
Abstract
The latest developments in precision medicine allow the modulation of therapeutic approaches in different pathologies on the basis of the specific molecular characterization of the patient. This review of the literature coupled with in silico analysis was to provide a selected screening of interactions between single-nucleotide polymorphisms (SNPs) and drugs (repurposed, investigational, and biological agents) showing efficacy and toxicityin counteracting Covid-19 infection. In silico analysis of genetic variants related to each drug was performed on such databases as PharmGKB, Ensembl Genome Browser, www.drugs.com, and SNPedia, with an extensive literature review of papers (to May 10, 2020) on Covid-19 treatments using Medline, Embase, International Pharmaceutical Abstracts, PharmGKB, and Google Scholar. The clinical relevance of SNPs, known as both drug targets and markers, considering genetic variations with known drug responses, and the therapeutic consequences are discussed. In the context of clinical treatment of Covid-19, including infection prevention, control measures, and supportive care, this review highlights the importance of a personalized approach in the final selection of therapy, which is probably essential in the management of the Covid-19 pandemic.
Introduction
Covid-19, an emergency all over the world, is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV2), a positive-sense RNA virus with higher mutation rates than DNA viruses.Citation1,Citation2 Laboratory tests on respiratory tract specimens (swab/saliva/tears PCR and serological tests) and computed tomography (CT; for chest or other tissue) should stage as soon as possible the presence of disease and its evolution/progression.Citation3,Citation4 SARS-CoV2 binds principally to the cell-membrane ACE2 receptor through the viral structural spike (S) protein, although other “virus doors” have been suggested (integrins and Toll-like receptors)Citation5 (). At the intracellular level, the virus activates cellular processes to produce viral proteins that replicate the virus’s genetic material, providing potential targets for drug therapy.Citation1,Citation5,Citation6
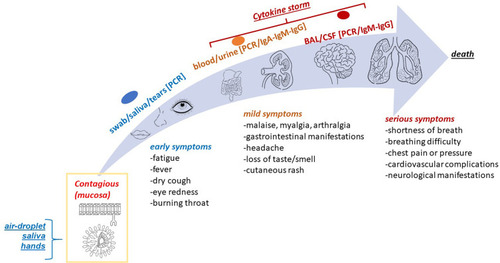
Figure 1 Overview of Covid-19 infection: SARS-CoV2–host interaction and tissue manifestation. Schematic representation of SARS-CoV2 virus interacting with mucosa epithelia (framed) and gradual sprouting to gut, kidney, brain, and lung tissue. “Virus doors” reportedwere ACE2, integrin, TLR3, or TMPRSS2. Overall symptoms are listed. Briefly, most common Covid-19 symptoms occur at the upper respiratory tract, together with asthenia and general malaise. Early, less common clinical features include gastrointestinal symptoms (nausea, anorexia, diarrhea), anosmia and dysgeusia. Severe cases encompass pneumonia or bronchopneumonia, severe acute respiratory syndrome, renal failure, up to death. The lower respiratory tract participation and complications are more frequent in people aged over 50 with pre-existing chronic diseases of cardiovascular and/or respiratory system, as well as some autoimmune diseases (diabetes). Cardiac involvement represents another potentially life-threatening complication, caused by direct viral damage, hypoxic injury, microvascular dysfunction and disclosing with diverse clinical pictures (arrhythmias, myocarditis, and heart failure). Finally, virus can reach central nervous system causing central (acute cerebrovascular diseases, impairment of consciousness) and peripheral complications. The evolution of infection from early detection severe complications and death (shaded arrow). As reported, molecular and serological, as well as imaging tests, are useful depending on disease evolution: real-time PCR applied to nasopharyngeal swabs, venous blood as well as conjunctival swabs can track disease ongoing, while early-released IgM and late-released IgG might assess for immune response, in line with cytokine storm panel (IL6, TNFα, IFNγ, and IL10) typifying tissue/organ complications.
SARS-CoV2 Infection and Main Clinical Aspects
Covid-19 features, diagnostic route, and early, mild, and severe Covid-19 symptoms are summarized in . Virus entry and multiple signaling pathways (Ca2+ release, cSrc, FAK, MAPK, and PI3K) occur upon Spike2–RGD–integrin interaction.Citation7 A “cytokine storm” is locally released (IL1β, IL6, IL8, TNFα, MIP1α, and VEGF), as first observed in patients showing fatal complications.Citation5 This specific panel was used to screen patients requiring prompt intervention to avoid acute respiratory distress syndrome (ARDS).Citation6 In a recent study, candidate drug targets for nonstructural proteins (3-chymotrypsin–like protease, papain-like protease, RNA-dependent RNA polymerase), viral access, and related immuno regulatory pathways have been prospected for evaluation.Citation6,Citation8,Citation9 A wide range of pulmonary manifestations can be observed, varying from mild respiratory symptoms (cough or sore throat) to severe pneumonia, up to a sudden development of respiratory failure.Citation10 Silent hypoxemia is a peculiar aspect frequent in frail and elderly patients that usually precedes the onset of an overt acute and severe respiratory syndrome.Citation11,Citation12 Chest CT imaging is strongly recommended for an early diagnosis of novel coronavirus pneumonia.Citation13,Citation14 CT findings, including patterns associated with less frequent signs, eg, lobular, bronchial, pleural, and subpleural involvement, as well as pleural lymphadenopathy and pericardial effusion, have been described.Citation15 SARS-CoV2 initially causes airspace exudates, interstitial edema, hyaline membranes, and inflammatory infiltrates in the alveoli.Citation16 Other than the deleterious lung effects, systemic SARS-CoV2 has a significant impact on the hematopoietic system and tissue homeostasis.Citation17 Initially, lymphopenia showed interesting prognostic value, for both neutrophil:lymphocyte and platelet:lymphocyte ratios in severe SARS-CoV2 cases. Lymphocyte parameters (count dynamics), some inflammatory indices (LDH, CRP, and IL6), and some recent circulating biomarkers (high serum procalcitonin and ferritin) have been suggested for identifying cases with poor prognosis (prompt intervention and improved outcomes). As observed, blood hypercoagulability, high D-dimer levels (particularly associated with