic acid.Citation98
Combinations of integrin inhibitors with radiation
Integrins are a family of heterodimeric transmembrane glycoproteins known to play critical roles in cell–cell adhesion and cell interaction with specific extracellular matrix proteins. Among integrins, the αv integrins, particularly αvβ3 and αvβ5, are overexpressed in both tumor-associated vasculature and glioma cells,Citation99,Citation100 and their activation triggers pathways involved in tumor-induced angiogenesis, cell proliferation, and survival.Citation101–Citation104 The antiangiogenic and antitumor effects of combining integrin inhibitors and radiation have been observed in preclinical models.Citation105–Citation109 Blockade of αvβ3 and αvβ5 integrins in combination with RT induces apoptosis in endothelial cells in vitro,Citation105,Citation106 and inhibits tumor growth in U87 GBM xenografts in vivo.Citation105 Moreover, in U87 and SF763 GBM cell lines, targeting αvβ3 and αvβ5 integrins significantly reduces cell survival after irradiation.Citation107 In vivo models have also shown that the enhanced antitumor effect of combined treatment depends on inhibition of radiation-induced αv integrins and VEGFR signaling pathways, and activation of apoptosis in both tumor cells and tumor vascular endothelial cells.Citation108 In addition, targeting αv integrins enhances blood perfusion and reduces tumor hypoxia, thus increasing tumor response to radiation therapy.Citation109
Cilengitide
Cilengitide (EMD 121974; Merck KgaA, Darmstadt, Germany), is a cyclized Arg-Gly-Glu(RGD)-containing pentapeptide that selectively inhibits αvβ3 and αvβ5 integrins at subnanomolar concentrations.Citation110–Citation112 Cilengitide has been evaluated in Phase I/II trials as a single agent and in combination with other chemotherapeutic agents in a variety of solid tumors, including prostate, pancreatic, and head and neck cancers.Citation113–Citation115 Cilengitide failed to demonstrate any clear survival advantage in these tumors; however, clinical activity was reported in patients with recurrent GBM.Citation116–Citation119
In vitro and in vivo studies have demonstrated the potential value of targeting αvβ3 and αvβ5 integrins with cilengitide in combination with RT in high-grade gliomas.Citation120,Citation121 Cilengitide combined with RT in vivo demonstrated more than doubling of the median survival time (>110 days) as compared to RT alone (50 days).Citation121 RT induces expression of αvβ3 integrins in human umbilical vein endothelial cells, and combined treatment with cilengitide and single-dose irradiation enhances detachment and apoptosis of these cells as compared to cilengitide or RT alone.Citation120
Based on the results of preclinical studies, the efficacy and safety of combining cilengitide with RT in patients with newly diagnosed GBM have been assessed in a few recent studies (). In an initial Phase I/II study of 52 patients who received cilengitide at a dose of 500 mg twice weekly in association with standard chemoradiation, Stupp et alCitation13 reported a median survival of 16.1 months and a 6-month progression-free survival of 69%. According to the methylation status of the MGMT gene promoter, patients with methylated MGMT promoter had significantly longer progression-free survival and overall survival as compared with those with unmethylated tumors. The treatment regimen was well tolerated. The most common toxicities were thrombocytopenia, intracranial hemorrhage, neuropathy, and idiosyncratic liver toxicity. Thromboembolic events and grade 1/2 hypertension were reported in three patients and five patients, respectively. Discontinuation of therapy due to possible treatment-related toxicity occurred in 14% of patients.
In a randomized Phase II trial of the New Agents Brain Tumor Treatment cooperative group (NABTT 0306), 112 patients with newly diagnosed GBM were randomized to receive cilengitide at a dose of 500 mg or 2,000 mg twice weekly concomitantly with standard treatment.Citation14 After six cycles of adjuvant TMZ, cilengitide was given as a single agent until tumor progression. Median survival and 2-year survival rates were 19.7 months and 38%, respectively, with a more favorable trend for patients treated in the 2,000 mg arm. The median progression-free survival was 10 months, with no differences between the two dose groups. Combined treatment was well tolerated with no DLTs observed at any dose level. Interestingly, the trial confirmed a survival benefit for patients who had methylated MGMT status, with a reported overall survival of 30 months for methylated patients and 19.1 months for unmethylated patients, respectively. Based on these results, a large multicentric Phase III randomized study Cilengitide in Combination with Temozolomide and Radiotherapy in Newly Diagnosed Glioblastoma phase III Randomized clinical trial (CENTRIC study) of more than 500 patients has assessed the efficacy and safety of cilengitide in combination with standard treatment versus standard treatment alone in newly diagnosed GBM patients with a methylated MGMT promoter gene.Citation122 Unfortunately, the results of the study showed that the addition of cilengitide to the standard treatment of RT and TMZ did not improve overall survival. A similar trial Cilengitide in Patients with newly Diagnosed and Glioblastoma Multiforme and unmethylated MGMT gene promoter (CORE study) is currently evaluating GBM patients with an unmethylated MGMT gene promoter status treated with standard chemoradiation or chemoradiation plus cilengitide, although no results have been reported yet.Citation122
Combinations of EGFR inhibitors with radiation
The EGFR is a transmembrane glycoprotein that constitutes one of four members of the ErbB family of tyrosine kinase receptors. It consists of an extracellular ligand-binding domain, a transmembrane segment, and an intracellular domain with an ATP-binding site and tyrosine kinase activity. EGFR is activated by ligand binding to the extracellular domain, which leads to rapid receptor dimerization and subsequent activation of tyrosine kinase activity in the intracellular domain. This results in the stimulation of downstream signaling effectors including PI3K, Akt, Ras, and mitogen-activated protein kinases, which are involved in cell proliferation, survival, migration, and apoptosis.Citation123 EGFR is highly expressed in a variety of solid tumors, including high-grade gliomas.Citation124 Approximately 40% of GBMs are characterized by EGFR gene amplification and overexpression,Citation125,Citation126 which promote tumor growth, migration and invasion,Citation127 and induce resistance to radiation.Citation128 Amplification of the EGFR gene is often associated with a mutation that encodes for a truncated form of the receptor, known as EGFR variant vIII (EGFRvIII), which lacks the extracellular binding domain leading to constitutive activation of tyrosine kinase.Citation125,Citation129 Expression of EGFRvIII correlates with poor survival in GBM patientsCitation130,Citation131 and promotes glioma cell migration,Citation132 tumor growth, invasion, survival,Citation133 and angiogenesis.Citation134 Moreover, it was shown that resistance of GBM cells in vitro toward RT is related to Human Epidermal Receptor (HER1)/EGFR overexpression.Citation128,Citation135 A large number of potentially therapeutic targets have been developed in order to block the EGFR signaling pathways, including monoclonal antibodies cetuximab (Erbitux®; Eli Lilly and Company; Bristol-Myers Squibb, New York, NY, USA), and TKIs gefitinib (Iressa™; AstraZeneca Pharmaceuticals), erlotinib (Tarceva®; OSI Pharmaceuticals, Inc, Melville, NY, USA; F Hoffman-La Roche, Ltd, Basel, Switzerland; Genentech, Inc) and lapatinib (Tykerb®; GlaxoSmithKline plc, London, UK). Erlotinib and gefitinib are two structurally related, orally active small molecule reversible TKIs that compete for the ATP-binding site in the intracellular tyrosine kinase domain of EGFR, thereby resulting in the inhibition of downstream signal transduction pathways.Citation136 Both targeted drugs have shown clinical activity against several cancer types, and both received approval as a second- or third-line treatment in previously treated advanced NSCLC.Citation137,Citation138 Erlotinib has also been approved in combination with gemcitabine for locally advanced, unresectable, or metastatic pancreatic cancer;Citation139 however, the use of EGFR inhibitors, erlotinib and gefitinib, as single agents in patients with progressive GBM has shown no significant survival benefit.Citation140,Citation141
In vitro and in vivo studies have provided strong evidence for the capacity of EGFR TKIs, erlotinib and gefitinib, to enhance the antitumor activity of ionizing radiation. Published data suggest that EGFR TKIs may enhance radiation responses at several levels, including through cell cycle kinetics, DNA damage repair, apoptosis induction, and the targeting of accelerated cellular repopulation.Citation142–Citation146 Moreover, EGFR inhibitors like erlotinib may decrease tumor hypoxia, thereby rendering cells more susceptible to the cytotoxic effects of radiation. Therefore, this strategy has been tested in Phase I/II clinical studies ().
