Abstract
Objective
We aimed to evaluate local tumor control after transarterial chemoembolization (TACE) for hepatocellular carcinoma using miriplatin and low-dose epirubicin combination therapy.
Methods
We retrospectively analyzed the records of patients who underwent TACE using miriplatin plus low-dose epirubicin (30 patients, 61 nodules, August 2011–March 2012) and control patients who underwent TACE using miriplatin alone (36 patients, 70 nodules, June 2010–July 2011). The local control rate was compared between the two groups using the Kaplan–Meier estimator and the log-rank test. Factors affecting local tumor recurrence were analyzed using multivariate logistic regression analysis. Treatment-related toxicity was evaluated using the Common Terminology Criteria for Adverse Events.
Results
The local control rates at 6 months and 1 year were 87% and 65% for the miriplatin plus low-dose epirubicin group, and 61% and 43% for the miriplatin group, respectively. Local tumor control rates were significantly better in the miriplatin plus low-dose epirubicin group than in the miriplatin group (P = 0.038). Multivariate analysis showed that the addition of epirubicin was an independent factor associated with better local tumor control (hazard ratio 0.2, P = 0.001). Overall incidence rates for adverse events were not significantly different between the two groups.
Conclusion
Additional usage of low-dose epirubicin for TACE using miriplatin improved local tumor control of hepatocellular carcinoma with adverse effects comparable to those observed with TACE using miriplatin alone.
Introduction
Transarterial chemoembolization (TACE) is an effective treatment for patients with unresectable hepatocellular carcinoma (HCC).Citation1–Citation3 Therapeutic efficacy depends on both sufficient accumulation of the chemotherapeutic agent at the target site and complete occlusion of tumor feeder vessels using the embolic material. Currently, different chemotherapeutic protocols are used for TACE in HCC, and determining which protocol is the most effective remains controversial.
Miriplatin (MPT; MIRIPLA®, Dainippon Sumitomo Pharma, Osaka, Japan), a third-generation platinum compound and anticancer drug, was first marketed in January 2010. Due to its high affinity for Lipiodol® (Lipiodol Ultrafluid, Terumo, Tokyo, Japan), once the MPT-Lipiodol suspension accumulates at the target tumor, it exerts a continuous antitumor effect through its gradual release from the tumor site. Furthermore, only mild systemic side effects are anticipated, as only trace amounts of the drug are expected to be released into systemic circulation.Citation4–Citation8 MPT also has the advantage of causing few adverse effects such as vascular damage or renal disturbance.Citation9,Citation10 However, local recurrence rates associated with TACE were reported to be higher when using MPT than when using epirubicin (EPI; Farmorubicin, Pfizer Japan, Tokyo, Japan) plus mitomycin or EPI alone.Citation11,Citation12 The inferior local control associated with MPT can be attributed to its reduced ability to induce vascular damage, higher viscosity, and slower release from the tumor.Citation11,Citation12 Concomitant use of vascular-toxic hydrophilic anticancer agents such as EPI is expected to enhance the therapeutic efficacy of MPT by compensating for these limitations.
This study was designed to assess whether combining MPT with low-dose EPI could increase the antitumor effect of MPT. In this regard, we retrospectively compared local tumor control rates between patients who had been treated with TACE using MPT plus low-dose EPI and those who had been treated with MPT alone.
Materials and methods
Patients
We enrolled 67 patients with unresectable HCC who underwent TACE using MPT with or without EPI between June 2010 and March 2012. Subjects were divided into two groups according to the anticancer drug(s) administered: 36 patients with 70 nodules were treated using MPT between June 2010 and July 2011 (MPT group), and 30 patients with 61 nodules were treated using MPT plus low-dose EPI between August 2011 and March 2012 (MPT + EPI group). Each patient was required to meet the following criteria: no previous treatment for the lesions under study, a total serum bilirubin level of <3 mg/dL, no portal venous thrombus in the main trunk, an interval of at least 4 weeks after the cessation of any previous anticancer therapy, and no more than five intrahepatic lesions. Subject nodules selected for treatment were enhanced in the arterial phase and washed out in the portal venous phase images of dynamic contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI). The diagnosis of HCC was confirmed by preprocedural CT or MRI findings as well as by intraprocedural angiography and cone-beam CT imaging findings, according to the American Association for Study of Liver Disease guidelines.Citation13,Citation14 Elevated levels of serum tumor markers were also considered for diagnosis. Tumor size was measured using cone-beam CT during TACE sessions. Comparative analysis was conducted for patient and tumor characteristics between the two groups. The TNM stage was classified according to the tumor staging system as revised by the Liver Cancer Study Group of Japan.Citation15 In this system, tumors are assigned a T factor according to the number and size of tumors and the location of invasion. A T1 classification refers to single tumors, ≤2 cm, and with no vascular or bile duct invasion. T2 tumors meet two of the above three criteria, T3 tumors meet one of these criteria, and T4 tumors do not meet any of the criteria.