disease worsening), protraction of both prothrombin (PT) time, activated partial thromboplastin time (aPTT), and disseminated intravascular coagulation require constant surveillance to allow prompt intervention. In addition to upper-airway contact, conjunctivitis may be an ocular manifestation of SARS-CoV2 infection, if quickly detected.Citation18 In December 2019, a Chinese ophthalmologist reported an unusual viral conjunctivitis. To date, several Internet articles and scientific reports have documented the potential use of eye swabs as a tool to screen virus infection, although contrasting data are available, most probably related to progression of infection and virus detection.Citation19 In January 2020, a worldwide expert in infectious diseases referred to conjunctivitis during an inspection of Wuhan and tested positive for SARS-CoV2, but quickly recovered from infection. This led to the idea of “eye infection” as a possible alternative route of SARS-CoV2 transmission, alternative to the respiratory one.Citation20 Ocular secretion might represent a reservoir of virus at the early stages of contagious.Citation18 When pinkeye occurs as a sign of conjunctivitis, a differential diagnosis can be of great utility to screen symptomatic and even presymptomatic individuals.Citation21
Genetic Background, Individual Responses, and SNP Association
Recently, pharmacogenomics (the effects of a single genetic marker) and pharmacogenetics (the collective influence of variability across the genome to modulate an individual’s drug response) have received great attention for their abilities to provide a new way to select drugs for personalized therapy (optimal dosing for maximizing drug efficacy or minimizing the risk of toxicity).Citation22,Citation23 Through drug therapy, pharmacogenetics might influence both pharmacokinetics and pharmacodynamics with respect to dosing, formulation sensitivity, and adverse drug reactions (ADRs), as well as drug-hypersensitivity reactions (allergic, pseudoallergic, and exaggerated pharmacological reactions to medications), determining an enhanced immunologic reaction or inflammatory response (side effects).Citation24 Genetic assessment can predict the occurrence of drug-related toxic effects. Single-nucleotide polymorphisms (SNPs) are the most common type of polymorphism found in the human genome, and represent the main reason for 90% of all types of genetic variations among individuals. An example of an ADR is the hypersensitivity reaction occurring in SNP carriers of the HLA-B*5701 allele who receive the antiviral abacavir for treatment of HIV.Citation25,Citation26 Covid-19 therapy is wide-ranging and multiple, and risk factors for ADRs can occur. Therefore, optimal doses, duration of treatment, side effects. and long-term outcomes are critical aspects of Covid-19 therapy.Citation27 CoV-mediated inflammation may be counteracted by anti-inflammatory cytokines, including IL1 family members, IL6, and TNFα.Citation28 Since no specific drug/therapy for Covid-19 treatment has been US Food and Drug Administration (FDA)-approved, an array of drugs approved for other diseases and under investigation (including off-label and biological drugs) have been included in clinical trials.Citation29,Citation30 As observed, the metabolic pathways of these drugs included various polymorphic cytochrome P450 enzymes, strongly suggesting genotyping for the CYP2D6*2, CYP2D6*3, CYP2D6*4, and CYP2D6*10 alleles.Citation31,Citation32 As an example, no predictability in the metabolic function of the CYP3A5*3 allele can result in alternative mRNA splicing with a trunked protein, due to the formation of an untimely stop codon. Moreover, haplotype CYP3A5*3 has been related to a reduced clearance of both ritonavir and lopinavir (substrates) (). Of interest is the association between polymorphisms inABCC and therapy efficacy, as the drug transporters are one of the primary mechanisms related to subtherapeutic antiretroviral-drug concentrations.Citation33 Prominent research has highlighted the relationship between the ABCB1 polymorphism (3435 C>T) and hepatotoxicity risk after antiviral treatments, and few additional studies were found regarding other nucleoside analogues.Citation33 More recently, the presence of grade 3–4 hyperbilirubinemia is directly proportional to the homozygosity, heterozygosity, and wild-type genotyping for the UGT1A1*28 allele in patients who receive ritonavir and lopinavir.Citation34 Therefore, the attempt of this literature review coupled with in silico analysis was to provide a selected screening of drugs showing efficacy and toxicity effects useful for counteracting Covid-19 infection.
Table 1 The Most Promising and Repurposed Drugs
Methods
An extensive literature review of papers published until May 10, 2020 was performed based on a standard procedure (Medline, Embase, International Pharmaceutical Abstracts, PharmGKB. and Google Scholar).Citation35 Search terms were “Covid-19”, “novel coronavirus”, “SARS-CoV2”, “pharmacogenetics”, “treatment/s”, “adverse side effects”, “therapy”, “lung”, “ocular”, “pulmonary infection”, “drugs”, “drug response”, “virus”, “candidate drugs”, “potential inhibitors”, “protease inhibitors”, “personalized medicine”, “individual therapy”, “pneumonia”, “ACE”, “heparin”, “vasculitis”, “conjunctivitis”, “rhinitis”, “hematological complication” and “main metabolic routes”, either alone or in combination. From this manually performed analysis, drugs reported in at least two studies or in a clinical trial were included. Ongoing clinical trials and the index of studies of Covid-19 were identified using the search term “coronavirus infection” on ClinicalTrials.gov and the Chinese Clinical Trial Registry (http://www/chictr.org/enindex.aspx). In silico analysis of genetic variants related to each drug was performed on dedicated databases, such as PharmGKB (), Ensembl Genome Browser, www.drugs.com, and SNPedia. The allelic frequency of each variant average in all populations was based on data from the 1000 Genomes Project phase 3. We considered SNPs related to both efficacy and toxicity response with allele frequencies ≥5%, as already described in previous studies.Citation36,Citation37 The quality of each study was assured, and resulting information included study design, baseline characteristics of disease, treatment regimens, and allelic frequencies of the genetic variant.