Table 2 Clinical trials of EGFR and mTOR inhibitors in combination with radiotherapy
An initial Phase I trial of erlotinib with standard RT and TMZ treatment in patients with newly diagnosed GBM was performed by the North Central Cancer Treatment Group (NCCTG).Citation147 Erlotinib was given orally daily throughout standard RT and TMZ, starting 1 week before the beginning of chemoradiotherapy during the 6-month cycles of adjuvant TMZ, and this regimen was continued until tumor progression. The drug was started at a dose of 100 mg/day and was escalated to 150 mg/day for patients not on EIAEDs (n = 10) and 200 mg/day for patients on EIAEDs (n = 9). The MTD was not reached, and only one DLT (stomatitis) was observed in the 100 mg group. At a median follow-up of 52 weeks, the median overall survival rates in the two arms were 51 weeks and 66 weeks, respectively. Another Phase I dose-escalation trial of erlotinib with RT limited to patients aged 3 years to 25 years with newly diagnosed high-grade gliomas was conducted by Broniscer et al.Citation148 Erlotinib was administered once daily during and after RT for up to 3 years, starting at 70 mg/m2 to the final dosage of 160 mg/m2. The recommended MTD was 120 mg/m2 per day. Toxicities reported in 23 evaluable patients included one grade 3 diarrhea at 120 mg/m2, one grade 3 serum lipase increase, and one grade 3 rash and pruritus at 160 mg/m2. The 1-year progression-free survival and overall survival were 56% and 78%, respectively.
Prados et alCitation4 have evaluated the efficacy of erlotinib combined to standard RT and TMZ treatment in 65 patients with newly diagnosed GBM or gliosarcoma. Erlotinib was administered during RT at a dose of 100 mg/day for patients not on EIAEDs and 200 mg/day for patients on EIAEDs. Two weeks after completion of chemoradiation, therapy was continued with adjuvant TMZ and erlotinib at a dose of 150 mg/day for patients not on EIAEDs, and 300 mg/day for patients on EIAEDs. The dose was escalated 50 mg per day every 2 weeks to a maximum of 200 mg/day or 500 mg/day for either group, respectively. The most common grade 3 to 4 toxicities likely related to erlotinib were diarrhea, rash, and fatigue. Median overall survival and progression-free survival were 19.3 months and 8.2 months, respectively, which compared favorably with two historical Phase II trials of patients with GBM treated with RT and TMZ in association with thalidomide or cis-retinoic acid.Citation97,Citation98 Patients with the MGMT gene promoter methylation, as well as patients with either MGMT promoter-methylated tumor and intact phosphatase and tensin homologue (PTEN), a tumor-suppressor protein that inhibits the PI3K signaling pathway, had a significantly longer median survival when compared with patients with unmethylated MGMT (25.5 months versus 14.6 months, P = 0.006).
Brown et alCitation149 have reported the results of a Phase I/II study conducted by the NCCTG (N0177 Study) in 93 patients with newly diagnosed GBM treated with erlotinib at a dose of 150 mg/day combined with standard RT and TMZ. Median progression-free survival and overall survival rates were 7.2 months and 15.3 months, respectively, being not significantly different compared to historical data from the European Organization for Research and Treatment of Cancer, National Cancer Institute of Canada (NCIC) trial conducted by Stupp et al.Citation2 Different from the Prados et alCitation4 study, no differences were found in survival rates in patient groups characterized by EGFRvIII plus wild PTEN versus groups without these genotypic features. Moreover, the addition of erlotinib was associated with increased toxicity compared with standard RT and TMZ treatment, with two reported grade 5 nonneutropenic pneumonias. In another Phase II study of patients with newly diagnosed GBM, erlotinib was given from the first day of standard RT and TMZ at a dose of 50 mg/day with escalation by 50 mg/day every 2 weeks to a maximum dose of 150 mg/day, until the occurrence of toxicity or disease progression.Citation3 Median progression-free survival and overall survival rates were 2.8 months and 8.6 months, respectively. Treatment-related grade 3 or 4 toxicities included thrombocytopenia, anemia, lymphopenia, fatigue, and febrile neutropenia. Three deaths that were attributed to treatment occurred during the study, leading to early closure of the trial – after enrollment of 27 of the 30 planned patients.
Few trials have reported on the combination of gefitinib with RT as first-line treatment in both adult and pediatric patients, or at tumor recurrence (). A Phase I dose-escalation study of 15 patients with recurrent malignant gliomas treated with fractionated stereotactic radiosurgery in combination with gefitinib was performed by Schwer et al.Citation150 Gefitinib was administered orally at a dose of 250 mg/day starting 1 week before fractionated stereotactic radiosurgery and continued for up to 1 year, or until disease progression or unacceptable toxicity. The initial dosage of Stereotactic Radio Surgery (SRS) was 18 Gy delivered in three fractions over 3 consecutive days, and subsequent RT doses were 24 Gy, 30 Gy, and 36 Gy. Treatment was well tolerated, and grade 3/4 toxicities were not reported. At a median follow-up of 7 months, the median overall survival and progression-free survival rates were 10 months and 7 months, respectively.