The study protocol was approved by the Institutional Review Board of our hospital, and all patients provided informed written consent prior to TACE.
Drug preparation
The MPT preparation comprised 70 mg MPT suspended in 4 mL Lipiodol. For MPT plus low-dose EPI combination therapy, 10 mg EPI and 2 mL contrast agent (Iopamiron® 370; Bayer Schering Pharma, Osaka, Japan) were mixed with a suspension of 70 mg MPT and 4 mL Lipiodol. The upper limits set for MPT and EPI were 140 and 20 mg, respectively. Dosages were determined according to tumor size, treatment area, and patient liver function. All anticancer drugs were pumped 20 or more times in 5–10 mL doses with two syringes, using a three-way stopcock at room temperature.
Chemoembolization
All angiographic procedures were performed under a flat-panel detector cone-beam angiographic system (Innova® 3100; GE Healthcare, Waukesha, WI, USA) by two interventional radiologists, each with at least 10 years of experience. After inserting a 4-Fr catheter into the femoral artery, a 1.7–2.7-Fr microcatheter was advanced using the coaxial method into the tumor feeder vessel. The hepatic areas containing target tumors were subsequently infused with an appropriate dose of chemotherapeutic agents and embolized with 1–2 mm porous gelatin particles (Gelpart; Nippon Kayaku, Tokyo, Japan) until the tumor vessels were completely filled. Post-procedural C-arm CT images were obtained to ensure that no viable tumors or additional tumor feeder vessels remained.
Treatment evaluation
On the seventh day after TACE, unenhanced CT using a 16-slice CT scanner (Somatom Sensation; Siemens Medical Solutions, Forchheim, Germany) was performed to assess the accumulation of Lipiodol at the tumor. Dynamic contrast-enhanced CT or MRI was performed every 1–3 months to assess local recurrence for each nodule thereafter. Areas adjacent to the tumor that showed abnormal early enhancement with washout in the portal venous phase were considered to represent local recurrence. Newly appearing lesions at sites distant from the initially treated lesions were not considered local recurrence. The local tumor control rate was calculated from the date of TACE to the last date on which local recurrence was documented. The observation period was defined as the time from TACE to the last date on which local recurrence was documented or the last date on which the most recent CT/MR image was acquired.
Toxicity evaluation
Treatment-related adverse events were assessed according to the National Cancer Institute Common Terminology Criteria (version 4.0). Adverse events were evaluated as the maximum change in the grade within 4 weeks after therapy. The assessment factors included: fever; nausea; vomiting; pain; fatigue; increased levels of aspartate aminotransferase, alanine aminotransferase, serum amylase, total bilirubin, and creatinine; hypoalbuminemia; leukopenia; neutropenia; lymphopenia; eosinophilia; anemia; and thrombocytopenia.
Statistical analysis
We statistically compared the background profiles and adverse events between the two groups by using the Mann–Whitney U-test or the unpaired t-test. Local tumor control rates for the two groups of patients were compared using the Kaplan–Meier estimator with log-rank test. Factors affecting local tumor recurrence were assessed using multivariate and univariate analyses. Multivariate analysis was performed using the Cox proportional hazards model with a backward stepwise selection technique. All variables in univariate analysis were entered into multivariate analysis. All tests were two-sided, and difference levels of P < 0.05 were considered statistically significant.
Results
Among patient, tumor, and treatment background factors, significant differences were observed in the treatment area (P = 0.021). No significant differences were observed with respect to the other factors investigated (). The median follow-up duration was 279.5 days (range, 7–802 days) for the MPT group and 294 days (range, 6–498 days) for the MPT + EPI group.