Table 2 Overview of PharmGKB
Results
Drugs in use as routine therapy or in clinical trials for Covid-19 include steroids and antiviral and biological humanized neutralizing antibodies against some proinflammatory cytokines, such as IL1, IL6, IFN, and TNFα, in addition to supportive measures and symptomatic treatment, according to the severity of the disease.Citation38 Data analysis on registered clinical trials of Covid-19 in the US is available at https://clinicaltrials.gov. Nowadays, a great number of agents have been evaluated for potential use in Covid-19 management, and only a fewhave been included within international and/or local protocols.Citation38 According to the US National Institutes of Health, no pharmacological agent has earned approval for safe and effective use yet, mainly because of the lack of evidence in favor or against these agents (https://covid19treatmentguidelines.nih.gov). One important aspect of a therapeutic approach consists in the choice of the right drugs throughout the natural history of disease. Indeed, a three-phase pathogenetic model has been proposed, with different clinical and laboratory features, each requiring a specific treatment based on the changing role over time,of direct viral damage and host inflammatory response in the disease course. This model describes an early stage (stage I), coinciding with incubation and/or mild flulike symptoms, during which antiviral drugs might reach high effectiveness, a moderate stage (stage II) characterized by pulmonary involvement without IIa or with IIb hypoxia, which may benefit from the use of antivirals and anti-inflammatory therapy (including steroids), and lastly a severe stage (stage III), in which a dysregulated, systemic hyperinflammatory response takes place, thus requiring the administration of immunomodulating agents, several of which are currently under investigation, and in some cases already in use within management protocols.Citation37
Gene variants associated with pharmacological responses to drugs are reported in a dedicated database — PharmGKB (https://www.pharmgkb.org) — allowing the identification of relationships between genetic variations (eg, SNPs, indels, repeats, haplotypes) and individual drug responsiveness.Citation40,Citation41 Herein, in silico pharmacogenetic analysis shows the potential clinical efficacy and/or toxicity of the major drugs selected for Covid-19 treatment. The main drugs proposed for Covid-19 treatments and reference sequence (rs) related to ADRs and efficacy are shown in . Genes and related SNPs (rs) associated with drug effects and their study annotation are summarized in .Citation42–Citation64 Major clinical information regarding “variant drug” responsiveness (clinical annotations) is highlighted. Bloodstream fluidity requires a tidy balance among factors favoring flow of blood and thrombosis. Any modification in this physiological balance triggers pathological conditions: deficit of coagulation factors favor bleeding, while genetic mutations of coagulation factors can determine a thrombotic risk framework characterized by differences in genetic variants of coagulation (). All drugs used as therapeutic options and their study annotation based on pharmacogenetic data are discussed.
Table 3 List of Genes and Reference SNPs (Rs: Reference Sequences) Associated with Drug Effects. Study Annotation Based on Data from Pharmgkb.org HGVS: Human Genome Variation Society (http://varnomen.hgvs.org)
Table 4 List of Coagulation Factors with Relative Protein Localization, Pathway, Function, Nucleotide Variants, and Reference SNPs (Reference Sequences) Involved in Thrombophilic Disorders
The Most Promising and Repurposed Drugs
Chloroquine (Cq) and Hydroxychloroquine (Hcq)
Cq is used for chemoprophylaxis of malaria and amebiasis, while Hcq is used to treat autoimmune disease.Citation8 The mechanism of action includes the blocking of viral entry through the inhibition of glycosylation of host receptors, proteolytic processing, and endosomal acidification.Citation65 Effects of immunomodulation on cytokine production and inhibition of autophagy/lysosomal activity have been also reported.Citation65–Citation67 Several randomized controlled trials (RCTs) are currently investigating Cq and Hcq in Covid-19 treatment (https://clinicaltrials.gov). Based on current data, both drugs are recommended for treatment of unhospitalized Covid-19 patients, and the effects of cardiotoxicity in immunosuppressed subjects or patients with kidney or liver problems are known. Recommendations for oral administration in Covid-19 treatment are 500 mg twice a day and 400 mg twice a day, followed by 200 mg twice a day for Cq and Hcq, respectively.Citation68 Blood monitoring is required, as hemolytic anemia might occur, particularly when the drug is delivered in association with other drugs that cause hemolysis.Citation69 It should not to be underestimated the extent to which both drugs may cause hemolysis in glucose-6-phosphate dehydrogenase (G6PD)-deficient individuals. Of note, about 39% of Covid-19 patients suffering from lupus have failed to respond or were even intolerant to Hcq.Citation70 Moreover, long-term Cq–Hcq treatment induces retinal toxicity, and particularly when Hcq-related retinopathy is diagnosed, the retinal damage endures, even after cessation of therapy.Citation71 High doses or prolonged administration of Hcq, even at recommended doses, may increase the risk of ocular toxicity (paracentral scotomas, color-vision changes, corneal/ciliary body/conjunctival as well as retinal abnormalities), and visual disturbances (retinal and macular toxicity).Citation72 This would imply that accurate eye screening for confirming SARS-CoV2 presence in early conjunctivitis or monitoring ocular structure during Covid-19 therapy is recommended to counteract early or even prevent eventual signs of ocular drug toxicity, including the retinopathy.Citation73
Lopinavir/Ritonavir
The oral combination of these two agents (FDA-approved and currently authorised as anti-HIV medicine) demonstrate activity against other novel coronaviruses.Citation74,Citation75 Several RCTs examining lopinavir/ritonavir in Covid-19 are in progress.Citation76 Recommendations for administration in Covid-19 treatment is 400 mg/100 mg twice daily for up to 14 days.Citation77 Adverse effects of lopinavir/ritonavir include several gastrointestinal complains, such as nausea, vomiting, and diarrhea, and hepatotoxicity, pancreatitis, and cardiac conduction abnormalities.Citation78 These adverse effects are increased in 20%–30% of Covid-19 patients with elevated transaminases.Citation79 Previous studies have shown that these ADRs with lopinavir–ritonavir combination are related to several polymorphisms present in the genes UGT1A1, UGT1A7, APOE, and APOC3 ().