The Pediatric Brain Tumor Consortium initiated a Phase I trial of gefitinib and RT in children with newly diagnosed brainstem gliomas or incompletely resected supratentorial malignant gliomas.Citation151 Thirty-three patients aged 3 years to 21 years were included in the study. Gefitinib was started concomitantly to RT. Gefitinib at a starting dose of 100 mg/m2 was administered orally once daily from the first day of RT, and the dose was subsequently escalated to 250 mg/m2 and 375 mg/m2. In the absence of disease progression or DLT, treatment was continued for 1 year. Although systemic toxicities were generally mild-moderate and reversible, there were four cases of symptomatic intratumoral hemorrhage and the trial was prematurely closed. In total, 250 mg/m2 was established as the recommended Phase II dose. The 1-year survival and progression-free survival rates were 48% and 16.1% for patients with brainstem glioma, and 28.8% and 15.4%, for patients with supratentorial glioma, respectively. In the subsequent Phase II trial, 43 children were enrolled and received gefitinib at a dose of 250 mg/m2/day in combination with RT.Citation152 One-year progression-free survival and overall survival rates were 20.9% and 56.4%, respectively. The most frequent toxicity was lymphopenia. Three patients experienced intratumoral hemorrhage, which was symptomatic in two cases.
More recently, the Radiation Therapy Oncology Group conducted a Phase I/II study to evaluate the safety and efficacy of gefitinib administered with RT in patients with newly diagnosed GBM.Citation153 In the Phase I part of the trial, gefitinib was given at 250 mg daily and escalated to a maximum dose of 750 mg for patients on EIAEDs (n = 18) or 500 mg for patients not on EIAEDs (n = 13). After the completion of RT, gefitinib was continued as a single-agent for 18 months, or until disease progression or unacceptable toxicity. The MTD was established to be 750 mg for patients on EIAEDs and 500 mg for patients not on EIAEDs. The most frequent reported toxicities were dermatologic, gastrointestinal, and fatigue. Therefore, 147 patients were enrolled to the Phase II component of the study that included only patients not on EIAEDs treated with gefitinib at 500 mg in combination with RT. Treatment was well tolerated with grade 3/4 rash, grade 3/4 gastrointestinal toxicity, grade 3/4 liver function test abnormalities, and grade 3/4 cardiovascular complications being the most common adverse events. However, despite a relatively good toxicity profile, overall survival was not significantly improved by the addition of gefitinib to RT, as compared to historical controls treated with RT alone (11.5 months versus 11 months).
Combination of mTOR inhibitors with RT
The mTOR complex is a serine–threonine kinase composed of two proteins, mTOR complex 1 and 2 (mTORC1 and mTORC2), that acts as a downstream effector of the PI3K and Akt/PKB (Protein Kinase B) signaling pathway.Citation154 Specifically, mTOR is regulated through activation of the PI3K/Akt cascade and promotes cell growth and proliferation through phosphorylation and inactivation of the translational regulator eukaryotic initiation factor 4E-binding protein, as well as through phosphorylation and activation of the 70 kd S6 (S6K1) ribosomal protein kinase.Citation155 An upstream negative regulator of this pathway is the tumor suppressor PTEN, which is commonly mutated in 20%–40% of GBMs.Citation156 Thus, targeting the mTOR complex may represent an attractive therapeutic approach for GBM, and synthetic analogs of rapamycin (sirolimus), including temsirolimus (Torisel®; Wyeth Pharmaceuticals, Madison, NJ, USA), everolimus (Afinitor®; Novartis Vaccines and Diagnostics AG, Basel, Switzerland), and ridaforolimus (MK-8669; AP23573; Merck KgaA; ARIAD Pharmaceuticals, Inc, Cambridge, MA, USA) are currently being tested in GBM. Temsirolimus and everolimus have received US FDA and European Medicines Agency approval for the treatment of advanced renal cell carcinoma, as well as for treatment of patients with subependymal giant cell astrocytoma, tuberous sclerosis, advanced breast cancer, and pancreatic neuroendocrine tumors (everolimus).Citation157,Citation158
Preclinical studies have shown that mTOR inhibitors can enhance tumor response to radiation by affecting both tumor vasculature and tumor cell viability through different mechanisms. The addition of everolimus to RT sensitizes GBM cell lines to radiation by decreasing cell survival through the activation of apoptosis, the induction of cell cycle arrest,Citation159,Citation160 and the upregulation of autophagy.Citation161 In addition, combined treatment decreases tumor vessel density and blood flow in vivo.Citation162 In U87 GBM xenografts, the addition of rapamycin to RT significantly enhances tumor growth control compared to either radiation or rapamycin alone.Citation159
Two Phase I trials have investigated the safety and efficacy of mTOR inhibitors in combination with RT in GBM (). NCCTG conducted a Phase I dose-escalation trial of temsirolimus with RT and TMZ in patients with newly diagnosed GBM.Citation163 Temsirolimus was administered intravenously weekly 1 week before chemoradiation and continued with adjuvant TMZ for up to six cycles. The dose started at 25 mg/week and was escalated to the final dosage of 75 mg/week. Among the first twelve patients enrolled, six patients developed an infection during adjuvant TMZ, and three of these patients died. Subsequently, 13 additional patients received temsirolimus only concomitantly to RT and TMZ. DLTs occurred to doses of 75 mg/week in two out of six patients during RT and included dysgeusia, hypercholesterolemia, hypertriglyceridemia, thrombocytopenia, thrombosis, and pulmonary embolism. The recommended dose was 50 mg/week. At a median follow-up of 10.2 months, stable disease was reported in 24 patients and progressive disease was reported in one patient.Citation163
The NCCTG also performed a Phase I trial to evaluate the safety and tolerability of everolimus with standard RT and TMZ treatment in 18 patients with newly diagnosed GBM.Citation164 Everolimus was administered orally once per week beginning 1 week before RT. The starting dose was 30 mg/week with subsequent escalations to 50 mg/week and 70 mg/week in cohorts of six patients. After completion of concomitant treatment, everolimus was given weekly in combination with TMZ for 6 months, or until disease progression or toxicity. Treatment-related DLTs were one instance of grade 3 fatigue at doses of 30 mg/week, one grade 4 myelotoxicity at doses of 50 mg/week, and one grade 4 liver dysfunction at doses of 70 mg/week. Consequently, a dose of 70 mg/weekly was recommended for Phase II studies. A partial response was reported in one patient and stable disease was reported in 15 patients. Given the small number of patients in both trials, no conclusions can be drawn on safety and efficacy of mTOR inhibitors combined with RT, and further investigation is warranted.