Table 1 Patient, tumor, and treatment profiles
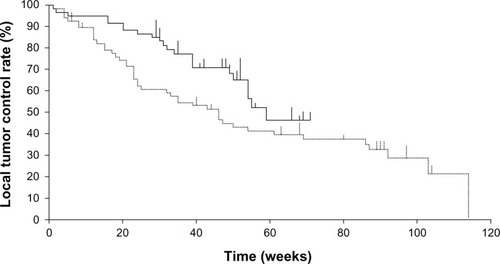
The overall local recurrence rate was 64% (45/70 nodules) for the MPT group and 36% (22/61 nodules) for the MPT + EPI group. The local tumor control rate at 6 months and 1 year was 61% and 43% for the MPT group and 87% and 65% for the MPT + EPI group, respectively. As shown in , local tumor control was significantly better in the MPT + EPI group than in the MPT group (P = 0.038).
Figure 1 Comparison of local control rates between the miriplatin plus low-dose epirubicin (solid line) and miriplatin (dotted line) groups in chemoembolization of hepatocellular carcinoma. The miriplatin plus low-dose epirubicin group showed significantly better local tumor control than the miriplatin group (P = 0.038).
Univariate analysis revealed that hepatitis B surface antigen positivity (P = 0.024), hepatitis C virus antibody negativity (P < 0.001), a serum α-fetoprotein level <20 ng/mL (P = 0.004), and additional EPI usage (P = 0.001) were significant factors associated with better local tumor control (). In multivariate analysis, additional EPI usage was an independent factor associated with the increased local tumor control rate (hazard ratio, 0.2; P = 0.001). A low local tumor control rate was associated with hepatitis C virus antigen positivity (hazard ratio, 4.0; P = 0.005) ().
Table 2 Univariate analysis of factors affecting local tumor recurrence after chemoembolization
Table 3 Multivariate analysis of factors affecting local tumor recurrence after chemoembolization
Treatment-related adverse events are shown in . No significant difference was found in the overall incidence rates for each adverse event investigated. The overall incidence rates of adverse events were 58% (213 events) and 60% (247 events) for the MPT + EPI and MPT groups, respectively. No significant differences were found in the overall incidence rate of adverse events between the two groups (P = 0.633). The incidence rates of severe adverse events (grade 3 or 4) were 4.4% (27 events) and 6.8% (42 events) in the MPT + EPI and MPT groups, respectively. No significant differences in the overall incidence rates of severe adverse events were found between the two groups (P = 0.063).
Table 4 Adverse events observed after chemoembolization
Discussion
Unlike other hydrophilic anticancer drugs, MPT can be easily dissolved in the carrier agent Lipiodol since it possesses lipophilic side chains. When the MPT-Lipiodol suspension accumulates at the tumor, gradual release of active platinum is expected over a prolonged period. However, the amount of active platinum released from an MPT suspension over a 28-day period is only 5.9% of the initial dose.Citation16 This observation suggests that MPT must be retained at the tumor site for a prolonged period of time in order to exert an adequate antitumor effect. Yanaihara et alCitation17 reported that initial CT accumulation rates are significantly lower after TACE using MPT than after TACE using EPI, whereas there was no significant difference in local control rates between both groups over a 1-year period when favorable Lipiodol accumulation had been observed on initial CT. This study indicates that favorable local tumor control could be achieved if MPT accumulates sufficiently within the tumor at initial TACE.
Methods for enhancing the accumulation of MPT have been addressed in several studies. Kora et alCitation18 and Seko et alCitation19 independently demonstrated that warming the MPT-Lipiodol suspension up to 40°C increased the therapeutic efficacy of TACE by reducing the viscosity of this chemotherapeutic agent. Indeed, experimental studies confirmed that the viscosity of the MPT suspension decreased as the temperature was elevated, thereby reducing injection pressure through a microcatheter.Citation20,Citation21 According to these studies, a lower viscosity of the MPT-Lipiodol suspension can enhance its distal delivery, thereby achieving sufficient initial accumulation of the agent in the target tumor.