Ribavirin
This antiviral drug (guanine analogue) inhibits viral RNA–dependent RNA polymerase. Ribavirin activity against Covid-19 disease is limited and requires high doses or combination therapy to be effective in humans. No evidence exists for inhaled ribavirin for Covid-19 treatment — no benefit over enteral or intravenous administrationCitation79 — though several studies have demonstrated possible harm due to adverse effects (hematologic and liver toxicity).Citation80 Ribavirin causes severe dose-dependent hematologic toxicity.Citation81 The inconclusive efficacy and toxicity results suggest that ribavirin has limited value in treatment of Covid-19. Case–control pharmacogenetic association studies indicate different polymorphisms in the ITPA, VDR, and SLC28A2 genes that are related to toxicity and adverse effects, while an increased pharmacological response is associated when some variants of the VDR, SLC29A1, IFNL3, and MICB–OASL genes are present. It must be noted that numerous studies have undertaken pharmacogenetic evaluations on populations undergoing ribavirin therapy combined with PEG-IFNα.Citation82
Umifenovir
This is an antiviral agent that exerts a mechanism of action targeting the S protein–ACE2 interaction, inhibiting membrane fusion of the viral envelope.Citation83 The recommendation for umifenovir oral dose (200 mg every 8 hours, 7–14 days) for influenza treatment was studied for Covid-19 therapy (NCT04260594). In Covid-19 patients treated with umifenovir, adverse effects include allergic-reaction gastrointestinal upset and elevated transaminases, although there are no studies that describe an association of these episodes with genetic variants.Citation27,Citation83
Miscellaneous Agents
IFNα/β
IFNα and -β have been studied for novel CoVs.Citation84 Several studies reported clinical outcomes in combination with ribavirin and/or lopinavir/ritonavir.Citation85 Adverse effects have been described in almost every organ, clearly dose-dependent.Citation84,Citation85 Several toxic mechanisms for IFNα/β have been investigated in recent years. Much remains still to be elucidated, although most side effects disappear on dose reduction or interruption of treatment. Previous genome-wide association studies on the response to IFNβ in neurological degenerative diseases suggest an increase in therapeutic response with the presence of several SNPs in the genes CD58, ZNF697, and FHIT. In parallel, ADRs have been observed with the presence of variants of the GAPVD1 and IRF6 genes. As of now, the use of interferons to treat Covid-19 disease is controversial.Citation86
Nitazoxanide/Camostat Mesylate
Although an antihelminthic agent, nitazoxanide has shown antiviral activity with a favorable safety profile.Citation87,Citation88 Camostat mesylate prevents novel CoV–cell entry through inhibition of the host surface transmembrane protease/serine (TMPRSS2), as observed by in vitro studies.Citation89 Neither drug has pharmacogenetic studies regarding efficacy or toxicity effects associated with genetic variants.
Azithromycin
This macrolide antibiotic is used extensively in patients with viral infections to prevent severe respiratory tract infections. Azithromycin–Hcq combination shows a synergistic effect on Covid-19 disease in vitro at concentrations comparable with that observed in human lung,Citation90 and has been found useful in combination with remdesivir, lopinavir/ritonavir and IFNβ. To date, the interaction between this macrolide and genetic factors is unknown. However, due to the potential risk of prolonged QT interval, remarkably increased by the mutual interaction between these two agents, their concomitant use is not recommended by several guidelines, unless within the setting of controlled trials (https://covid19treatmentguidelines.nih.gov).
Low Molecular–Weight Heparin
This anticoagulant is used to reduce thromboembolic events in patients with Covid-19 infection. As known, the SARS-CoV2 pandemic is characterized by the development of ARDS that results from acute inflammation within the alveolar space and prevention of normal gas exchange. Indeed, huge deposits of fibrin in the lung parenchyma and air spaces have been reported. The raising of proinflammatory cytokines within the lung leads to recruitment of leukocytes, increasing the local inflammatory response, and since the coagulation route contributes to reducing pathogen invasion by improving compartmentalization, this anticoagulant treatment has potential risk in those Covid-19 patients with no significant coagulopathy. The drug enoxaparin can be started as soon as the day of Covid-19 diagnosis and continued over 14 days, after baseline assessment and monitoring of PT, aPTT, complete blood-cell count, and creatinine levels. Clinical aggravation causing worsening and death in Covid-19 inpatients appears to be thrombotic. Therefore, special attention should be devoted to both risks and benefits of using heparin in Covid-19 patients. Prescreening is essential to highlight genetic predisposition related to thrombophilia, as these subjects with thrombophilic mutations (based on the degree found) are at greater risk of thrombotic complications.