Conclusion
An increasing body of preclinical data show that inhibition of EGFR-, VEGFR-, integrin-, and mTOR-mediated signaling may enhance the effect of radiation through several mechanisms, including activation of apoptosis, induction of cell cycle arrest, inhibition of angiogenesis, and by improving tumor oxygenation. Several trials have assessed the efficacy of combining targeted agents with radiation in newly diagnosed and recurrent high-grade gliomas; however, despite the strong rationale for their use in clinical trials, most studies have shown very modest results. Currently, only the use of bevacizumab in combination with RT plus TMZ has been associated with improved progression-free survival and quality of life in patients with newly diagnosed GBM in a large randomized study, although without significant survival benefit. In contrast, Phase II/III trials evaluating the addition of single agents targeting angiogenesis, integrins, and EGFR-signaling pathways showed no survival advantages when compared to the standard treatment of TMZ plus RT alone; however, in a study testing EGFR TKI erlotinib in combination with RT and TMZ, a subset of patients with MGMT promoter methylation and PTEN positivity showed significantly longer survival.Citation4
The negative results reported in the majority of published clinical studies may be explained, at least in part, by this single-target approach, which may be somewhat limited by such factors as tumor heterogeneity and genetic instability. Heterogeneity of the GBM cell population, which includes expression of cell surface receptors, as well as proliferative and angiogenic potential, might be attributed to morphological and epigenetic plasticity, but there is also evidence for the coexistence of genetically divergent tumor cell clones within tumors. So far, if multiple oncogenic processes are active in distinct tumor subpopulations, single-target therapies may provide limited effects. Furthermore, GBM cells may exhibit significant genetic instability, possibly leading to resistance of single-targeted agents by switching to alternative molecular pathways that may influence radiation resistance. This complex interaction between tumor-specific signaling and radiation response provides a rationale for the use of multiple single-targeted therapies that can simultaneously inhibit a variety of molecular pathways, including growth factor receptor signaling pathways, DNA damage repair processes, and angiogenesis. A better understanding of the multiple mechanisms underlying radiation response and resistance in GBM will help to select patients based on molecular biomarkers, who may benefit from multitarget therapy regimens in clinical trials.
Disclosure
The authors report no conflicts of interest in this work.
References
- DeorahSLynchCFSibenallerZARykenTCTrends in brain cancer incidence and survival in the United States: Surveillance, Epidemiology, and End Results Program, 1973 to 2001Neurosurg Focus2006204E116709014
- StuppRMasonWPvan den BentMJEuropean Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy GroupsNational Cancer Institute of Canada Clinical Trials GroupRadiotherapy plus concomitant and adjuvant temozolomide for glioblastomaN Engl J Med20053521098799615758009
- PeereboomDMShepardDRAhluwaliaMSPhase II trial of erlotinib with temozolomide and radiation in patients with newly diagnosed glioblastoma multiformeJ Neurooncol2010981939919960228
- PradosMDChangSMButowskiNPhase II study of erlotinib plus temozolomide during and after radiation therapy in patients with newly diagnosed glioblastoma multiforme or gliosarcomaJ Clin Oncol200927457958419075262
- UhmJHBallmanKVWuWPhase II evaluation of gefitinib in patients with newly diagnosed Grade 4 astrocytoma: Mayo/North Central Cancer Treatment Group Study N0074Int J Radiat Oncol Biol Phys201180234735320510539
- FranceschiECavalloGLonardiSGefitinib in patients with progressive high-grade gliomas: a multicentre phase II study by Gruppo Italiano Cooperativo di Neuro-Oncologia (GICNO)Br J Cancer20079671047105117353924
- NaborsLBSupkoJGRosenfeldMNew Approaches to Brain Tumor Therapy (NABTT) CNS Consortium. Phase I trial of sorafenib in patients with recurrent or progressive malignant gliomaNeuro-oncology201113121324133021954442
- FieldsECDamekDGasparLEPhase I dose escalation trial of vandetanib with fractionated radiosurgery in patients with recurrent malignant gliomasInt J Radiat Oncol Biol Phys2012821515721035955
- GerstnerEREichlerAFPlotkinSRPhase I trial with biomarker studies of vatalanib (PTK787) in patients with newly diagnosed glioblastoma treated with enzyme inducing anti-epileptic drugs and standard radiation and temozolomideJ Neurooncol2011103232533220821342
- VredenburghJJDesjardinsAReardonDAThe addition of bevacizumab to standard radiation therapy and temozolomide followed by bevacizumab, temozolomide, and irinotecan for newly diagnosed glioblastomaClin Cancer Res201117124119412421531816
- LaiATranANghiemphuPLPhase II study of bevacizumab plus temozolomide during and after radiation therapy for patients with newly diagnosed glioblastoma multiformeJ Clin Oncol201129214214821135282
- GalanisEBucknerJCMaurerMJNorth Central Cancer Treatment GroupPhase II trial of temsirolimus (CCI-779) in recurrent glioblastoma multiforme: a North Central Cancer Treatment Group StudyJ Clin Oncol200523235294530415998902
- StuppRHegiMENeynsBPhase I/IIa study of cilengitide and temozolomide with concomitant radiotherapy followed by cilengitide and temozolomide maintenance therapy in patients with newly diagnosed glioblastomaJ Clin Oncol201028162712271820439646
- NaborsLBMikkelsenTHegiMENew Approaches to Brain Tumor Therapy (NABTT) Central Nervous System Consortium. A safety run-in and randomized phase 2 study of cilengitide combined with chemoradiation for newly diagnosed glioblastoma (NABTT 0306)Cancer2012118225601560722517399
- MinnitiGMuniRLanzettaGchemotherapy for glioblastoma: current treatment and future perspectives for cytotoxic and targeted agentsAnticancer Res200929125171518420044633
- DorseyKAgulnikMPromising new molecular targeted therapies in head and neck cancerDrugs201373431532523440867
- PetrosyanFDawHHaddadASpiroTTargeted therapy for lung cancerAnticancer Drugs201223101016102122932130
- GorskiDHBeckettMAJaskowiakNTBlockage of the vascular endothelial growth factor stress response increases the antitumor effects of ionizing radiationCancer Res199959143374337810416597
- GengLDonnellyEMcMahonGInhibition of vascular endothelial growth factor receptor signaling leads to reversal of tumor resistance to radiotherapyCancer Res20016162413241911289107
- GuptaVKJaskowiakNTBeckettMAVascular endothelial growth factor enhances endothelial cell survival and tumor radioresistanceCancer J200281475411895203