Recently, Iwazawa et alCitation9 reported that more severe arterial damage was observed by using EPI than by using MPT in TACE for HCC. They concluded that therapeutic occlusion of tumor feeder vessels was associated with lower local recurrence. According to their observations, the use of vascular-toxic agents such as EPI can induce greater vascular occlusion of tumor feeder vessels. This leads to better local tumor control due to prolonged tumor ischemia. However, use of high-dose EPI can cause severe vascular alterations such as arterioportal shunting, intra- and extra-hepatic collateralizations, and aneurysm formation.Citation22 Such vascular complications may interfere with subsequent catheterization, thus compromising treatment success and clinical outcome.
Combination therapy of MPT with low-dose EPI in the treatment of HCC was first described by Iwazawa et al.Citation23 In short-term observation periods, they showed that TACE using MPT with low-dose EPI was associated with an increased objective response and comparable adverse effects compared with TACE using MPT alone. However, whether combination therapy with MPT and low-dose EPI actually improves long-term therapeutic efficacy compared with TACE using MPT alone has not yet been investigated. To our knowledge, the current study is the first to demonstrate that TACE using MPT plus low-dose EPI resulted in better local tumor control after 1 year than TACE using MPT alone.
There are several advantages to using low-dose EPI in combination with MPT during TACE. The addition of low-dose EPI may induce certain vascular injuries, thereby preventing early recanalization of the tumor feeder vessels. Long-term retention of the chemotherapeutic agents, initially accumulated at the tumor, can be anticipated by reducing arterial blood flow into the tumor. Furthermore, long-standing ischemia can also enhance the antitumor effect. Generally, oil suspensions have higher viscosity than water-in-oil emulsions. The viscosity of the MPT suspension may be higher than that of the MPT-EPI emulsion. In addition, we found that the oil droplets of the MPT-EPI emulsion delivered to the tumor were generally much smaller than those of the MPT suspension. The low viscosity and small chemotherapeutic droplets of the MPT-EPI emulsion may prevent the unintentional early occlusion of narrow tumor feeder vessels before the anticancer agents have completely filled in the entire tumor. EPI is a hydrophilic anticancer agent; therefore, a prompt antitumor effect just after therapy can be expected. Conversely, MPT retained at the target tumor site may exert prolonged antitumor activity by the gradual release of active platinum. Consequently, combined use of MPT and EPI is expected to result in complementary and long-lasting antitumor effects. Furthermore, compared with high-dose EPI, low-dose EPI used in a combination therapy can reduce vascular toxicity and preserve liver function, thereby providing patients with potential opportunities for future treatments.
There are limitations to this present study. First, the study was retrospective; thus, there may have been selection and information biases. Second, HCC was not histologically confirmed. All study lesions were diagnosed on the basis of imaging findings and elevated serum levels of tumor markers. Third, the sample size was fairly small. Study of a larger number of subjects may be necessary to confirm the current results. Fourth, chemoembolization was performed more distally on the MPT + EPI group than on the MPT group. This difference might have affected the local tumor control rate. Fifth, the observation period for the MPT + EPI group was relatively short. Longer-term observation might have produced a different outcome. Finally, the concomitant use of MPT and EPI in TACE may limit second-line drug options, when tumors become unresponsive.
Conclusion
Combination therapy using MPT plus low-dose EPI for TACE improved local tumor control in HCC patients with adverse effects comparable to those encountered on using TACE with MPT alone. Additional usage of EPI for TACE using MPT was an independent factor associated with better local tumor control in TACE for HCC.
Disclosure
The authors report no conflicts of interest in this work.