Investigational Drugs
Remdesivir
This is an RNA-polymerase inhibitor (GS-5734), a retroviral drug belonging to the class of nucleotide analogues, and a monophosphate prodrug that was discovered during a screening study of antimicrobials with antiviral activity, showing promise against the Ebola virus.Citation91,Citation92 Recently approved by the FDA for the treatment of patients with Covid-19, remdesivir is recommended as a single 200 mg dose, followed by 100 mg daily infusion.Citation93 Besides the drug’s clinical use in the treatment of Ebola, several clinical trials are ongoing to evaluate the antiviral activity of remdesivir in patients with Covid-19 (NCT04292899, NCT04292730, NCT04257656, NCT04252664, and NCT04280705).Citation91 No pharmacogenetic indications are present, allowing modulation of dosage for therapy. Due to its toxicity, remdesivir is not currently FDA-approved, and must be obtained via compassionate use, expanded access, or enrollment in a clinical trial.
Favipiravir
Favipiravir ribofuranosyl-5′-triphosphate is a retroviral drug acting as an inhibitor of viral replication (RNA-polymerase inhibitor T705). This agent demonstrates broad activity against Ebola infection and other RNA viruses.Citation94 Favipiravir is recommended at a dose of 2,400–3,000 mg every 12 hours (two doses) followed by maintenance doses of 1,200–1,800 mg every 12 hours. Favipiravir is overall well tolerated, although a mild adverse-event profile for higher-dose regimens has been observed.Citation95–Citation97 The high doses used result in hyperuricemia, diarrhea, elevated transaminases, and reduction in neutrophil count, but nothing is known about any pharmacogenetic correlations. Favipiravir presents efficacy in the treatment of Covid-19 disease, but to date limited clinical experience has reported support for its use. No pharmacogenetic indications are present, allowing modulation of dosage for therapy using this drug.
Atazanavir and Darunavir
These drugs are well-known protease inhibitors used for the treatment of AIDS, with good efficacy and safety profiles. While atazanavir is combined with other antiretrovirals, darunavir is used in a fixed-dose combination with cobicistat, a new pharmacokinetic enhancer. With respect to the other protease inhibitors, atazanavir is less likely to cause lipodystrophy and is preferentially used in combination with other antiviral agents (ritonavir), providing antiviral potency equivalent to lopinavir, although concomitant use of ritonavir decreases the efficacy of atazanavir. Valid pharmacogenetic correlations of the efficacy of these antivirals can be deduced from studies carried out on HIV patients in which the efficacy of polymorphisms in the UGT1A1, CYP3A4, CYP3A5, and SLCO3A1 genes has been demonstrated. In contrast, cases of toxicity and ADRs are related to sequence variants in the UGT1A1, UGT1A7, UGT1A3, APOE, and APOC3 genes.Citation44–Citation48,Citation51,Citation55,Citation56,Citation98 In some settings, darunavir–cobicistat may be used in the presence of tolerability or availability of the lopinavir–ritonavir combination (https://covid19treatmentguidelines.nih.gov). Concerning the metabolism of Azatavir, the variants CYP3A5*1, CYP3A5*3, CYP3A5*6, CYP3A5*7 in CYP3A5 (rs776746) have been reported. Briefly, individuals carrying one or two copies of the *1 allele may metabolize atazanavir more rapidly than individuals with one or more copies of the *3, *6, or *7 alleles.Citation98
Adjunctive Experimental Therapies
Anticytokine or Immunomodulatory Agents (Tocilizumab, Sarilumab, and Bevacizumab)
Monoclonal antibodies directed against key inflammatory cytokines represent another potential class of adjunctive anti–Covid-19 therapies.Citation99,Citation100 IL6 is a key driver of this dysregulated inflammation.Citation100 The use of monoclonal antibodies against IL6 shows a dampening of this process and improves clinical outcomes. Tocilizumab, a monoclonal antibody IL6-receptor antagonist, is used in severe Covid-19 cases with success. Adult doses are 400 mg or 8 mg/kgin one or two doses, with second dose 8–12 hours after the first if response is inadequate.Citation101 Sarilumab is another IL6-receptor antagonist approved for rheumatoid arthritis. It is being studied in multiple centers for hospitalized patients with severe Covid-19 (NCT04315298; www.news.sanofi.us/2020-03-16-Sanofi-and-Regeneron-begin-global-Kevzara-R-sarilumabclinical-trial-program-in-patients-with-severe-COVID-19). Other monoclonal antibodies or immunomodulatory agents in several clinical trials are available for expanded access, such as bevacizumab (anti-VEGF medication; NCT04275414), fingolimod (immunomodulator approved for multiple sclerosis; NCT04280588) and eculizumab (antibody inhibiting terminal complement; NCT04288713). ADRs have been reported in subjects carrying variants in the IL6R, CD69, FCGR3, and GALNT18 genes.