- HovingaKEStalpersLJvan BreeCRadiation-enhanced vascular endothelial growth factor (VEGF) secretion in glioblastoma multiforme cell lines – a clue to radioresistance?J Neurooncol20057429910316193379
- WachsbergerPRBurdRCardiCVEGF trap in combination with radiotherapy improves tumor control in u87 glioblastomaInt J Radiat Oncol Biol Phys20076751526153717234361
- KilWJTofilonPJCamphausenKPost-radiation increase in VEGF enhances glioma cell motility in vitroRadiat Oncol201272522356893
- BirnerPPiribauerMFischerIVascular patterns in glioblastoma influence clinical outcome and associate with variable expression of angiogenic proteins: evidence for distinct angiogenic subtypesBrain Pathol200313213314312744467
- PrestaLGChenHO’ConnorSJHumanization of an anti-vascular endothelial growth factor monoclonal antibody for the therapy of solid tumors and other disordersCancer Res19975720459345999377574
- GerberHPFerraraNPharmacology and pharmacodynamics of bevacizumab as monotherapy or in combination with cytotoxic therapy in preclinical studiesCancer Res200565367168015705858
- YuanFChenYDellianMSafabakhshNFerraraNJainRKTime-dependent vascular regression and permeability changes in established human tumor xenografts induced by an anti-vascular endothelial growth factor/vascular permeability factor antibodyProc Natl Acad Sci USA1996932514765147708962129
- BorgströmPHillanKJSriramaraoPFerraraNComplete inhibition of angiogenesis and growth of microtumors by anti-vascular endothelial growth factor neutralizing antibody: novel concepts of angiostatic therapy from intravital videomicroscopyCancer Res19965617403240398752175
- WillettCGBoucherYdi TomasoEDirect evidence that the VEGF-specific antibody bevacizumab has antivascular effects in human rectal cancerNat Med200410214514714745444
- HurwitzHFehrenbacherLNovotnyWBevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancerN Engl J Med2004350232335234215175435
- SandlerAGrayRPerryMCPaclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancerN Engl J Med2006355242542255017167137
- EscudierBPluzanskaAKoralewskiPAVOREN Trial investigatorsBevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: a randomised, double-blind phase III trialLancet200737096052103211118156031
- FriedmanHSPradosMDWenPYBevacizumab alone and in combination with irinotecan in recurrent glioblastomaJ Clin Oncol200927284733474019720927
- KreislTNKimLMooreKPhase II trial of single-agent bevacizumab followed by bevacizumab plus irinotecan at tumor progression in recurrent glioblastomaJ Clin Oncol200927574074519114704
- WinklerFKozinSVTongRTKinetics of vascular normalization by VEGFR2 blockade governs brain tumor response to radiation: role of oxygenation, angiopoietin-1, and matrix metalloproteinasesCancer Cell20046655356315607960
- HoangTHuangSArmstrongEEickhoffJCHarariPMEnhancement of radiation response with bevacizumabJ Exp Clin Cancer Res2012313722538017
- LeeCGHeijnMdi TomasoEAnti-vascular endothelial growth factor treatment augments tumor radiation response under normoxic or hypoxic conditionsCancer Res200060195565557011034104
- DingsRPLorenMHeunHScheduling of radiation with angiogenesis inhibitors anginex and Avastin improves therapeutic outcome via vessel normalizationClin Cancer Res200713113395340217545548
- McGeeMCHamnerJBWilliamsRFImproved intratumoral oxygenation through vascular normalization increases glioma sensitivity to ionizing radiationInt J Radiat Oncol Biol Phys20107651537154520338480
- NarayanaAGolfinosJGFischerIFeasibility of using bevacizumab with radiation therapy and temozolomide in newly diagnosed high-grade gliomaInt J Radiat Oncol Biol Phys200872238338918793954
- NarayanaAGruberDKunnakkatSA clinical trial of bevacizumab, temozolomide, and radiation for newly diagnosed glioblastomaJ Neurosurg2012116234134522035272
- LaiAFilkaEMcGibbonBPhase II pilot study of bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly diagnosed glioblastoma multiforme: interim analysis of safety and tolerabilityInt J Radiat Oncol Biol Phys20087151372138018355978
- VredenburghJJDesjardinsAKirkpatrickJPAddition of bevacizumab to standard radiation therapy and daily temozolomide is associated with minimal toxicity in newly diagnosed glioblastoma multiformeInt J Radiat Oncol Biol Phys2012821586621036490
- HainsworthJDShihKCShepardGCTillinghastGWBrinkerBTSpigelDRPhase II study of concurrent radiation therapy, temozolomide, and bevacizumab followed by bevacizumab/everolimus as first-line treatment for patients with glioblastomaClin Adv Hematol Oncol201210424024622706484
- ChinotOLde La Motte RougeTMooreNAVAglio: Phase 3 trial of bevacizumab plus temozolomide and radiotherapy in newly diagnosed glioblastoma multiformeAdv Ther201128433434021432029
- GutinPHIwamotoFMBealKSafety and efficacy of bevacizumab with hypofractionated stereotactic irradiation for recurrent malignant gliomasInt J Radiat Oncol Biol Phys200975115616319167838
- ShapiroLQBealKGoenkaAPatterns of failure after concurrent bevacizumab and hypofractionated stereotactic radiation therapy for recurrent high-grade gliomaInt J Radiat Oncol Biol Phys201385363664222765876
- NiyaziMGanswindtUSchwarzSBIrradiation and bevacizumab in high-grade glioma retreatment settingsInt J Radiat Oncol Biol Phys2012821677621030162
- HundsbergerTBrüggeDPutoraPMWederPWeberJPlasswilmLRe-irradiation with and without bevacizumab as salvage therapy for recurrent or progressive high-grade gliomasJ Neurooncol2013112113313923314822
- HennequinLFStokesESThomasAPNovel 4-anilinoquinazolines with C-7 basic side chains: design and structure activity relationship of a series of potent, orally active, VEGF receptor tyrosine kinase inhibitorsJ Med Chem20024561300131211881999
- CiardielloFCaputoRDamianoVAntitumor effects of ZD6474, a small molecule vascular endothelial growth factor receptor tyrosine kinase inhibitor, with additional activity against epidermal growth factor receptor tyrosine kinaseClin Cancer Res2003941546155612684431
- BraveSROdedraRJamesNHVandetanib inhibits both VEGFR-2 and EGFR signalling at clinically relevant drug levels in preclinical models of human cancerInt J Oncol201139127127821537841
- LeboulleuxSBastholtLKrauseTVandetanib in locally advanced or metastatic differentiated thyroid cancer: a randomised, double-blind, phase 2 trialLancet Oncol201213989790522898678
- MeyerhardtJAAncukiewiczMAbramsTAPhase I study of cetuximab, irinotecan, and vandetanib (ZD6474) as therapy for patients with previously treated metastastic colorectal cancerPLoS One201276e3823122701615
- LeeJSHirshVParkKVandetanib Versus placebo in patients with advanced non-small-cell lung cancer after prior therapy with an epidermal growth factor receptor tyrosine kinase inhibitor: a randomized, double-blind phase III trial (ZEPHYR)J Clin Oncol201230101114112122370318
- HsuCYangTSHuoTIVandetanib in patients with inoperable hepatocellular carcinoma: a phase II, randomized, double-blind, placebo-controlled studyJ Hepatol20125651097110322245891