References
- YamadaRSatoMKawabataMNakatsukaHNakamuraKTakashimaSHepatic artery embolization in 120 patients with unresectable hepatomaRadiology198314823974016306721
- UchidaHOhishiHMatsuoNTranscatheter hepatic segmental arterial embolization using lipiodol mixed with an anticancer drug and Gelform particles for hepatocellular carcinomaCardiovacs Intervent Radiol1990133140145
- MatsuiOKadoyaMYoshikawaJSmall hepatocellular carcinoma: treatment with subsegmental transcatheter arterial embolizationRadiology1993188179838390073
- MaedaMUchidaNASasakiTLiposoluble platinum (II) complexes with antitumor activityJpn J Cancer Res19867765235253015851
- HanadaMBabaATsutsumishitaYIntra-hepatic arterial administration with miriplatin suspended in an oily lymphographic agent inhibits the grows of tumors implanted in rat livers by including platinum DNA adducts to form and massive apoptosisCancer Chemother Pharmacol200964347348319104812
- OkusakaTOkadaSNakanishiTFujiyamaSKuboYPhase II trial of intra-arterial chemotherapy using a novel lipophilic platinum derivative (SM-11355) in patients with hepatocellular carcinomaInvest New Drugs200422216917614739665
- ImaiNIkedaKKawamuraYTranscatheter arterial chemotherapy using miriplatin–lipiodol suspension with or without embolization for unresectable hepatocellular carcinomaJpn J Clin Oncol201242317518222210921
- OkabeKBeppuTHaraokaKSafety and short-term therapeutic effects of miriplatin-lipiodol suspension in transarterial chemoembolization (TACE) for hepatocellular carcinomaAnticancer Res20113192983298821868548
- IwazawaJHashimotoNOhueSMuramotoOMitaniTChemoembolization-induced arterial damage: evaluation of three different chemotherapeutic protocols using epirubicin and miriplatinHepatol Res Epub342013
- ImaiNIkedaKSekoYTranscatheter arterial chemotherapy with miriplatin for hepatocellular carcinoma patients with chronic renal failure: Report of three casesGut Liver20137224625123560163
- MiyayamaSYamashiroMShibataYComparison of local control effects of superselective transcatheter arterial chemoembolization using epirubicin plus mitomycin C and miriplatin for hepatocellular carcinomaJpn J Radiol201230326327022223074
- IwazawaJOhueSHashimotoNMitaniTLocal tumor progression following lipiodol-based targeted chemoembolization of hepatocellular carcinoma: a retrospective comparison of miriplatin and epirubicinCancer Manag Res2012411311922570565
- BruixJShermanMPractice Guidelines Committee, American Association for the Study of Liver DiseasesManagement of hepatocellular carcinomaHepatology20054251208123616250051
- BruixJShermanMAmerican Association for the Study of Liver DiseasesManagement of hepatocellular carcinoma: an updateHepatology20115331020102221374666
- MakuuchiMBelghitiJBelliGWorking Group of the International Scientific Committee of the International Hepato-Pancreato-Biliary AssociationIHPBA concordant classification of primary liver cancer: working group reportJ Hepatobiliary Pancreat Surg2003101263012918454
- KishimotoSNoguchiTYamaokaTFukushimaSTakeuchiYAntitumor effects of a novel lipophilic platinum complex (SM-11355) against a slowly-growing rat hepatic tumor after intra-hepatic arterial administrationBiol Pharm Bull200023334434810726891
- YanaiharaHTsunematsuSWoodhamsRMatsunagaKTsuchimotoKInoueY[Comparison between miriplatin and epirubicin in transcatheter arterial chemoembolization for hepatocellular carcinoma performed by a single operator.]Kitasato Medicine201242105109 Japanese
- KoraSUrakawaHMitsufujiTOsameAHigashiharaHYoshimitsuKWarming effect on miriplatin-lipiodol suspension as a chemotherapeutic agent for transarterial chemoembolization for hepatocellular carcinoma: preliminary clinical experienceCardiovasc Intervent Radiol20133641023102923238851
- SekoYIkedaKKawamuraYAntitumor efficacy of transcatheter arterial chemoembolization with warmed miriplatin in hepatocellular carcinomaHepatol Res Epub1272012
- KoraSUrakawaHMitsufujiTWarming effect on miriplatin-lipiodol suspension for potential use as a chemotherapeutic agent for transarterial chemoembolization of hepatocellular carcinoma: in vitro studyHepatol Res Epub12262012
- HasegawaTTakakiHYamanakaTExperimental assessment of temperature influence on miriplatin and cisplatin iodized-oil suspension viscosityJpn J Radiol201331642442723525952
- SueyoshiEHayashidaTSakamotoIUetaniMVascular complications of hepatic artery after transcatheter arterial chemoembolization in patients with hepatocellular carcinomaAJR Am J Roentgenol2010195124525120566824
- IwazawaJHashimotoNOhueSMitaniTInitial safety and outcomes of miriplatin plus low-dose epirubicin for transarterial chemoembolization of hepatocellular carcinomaAnticancer Res201232115039504423155276