Corticosteroids (Hydrocortisone, Prednisolone/Methylprednisolone, and Dexamethasone)
Corticosteroids are used to reduce lung inflammatory responses that in many cases evolve into acute lung injury and ARDS. At present, the effects of corticosteroids in patients affected by Covid-19 have been poorly described, so our considerations are based on observations in other viral pneumonia types, such as SARS and MERS.Citation102 These previous studies do not indicate any association between corticosteroid use and increased survival, but slower viral clearance in the respiratory and blood tracts, hyperglycemia (high blood sugar), vascular necrosis, and psychotic episodes.Citation103 Data are still unclear in patients with SARS-CoV2 infection. Although it remains controversial, the possibility of using corticosteroid treatment in patients with moderate or severe ARDS can be useful to reduce mortality. Low (ie, 25 mg/day) and moderate (ie, 140 mg/day) doses of corticosteroids reduce mortality in patients with acquired pneumonia,Citation104 but at present the risk of secondary infections, excessive persistence of viral load, and long-term complications using high-dose corticosteroids cannot be excluded. Dexamethasone is a potent CYP3A4 inducer. To date, the main studies on the pharmacogenetic aspects of steroid drugs have indicated a correlation between adverse events and variants of the ATF5, MIR3683, CTNNB1, and PNPLA3 genes.Citation61–Citation63
ACE Inhibitors
As stated, SARS-CoV2 has the ability to introduce and infect the host cell using the ACE2 receptor.Citation5 This has alarmed several researchers, who hypothesized how ACE inhibitors and angiotensin-receptor blockers could interfere negatively or positively with the viral infection process.Citation89,Citation105 Since ACE inhibitors upregulate ACE2 receptors, possible worsening of disease under ACE inhibitor therapy has been hypothesized. By contrary, angiotensin-receptor blockers could theoretically prevent the entry of the virus at the cellular level.Citation106 Some RCTs specific for captopril used alone or in combination in patients with Covid-19 with severe pneumonia are currently under investigation in order to understand ARDS (NCT04355429, https://clinicaltrials.gov). Since ACE inhibitors are among the most frequently used drugs in medical practice, consequent knowledge on related pharmacogenetic aspects is now widely known. The polymorphisms that modulate the activity of these drugs in ACE, ACE2, and AGTR1 genes have been widely studied and described in several recent studies.
Discussion
The Covid-19 pandemic is due to the novel pathogenic coronavirus SARS-CoV2, which emerged in China and spread quickly worldwide.Citation1,Citation2 Therapeutic options for Covid-19 are wide-ranging, and some drugs have gained emergency-use authorization from the FDA and/or European Medicines Agency. At present, patients are treated with symptomatic therapy and vital support in severe cases. Several international efforts are aimed at the investigation and development of antiviral agents, other immunotherapies, and vaccine strategies. Pharmacogenomics might be a promising tool in the development of more appropriate therapies (including drug management) and the prevention of fatal-complication onset due to ADRs.Citation27 Pharmacogenomics can predict from the beginning the effect of a specific drug formulation in terms of efficacy/toxicity with respect to individual genetic background and minimize exposure to drugs potentially less/ineffective other than toxic (precision medicine).Citation22,Citation23 As known, drug formulations can elicit different cell/tissue responses depending on individual genetic background. This is possible because each subject can have variations in nucleotide sequences belonging to genes encoding for enzymes involved in the activity of the drug that has been considered for therapy.Citation22–Citation24 This aspect appears of great importance in patients having several comorbidities or simply “fragile” old patients.
As there is no specific cure for Covid-19, we reviewed all the therapies (drugs) actually in use to counteract SARS-CoV2 effects and the related adverse effects to certain drugs (antiviral, antimalarial, and several biological humanized agents able to reduce the levels of some cytokines belonging to the cytokine storm), as reported by RCTs.Citation29–Citation34,Citation38–Citation41 Response to these drugs was extremely complex, and numerous cases of toxicities and antiretroviral drug resistance (viral mutations) have been reported.Citation38 A possible explanation of this variability might be the presence of factors that modify pharmacokinetics/pharmacodynamics and the activity of the virus itself (viral pharmacodynamics).Citation40 In addition, viral pharmacodynamics and mutagenesis are still unclear with regard to Covid-19 drug resistance.Citation38
Genetic factors might account at least in part for the unpredictability of therapy among Covid-19 patients.Citation38 Merely, a significant number of SNPs in genes encoding proteins implicated in the transport and metabolization of drugs may be responsible for the wide variability in drug pharmacokinetics and toxicity.Citation32 Consistently, this review, coupled with a wide in silico analysis on the relevance of identification of SNPs involved in drug metabolism, provides a list of specific drug-associated SNPs associated with efficacy (green) or toxicity (red), useful in predicting individual response to therapy in Covid-19 patients. This would imply the possibility of checking variants in biological samples collected and evaluated before the beginning of therapy with the aim of predicting the outcome of a single or combined Covid-19 therapy. To our knowledge, although a considerable number of ADR episodes in Covid-19 patients have to date been described in the literature, there has been no pharmacogenetic study attempting to correlate the clinical outcomes of drug treatment with gene variants.Citation27 The identification of gene variants is only the first step in a complex process prior to applicability into clinical practice. In fact, the clinical application of pharmacogenetic analysis requires previous studies confirming its validity and usefulness. To support this, essential measures applied to genetic tests are required: analytical and clinical validity and clinical utility. While analytical validity defines test accuracy, sensitivity, and specificity, guaranteeing that a “positive” or “negative” result corresponds with the real presence or absence of the sequence variant investigated, clinical validity represents the ability to identify the clinical phenotype of interest, evaluating clinical sensitivity and specificity, and positive or negative predictive values, or in other cases, the association measured as a risk or odds ratio.Citation107,Citation108 Of note, clinical utility is related to the evidence that genetic testing can provide useful information for the diagnostic process, better measures for clinical outcomes, and odds ratios for patient-management decision-making (precision medicine).Citation107,Citation108 As such, a pharmacogenetic test — potentially useful for patient treatment — must improve clinical outcomes. Evidence on the clinical utility of a pharmacogenetic assay is obtained by experimental studies, preferably RCTs. A valid method to evaluate clinical utility is the use of prospective trials on randomized subjects undergoing genetic testing or not to compare the same treatment between the two groups. Similarly, prospective trials on genetically stratified groups are also mandatory to comparing treatment outcomes between different groups.Citation108,Citation109 In other cases, clinical utility is determined by a “chain of indirect evidence” linking the results of a genetic test to intermediate data that are associated with improved clinical outcomes.Citation108,Citation110 However, pharmacogenetic research remains an expanding field, and to date there is no unanimous consensus on the best appropriate study designs to uniquely evaluate drug–response variability related to genetic variations.109 Finally, several national drug agencies are carefully evaluating risk:benefit ratios in individual cases, carefully considering the concomitant pathologies (long QT syndrome, major arrhythmias, liver or kidney failure, electrolyte disorders), pharmacological associations (in particular for drugs that increase the QT), and above all the clinical anamnesis and identification with genetic diagnosis of favism (G6PD deficiency).