- ThorntonKKimGMaherveVandetanib for the treatment of sympomatic or progressive medullary thyroid cancer in patients with unresectable locally advanced or metastatic disease: U.SFood and Drug administration drug approval cemicar cancer Res2012181437223730
- AnsiauxRDeweverJGrégoireVFeronOJordanBFGallezBDecrease in tumor cell oxygen consumption after treatment with vandetanib (ZACTIMA; ZD6474) and its effect on response to radiotherapyRadiat Res2009172558459119883226
- DamianoVMelisiDBiancoCCooperative antitumor effect of multitargeted kinase inhibitor ZD6474 and ionizing radiation in glioblastomaClin Cancer Res200511155639564416061883
- SandströmMJohanssonMBergströmPBergenheimATHenrikssonREffects of the VEGFR inhibitor ZD6474 in combination with radiotherapy and temozolomide in an orthotopic glioma modelJ Neurooncol20088811918228115
- GustafsonDLFrederickBMerzALRabenDDose scheduling of the dual VEGFR and EGFR tyrosine kinase inhibitor vandetanib (ZD6474, Zactima) in combination with radiotherapy in EGFR-positive and EGFR-null human head and neck tumor xenograftsCancer Chemother Pharmacol200861217918817393165
- WilliamsKJTelferBABraveSZD6474, a potent inhibitor of vascular endothelial growth factor signaling, combined with radiotherapy: schedule-dependent enhancement of antitumor activityClin Cancer Res200410248587859315623642
- SiemannDWHorsmanMRTargeting the tumor vasculature: a strategy to improve radiation therapyExpert Rev Anticancer Ther20044232132715056061
- BrazelleWDShiWSiemannDWVEGF-associated tyrosine kinase inhibition increases the tumor response to single and fractionated dose radiotherapyInt J Radiat Oncol Biol Phys200665383684116751064
- DrappatzJNordenADWongETPhase I study of vandetanib with radiotherapy and temozolomide for newly diagnosed glioblastomaInt J Radiat Oncol Biol Phys2010781859020137866
- BroniscerABakerJNTagenMPhase I study of vandetanib during and after radiotherapy in children with diffuse intrinsic pontine gliomaJ Clin Oncol201028314762476820921456
- WoodJMBoldGBuchdungerEPTK787/ZK222584, a novel and potent inhibitor of vascular endothelial growth factor receptor tyrosine kinases, impairs vascular endothelial growth factor-induced responses and tumor growth after oral administrationCancer Res20006082178218910786682
- ErberRThurnherAKatsenADCombined inhibition of VEGF and PDGF signaling enforces tumor vessel regression by interfering with pericyte-mediated endothelial cell survival mechanismsFASEB J200418233834014657001
- HasumiYKłosowska-WardegaAFuruhashiMOstmanAHeldinCHHellbergCIdentification of a subset of pericytes that respond to combination therapy targeting PDGF and VEGF signalingInt J Cancer2007121122606261417691110
- HessCVuongVHegyiIEffect of VEGF receptor inhibitor PTK787/ZK222584 [correction of ZK222548] combined with ionizing radiation on endothelial cells and tumour growthBr J Cancer200185122010201611747347
- ZipsDKrauseMHesselFExperimental study on different combination schedules of VEGF-receptor inhibitor PTK787/ZK222584 and fractionated irradiationAnticancer Res2003235A3869387614666690
- ZipsDEichelerWGeyerPEnhanced susceptibility of irradiated tumor vessels to vascular endothelial growth factor receptor tyrosine kinase inhibitionCancer Res200565125374537915958586
- BrandesAAStuppRHauPEORTC study 26041-22041: phase I/II study on concomitant and adjuvant temozolomide (TMZ) and radiotherapy (RT) with PTK787/ZK222584 (PTK/ZK) in newly diagnosed glioblastomaEur J Cancer201046234835419945857
- HechtJRTrarbachTHainsworthJDRandomized, placebo-controlled, phase III study of first-line oxaliplatin-based chemotherapy plus PTK787/ZK222584, an oral vascular endothelial growth factor receptor inhibitor, in patients with metastatic colorectal adenocarcinomaJ Clin Oncol201129151997200321464406
- Van CutsemEBajettaEValleJRandomized, placebo-controlled, phase III study of oxaliplatin, fluorouracil, and leucovorin with or without PTK787/ZK222584 in patients with previously treated metastatic colorectal adenocarcinomaJ Clin Oncol201129152004201021464401
- AdnaneLTrailPATaylorIWilhelmSMSorafenib (BAY 43-9006, Nexavar), a dual-action inhibitor that targets RAF/MEK/ERK pathway in tumor cells and tyrosine kinases VEGFR/PDGFR in tumor vasculatureMeth Enzymol200640759761216757355
- WilhelmSMAdnaneLNewellPVillanuevaALlovetJMLynchMPreclinical overview of sorafenib, a multikinase inhibitor that targets both Raf and VEGF and PDGF receptor tyrosine kinase signalingMol Cancer Ther20087103129314018852116
- LlovetJMRicciSMazzaferroVSHARP Investigators Study GroupSorafenib in advanced hepatocellular carcinomaN Engl J Med2008359437839018650514
- EscudierBEisenTStadlerWMTARGET Study GroupSorafenib in advanced clear-cell renal-cell carcinomaN Engl J Med2007356212513417215530
- SiegelinMDRaskettCMGilbertCARossAHAltieriDCSorafenib exerts anti-glioma activity in vitro and in vivoNeurosci Lett2010478316517020470863
- YangFBrownCBuettnerRSorafenib induces growth arrest and apoptosis of human glioblastoma cells through the dephosphorylation of signal transducers and activators of transcription 3Mol Cancer Ther20109495396220371721
- CarraEBarbieriFMarubbiDSorafenib selectively depletes human glioblastoma tumor-initiating cells from primary culturesCell Cycle201312349150023324350
- DenRBKamravaMShengZA phase I study of the combination of sorafenib with temozolomide and radiation therapy for the treatment of primary and recurrent high-grade gliomasInt J Radiat Oncol Biol Phys201385232132822687197
- HugHSarreTFProtein kinase C isoenzymes: divergence in signal transduction?Biochem J1993291Pt 23293438484714
- MusashiMOtaSShiroshitaNThe role of protein kinase C isoforms in cell proliferation and apoptosisInt J Hematol2000721121910979203
- PodarKTaiYTDaviesFEVascular endothelial growth factor triggers signaling cascades mediating multiple myeloma cell growth and migrationBlood200198242843511435313
- YoshijiHKuriyamaSWaysDKProtein kinase C lies on the signaling pathway for vascular endothelial growth factor-mediated tumor development and angiogenesisCancer Res199959174413441810485491
- GoekjianPGJirousekMRProtein kinase C inhibitors as novel anticancer drugsExpert Opin Investig Drugs2001101221172140
- TeicherBAAlvarezEMenonKAntiangiogenic effects of a protein kinase Cbeta-selective small moleculeCancer Chemother Pharmacol2002491697711855754
- KeyesKAMannLShermanMLY317615 decreases plasma VEGF levels in human tumor xenograft-bearing miceCancer Chemother Pharmacol200453213314014593497
- GraffJRMcNultyAMHannaKRThe protein kinase Cbeta-selective inhibitor, Enzastaurin (LY317615.HCl), suppresses signaling through the AKT pathway, induces apoptosis, and suppresses growth of human colon cancer and glioblastoma xenograftsCancer Res200565167462746916103100