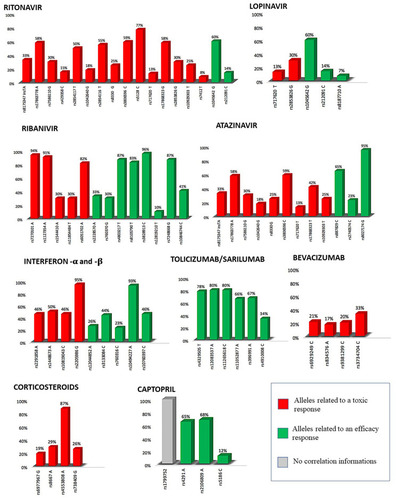
In our opinion, this is the first study to suggest the application of personalized medicine tools during the treatment of SARS-CoV2 infection. All identified SNPs, including allelic efficacy/toxicity, selected from an accurate in silico analysis have been identified for the most promising and repurposed drugs, and the investigational and adjunctive experimental drugs have been reported in both tables and figures.Citation42–Citation64 Particularly, in we graphically represent the frequency of SNP alleles related to an efficacy response (green bars) or toxicity (red bars), useful in predicting individual response to therapy with the main therapies used for Covid-19 patients. In this study, tocilizumab showed varying efficacy, while inside the antiviral group a divergent response was observed. Therefore, to understand from the beginning specific susceptibility (efficacy/toxicity) to a drug, as displayed by the presence of specific functional clusters in the genetic background of the patient under treatment, might assist the specialist toward a more “specific” selection of therapeutic agent. This would result in a more appropriate therapeutic response, with fewer ADRs. As reported in other therapies, this individualized approach appears of great utility, and particularly for the Covid-19 pandemic could improve the choice of more efficient therapy. The screening is less invasive for the patient, as it is possible by venous blood or buccal-cell swab using real-time PCR analysis.
Figure 2 Graphical representation of the frequency of SNPs’ alleles related to toxicity (red bars) and efficacy (green bars) response, useful in predicting individual response to therapy with the main drugs used for the therapy of Covid-19 patients. Allelic frequencies have been recovered by 1000 Genomes Project (https://www.internationalgenome.org/home), Ensemble (http://www.ensembl.org/index.html), dbSNPs (https://www.ncbi.nlm.nih.gov/snp/), gnomAD v2.1.1 (https://gnomad.broadinstitute.org/). The gray bar refers to SNP rs1799752 for which there is no correlation information. The information for SNP rs8027174 refers to both Atazanavir and Darunavir.
Conclusion
Any attempt to find more suitable tests, identify asymptomatic/presymptomatic and/or confirm symptomatic subjects, and therapeutic agents/strategies to sustain therapeutic decisions in Covid-19–affected patients appears mandatory. Herein, we performed a wide in silico study of genetic variants associated with the main drugs in use for Covid-19 therapy, providing a list of genetic variants of efficacy/toxicity. This study highlights the clinical utility of a pharmacogenetic tool in planning personalized treatments that are likely to become essential in the pharmacological management of Covid-19 patients.
Author Contributions
CC, AR, AM, RP, and SP conceived the study and participated in its design and coordination. CC, AR, AM, and RP contributed to data collection and analysis. All authors made a significant contribution to the work reported, whether in its conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Acknowledgments
AM and AC thank the Italian Ministry of Health and Fondazione Roma (Italy).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest and report no conflicts of interest for this work.