- SpaldingACZeitlinBDWilder-RomansKEnzastaurin, an inhibitor of PKCbeta, enhances antiangiogenic effects and cytotoxicity of radiation against endothelial cellsTransl Oncol20081419520119043530
- WilleyCDXiaoDTuTEnzastaurin (LY317615), a protein kinase C beta selective inhibitor, enhances antiangiogenic effect of radiationInt J Radiat Oncol Biol Phys20107751518152619906497
- TabatabaiGFrankBWickASynergistic antiglioma activity of radiotherapy and enzastaurinAnn Neurol200761215316117212356
- ButowskiNChangSMLambornKREnzastaurin plus temozolomide with radiation therapy in glioblastoma multiforme: a phase I studyNeuro-oncology201012660861320156802
- ButowskiNChangSMLambornKRPhase II and pharmacogenomics study of enzastaurin plus temozolomide during and following radiation therapy in patients with newly diagnosed glioblastoma multiforme and gliosarcomaNeuro-oncology201113121331133821896554
- ChangSMLambornKRMalecMPhase II study of temozolomide and thalidomide with radiation therapy for newly diagnosed glioblastoma multiformeInt J Radiat Oncol Biol Phys200460235335715380566
- ButowskiNPradosMDLambornKRA phase II study of concurrent temozolomide and cis-retinoic acid with radiation for adult patients with newly diagnosed supratentorial glioblastomaInt J Radiat Oncol Biol Phys20056151454145915817350
- GingrasMCRousselEBrunerJMBranchCDMoserRPComparison of cell adhesion molecule expression between glioblastoma multiforme and autologous normal brain tissueJ Neuroimmunol1995571–21431537535788
- GladsonCLExpression of integrin alpha v beta 3 in small blood vessels of glioblastoma tumorsJ Neuropathol Exp Neurol19965511114311498939197
- HoodJDChereshDARole of integrins in cell invasion and migrationNat Rev Cancer2002229110012635172
- TakadaYYeXSimonSThe integrinsGenome Biol20078521517543136
- HuveneersSTruongHDanenHJIntegrins: signaling, disease, and therapyInt J Radiat Biol20078311–1274375117852562
- DesgrosellierJSChereshDAIntegrins in cancer: biological implications and therapeutic opportunitiesNat Rev Cancer201010192220029421
- AbdollahiAGriggsDWZieherHInhibition of alpha(v) beta3 integrin survival signaling enhances antiangiogenic and antitumor effects of radiotherapyClin Cancer Res200511176270627916144931
- NingSChenZDirksATargeting integrins and PI3K/Akt-mediated signal transduction pathways enhances radiation-induced anti-angiogenesisRadiat Res2007168112513317722999
- MonferranSSkuliNDelmasCAlphavbeta3 and alphavbeta5 integrins control glioma cell response to ionising radiation through ILK and RhoBInt J Cancer2008123235736418464290
- NingSNemethJAHansonRLForsytheKKnoxSJAnti-integrin monoclonal antibody CNTO 95 enhances the therapeutic efficacy of fractionated radiation therapy in vivoMol Cancer Ther2008761569157818566227
- NingSTianJMarshallDJKnoxSJAnti-alphav integrin monoclonal antibody intetumumab enhances the efficacy of radiation therapy and reduces metastasis of human cancer xenografts in nude ratsCancer Res201070197591759920841470
- GoodmanSLHölzemannGSulyokGAKesslerHNanomolar small molecule inhibitors for alphav(beta)6, alphav(beta)5, and alphav(beta)3 integrinsJ Med Chem20024551045105111855984
- BelvisiLRiccioniTMarcelliniMBiological and molecular properties of a new alpha(v)beta3/alpha(v)beta5 integrin antagonistMol Cancer Ther20054111670168016275988
- DechantsreiterMAPlankerEMathäBN-Methylated cyclic RGD peptides as highly active and selective alpha(V)beta(3) integrin antagonistsJ Med Chem199942163033304010447947
- AlvaASlovinSDaignaultSPhase II study of cilengitide (EMD 121974, NSC 707544) in patients with non-metastatic castration resistant prostate cancer, NCI-6735. A study by the DOD/PCF prostate cancer clinical trials consortiumInvest New Drugs201230274975721049281
- FriessHLangrehrJMOettleHA randomized multi-center phase II trial of the angiogenesis inhibitor Cilengitide (EMD 121974) and gemcitabine compared with gemcitabine alone in advanced unresectable pancreatic cancerBMC Cancer2006628517156477
- VermorkenJBGuigayJMesiaRPhase I/II trial of cilengitide with cetuximab, cisplatin and 5-fluorouracil in recurrent and/or metastatic squamous cell cancer of the head and neck: findings of the phase I partBr J Cancer2011104111691169621540865
- NaborsLBMikkelsenTRosenfieldSSPhase I and correlative biology study of cilengitide in patients with recurrent malignant gliomaJ Clin Oncol200725131651165717470857
- MacDonaldTJStewartCFKocakMPhase I clinical trial of cilengitide in children with refractory brain tumors: Pediatric Brain Tumor Consortium Study PBTC-012J Clin Oncol200826691992418281665
- ReardonDAFinkKLMikkelsenTRandomized phase II study of cilengitide, an integrin-targeting arginine-glycine-aspartic acid peptide, in recurrent glioblastoma multiformeJ Clin Oncol200826345610561718981465
- GilbertMRKuhnJLambornKRCilengitide in patients with recurrent glioblastoma: the results of NABTC 03-02, a phase II trial with measures of treatment deliveryJ Neurooncol2012106114715321739168
- AlbertJMCaoCGengLLeavittLHallahanDELuBIntegrin alpha v beta 3 antagonist Cilengitide enhances efficacy of radiotherapy in endothelial cell and non-small-cell lung cancer modelsInt J Radiat Oncol Biol Phys20066551536154316863930
- MikkelsenTBrodieCFinnissSRadiation sensitization of glioblastoma by cilengitide has unanticipated schedule-dependencyInt J Cancer2009124112719272719199360
- ClinicalTrials.gov [homepage on the Internet]ClinicalTrials.gov: A service of the US National Institutes of HealthBethesda, MDNational Institutes of Health Available from: http://www.clinicaltrials.govAccessed May 2013
- YardenYThe EGFR family and its ligands in human cancer. Signalling mechanisms and therapeutic opportunitiesEur J Cancer200137Suppl 4S3S811597398
- SalomonDSBrandtRCiardielloFNormannoNEpidermal growth factor-related peptides and their receptors in human malignanciesCrit Rev Oncol Hematol19951931832327612182
- LibermannTANusbaumHRRazonNAmplification and over-expression of the EGF receptor gene in primary human glioblastomasJ Cell Sci Suppl198531611723011820
- WongAJBignerSHBignerDDKinzlerKWHamiltonSRVogelsteinBIncreased expression of the epidermal growth factor receptor gene in malignant gliomas is invariably associated with gene amplificationProc Natl Acad Sci USA19878419689969033477813
- Lund-JohansenMBjerkvigRHumphreyPABignerSHBignerDDLaerumODEffect of epidermal growth factor on glioma cell growth, migration, and invasion in vitroCancer Res19905018603960442393868
- BarkerFGJrSimmonsMLChangSMEGFR overexpression and radiation response in glioblastoma multiformeInt J Radiat Oncol Biol Phys200151241041811567815
- HuangHSNaganeMKlingbeilCKThe enhanced tumorigenic activity of a mutant epidermal growth factor receptor common in human cancers is mediated by threshold levels of constitutive tyrosine phosphorylation and unattenuated signalingJ Biol Chem19972725292729359006938
- HeimbergerABHlatkyRSukiDPrognostic effect of epidermal growth factor receptor and EGFRvIII in glioblastoma multiforme patientsClin Cancer Res20051141462146615746047
- FeldkampMMLalaPLauNRoncariLGuhaAExpression of activated epidermal growth factor receptors, Ras-guanosine triphosphate, and mitogen-activated protein kinase in human glioblastoma multiforme specimensNeurosurgery19994561442145310598712
- LiuMYangYWangCThe effect of epidermal growth factor receptor variant III on glioma cell migration by stimulating ERK phosphorylation through the focal adhesion kinase signaling pathwayArch Biochem Biophys20105022899520650261
- LuKVZhuSCvrljevicAFyn and SRC are effectors of oncogenic epidermal growth factor receptor signaling in glioblastoma patientsCancer Res200969176889689819690143
- BonaviaRIndaMMVandenbergSEGFRvIII promotes glioma angiogenesis and growth through the NF-κB, interleukin-8 pathwayOncogene201231364054406622139077
- ChakravartiALoefflerJSDysonNJInsulin-like growth factor receptor I mediates resistance to anti-epidermal growth factor receptor therapy in primary human glioblastoma cells through continued activation of phosphoinositide 3-kinase signalingCancer Res200262120020711782378
- MendelsohnJBaselgaJEpidermal growth factor receptor targeting in cancerSemin Oncol200633436938516890793
- KimESHirshVMokTGefitinib versus docetaxel in previously treated non-small-cell lung cancer (INTEREST): a randomised phase III trialLancet200837296521809181819027483
- CappuzzoFCiuleanuTStelmakhLSATURN investigatorsErlotinib as maintenance treatment in advanced non-small-cell lung cancer: a multicentre, randomised, placebo-controlled phase 3 studyLancet Oncol201011652152920493771
- VickersMMPowellEDAsmisTRComorbidity, age and overall survival in patients with advanced pancreatic cancer – results from NCIC CTG PA.3: a phase III trial of gemcitabine plus erlotinib or placeboEur J Cancer201248101434144222119354
- van den BentMJBrandesAARamplingRRandomized phase II trial of erlotinib versus temozolomide or carmustine in recurrent glioblastoma: EORTC brain tumor group study 26034J Clin Oncol20092781268127419204207
- RichJNReardonDAPeeryTPhase II trial of gefitinib in recurrent glioblastomaJ Clin Oncol200422113314214638850
- BiancoCTortoraGBiancoREnhancement of antitumor activity of ionizing radiation by combined treatment with the selective epidermal growth factor receptor-tyrosine kinase inhibitor ZD1839 (Iressa)Clin Cancer Res20028103250325812374696
- ChinnaiyanPHuangSVallabhaneniGMechanisms of enhanced radiation response following epidermal growth factor receptor signaling inhibition by erlotinib (Tarceva)Cancer Res20056583328333515833866
- SarkariaJNCarlsonBLSchroederMAUse of an orthotopic xenograft model for assessing the effect of epidermal growth factor receptor amplification on glioblastoma radiation responseClin Cancer Res2006127 Pt 12264227116609043
- ChakravartiADickerAMehtaMThe contribution of epidermal growth factor receptor (EGFR) signaling pathway to radioresistance in human gliomas: a review of preclinical and correlative clinical dataInt J Radiat Oncol Biol Phys200458392793114967452
- HarariPMHuangSMEpidermal growth factor receptor modulation of radiation response: preclinical and clinical developmentSemin Radiat Oncol2002123 Suppl 2212612174341
- KrishnanSBrownPDBallmanKVNorth Central Cancer Treatment GroupPhase I trial of erlotinib with radiation therapy in patients with glioblastoma multiforme: results of North Central Cancer Treatment Group protocol N0177Int J Radiat Oncol Biol Phys20066541192119916626884
- BroniscerABakerSJStewartCFPhase I and pharmacokinetic studies of erlotinib administered concurrently with radiotherapy for children, adolescents, and young adults with high-grade gliomaClin Cancer Res200915270170719147777
- BrownPDKrishnanSSarkariaJNNorth Central Cancer Treatment Group Study N0177Phase I/II trial of erlotinib and temozolomide with radiation therapy in the treatment of newly diagnosed glioblastoma multiforme: North Central Cancer Treatment Group Study N0177J Clin Oncol200826345603560918955445
- SchwerALDamekDMKavanaghBDA phase I dose-escalation study of fractionated stereotactic radiosurgery in combination with gefitinib in patients with recurrent malignant gliomasInt J Radiat Oncol Biol Phys2008704993100117967517
- GeyerJRStewartCFKocakMA phase I and biology study of gefitinib and radiation in children with newly diagnosed brain stem gliomas or supratentorial malignant gliomasEur J Cancer201046183287329320708924
- PollackIFStewartCFKocakMA phase II study of gefitinib and irradiation in children with newly diagnosed brainstem gliomas: a report from the Pediatric Brain Tumor ConsortiumNeuro-oncology201113329029721292687
- ChakravartiAWangMRobinsHIRTOG 0211: a phase 1/2 study of radiation therapy with concurrent gefitinib for newly diagnosed glioblastoma patientsInt J Radiat Oncol Biol Phys20138551206121123182702
- NavéBTOuwensMWithersDJAlessiDRShepherdPRMammalian target of rapamycin is a direct target for protein kinase B: identification of a convergence point for opposing effects of insulin and amino-acid deficiency on protein translationBiochem J1999344Pt 242743110567225
- FingarDCSalamaSTsouCHarlowEBlenisJMammalian cell size is controlled by mTOR and its downstream targets S6K1 and 4EBP1/eIF4EGenes Dev200216121472148712080086
- ZhangSYuDPI(3)king apart PTEN’s role in cancerClin Cancer Res201016174325433020622047
- KhanKHYapTAYanLCunninghamDTargeting the PI3K-AKT-motor signaling network in cancerChim J cancer2013325253265
- FranzDNWeissBDMolecolar therapies for tuberous selerosis and neurofibromatosisCover Neurol Neurosci Rep2012123294302
- EshlemanJSCarlsonBLMladekACKastnerBDShideKLSarkariaJNInhibition of the mammalian target of rapamycin sensitizes U87 xenografts to fractionated radiation therapyCancer Res200262247291729712499272
- AnandharajACinghuSParkWYRapamycin-mediated mTOR inhibition attenuates survivin and sensitizes glioblastoma cells to radiation therapyActa Biochim Biophys Sin (Shanghai)201143429230021367753
- KimKWMutterRWCaoCAutophagy for cancer therapy through inhibition of pro-apoptotic proteins and mammalian target of rapamycin signalingJ Biol Chem200628148368833689017005556
- ShinoharaETCaoCNiermannKEnhanced radiation damage of tumor vasculature by mTOR inhibitorsOncogene200524355414542215940265
- SarkariaJNGalanisEWuWCombination of temsirolimus (CCI-779) with chemoradiation in newly diagnosed glioblastoma multiforme (GBM) (NCCTG trial N027D) is associated with increased infectious risksClin Cancer Res201016225573558020921209
- SarkariaJNGalanisEWuWNorth Central Cancer Treatment Group Phase I trial N057K of everolimus (RAD001) and temozolomide in combination with radiation therapy in patients with newly diagnosed glioblastoma multiformeInt J Radiat Oncol Biol Phys201181246847520864273