References
- Chen Y, Liu Q, Guo D. Emerging coronaviruses: genome structure, replication, and pathogenesis. J Med Virol. 2020;92:418–423. doi:10.1002/jmv.2568131967327
- Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:102433. doi:10.1016/j.jaut.2020.10243332113704
- Padoan A, Sciacovelli L, Basso D, et al. IgA-Ab response to spike glycoprotein of SARS-CoV-2 in patients with COVID-19: a longitudinal study. ClinicaChimica Acta. 2020;507:164–166. doi:10.1016/j.cca.2020.04.026
- Sethuraman N, Jeremiah SS, Ryo A. Interpreting diagnostic tests for SARS-CoV-2. JAMA. 2020. doi:10.1001/jama.2020.8259
- Tay MZ, Poh CM, Rénia L, MacAry PA, Ng LFP. The trinity of COVID-19: immunity, inflammation and intervention. Nat Rev Immunol. 2020;20(6):363–374. doi:10.1038/s41577-020-0311-832346093
- Ye Q, Wang B, Mao J. The pathogenesis and treatment of the `Cytokine Storm’ in COVID-19. J Infect. 2020;80(6):607–613. doi:10.1016/j.jinf.2020.03.03732283152
- Coroneoa MT. The eye as the discrete but defensible portal of coronavirus infection. Ocul Surf. 2020;S1542–0124(20):30089. doi:10.1016/j.jtos.2020.05.011
- Savarino A, Boelaert JR, Cassone A, Majori G, Cauda R. Effects of chloroquine on viral infections: an old drug against today’s diseases? Lancet Infect Dis. 2003;3:722–727. doi:10.1016/s1473-3099(03)00806-514592603
- Al-Bari MAA. Targeting endosomal acidification by chloroquine analogs as a promising strategy for the treatment of emerging viral diseases. Pharmacol Res Perspect. 2017;5:e00293. doi:10.1002/prp2.29328596841
- Müller NL, Ooi GC, Khong PL, Nicolaou S. Severe acute respiratory syndrome: radiographic and CT findings. AJR Am J Roentgenol. 2003;181:3–8. doi:10.2214/ajr.182.1.182003912818821
- Ajlan AM, Ahyad RA, Jamjoom LG, Alharthy A, Madani TA. Middle East respiratory syndrome coronavirus (MERS-CoV) infection: chest CT findings. AJR Am J Roentgenol. 2014;203(4):782–787. doi:10.2214/AJR.14.1302124918624
- Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A. Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. AJR Am J Roentgenol. 2020;14:1–7. doi:10.2214/AJR.20.23034
- Han R, Huang L, Jiang H, Dong J, Peng H, Zhang D. Early clinical and CT manifestations of Coronavirus disease 2019 (COVID-19) pneumonia. AJR Am J Roentgenol. 2020;1–6. doi:10.2214/AJR.20.22961
- Ai T, Yang Z, Hou H, et al. Correlation of chest CT and RT-PCR testing in Coronavirus Disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology. 2020:200642. doi:10.1148/radiol.2020200642.
- Wu J, Wu X, Zeng W, et al. Chest CT findings in patients with Coronavirus Disease 2019 and its relationship with clinical features. Invest Radiol. 2020;55(5):257–261. doi:10.1097/RLI.000000000000067032091414
- Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. The Lancet Respir Med. 2020;8:420–422. doi:10.1016/S2213-2600(20)30076-X32085846
- Terpos E, Ntanasis-Stathopoulos I, Elalamy I, et al. Hematological findings and complications of COVID-19. Am J Hematol. 2020;95(7):834–847. doi:10.1002/ajh.2582932282949
- Hu K, Patel J, Patel BC. Ophthalmic manifestations of Coronavirus (COVID-19) In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020.
- Ulhaq ZS, Soraya GV. The prevalence of ophthalmic manifestations in COVID-19 and the diagnostic value of ocular tissue/fluid. Graefes Arch Clin Exp Ophthalmol. 2020;258(6):1351–1352. doi:10.1007/s00417-020-04695-832328758
- Wu P, Duan F, Luo C, et al. Characteristics of ocular findings of patients with Coronavirus Disease 2019 (COVID-19) in Hubei Province, China. JAMA Ophthalmol. 2020;138(5):575–578. doi:10.1001/jamaophthalmol.2020.129132232433
- Romano MR, Montericcio A, Montalbano C, et al. Facing COVID-19 in Ophthalmology Department. Curr Eye Res. 2020;45(6):653–658. doi:10.1080/02713683.2020.175273732253942
- Roederer MW. NAVAGATE: a rubric to move from pharmacogenomics science to pharmacogenomics practice. Pharmacogenomics. 2012;13(11):1307–1313. doi:10.2217/pgs.12.11022920399
- Zhang W, Zhou HH. Translational approach for pharmacogenomics and personalized medicine. Yao XueXue Bao. 2011;46:1–5.
- Khan DA. Pharmacogenomics and adverse drug reactions: primetime and not ready for primetime tests. J Allergy Clin Immunol. 2016;138(4):943–955. doi:10.1016/j.jaci.2016.08.00227720019
- Mallal S, Nolan D, Witt C, et al. Association between presence of HLA-B*5701, HLA-DR7, and HLA-DQ3 and hypersensitivity to HIV-1 reverse-transcriptase inhibitor abacavir. Lancet. 2002;359:727–732. doi:10.1016/s0140-6736(02)07873-x11888582
- Hetherington S, Hughes AR, Mosteller M, et al. Genetic variations in HLA-B region and hypersensitivity reactions to abacavir. Lancet. 2002;359:1121–1122. doi:10.1016/S0140-6736(02)08158-811943262
- Sun J, Deng X, Chen X, et al. Incidence of adverse drug reactions in COVID-19 patients in China: an active monitoring study by Hospital Pharmacovigilance system. Clin Pharmacol Ther. 2020. doi:10.1002/cpt.1866
- Conti P, Ronconi G, Caraffa A, et al. Induction of pro-inflammatory cytokines (IL-1 and IL-6) and lung inflammation by Coronavirus-19 (COVI-19 or SARS-CoV-2): anti-inflammatory strategies. J Biol RegulHomeost Agents. 2020;34(2):1. doi:10.23812/CONTI-E
- TMA E-A, Stockand JD. Recent progress and challenges in drug development against COVID-19 coronavirus (SARS-CoV-2) - an update on the status. Infect Genet Evol. 2020;83:104327. doi:10.1016/j.meegid.2020.10432732320825
- McCreary EK, Pogue JM. Coronavirus disease 2019 treatment: a review of early and emerging options. Open Forum Infect Dis. 2020;7(4):ofaa105. doi:10.1093/ofid/ofaa10532284951
- Haas DW, Smeaton LM, Shafer RW, et al. Pharmacogenetics of long-term responses to antiretroviral regimens containing Efavirenz and/or Nelfinavir: an Adult Aids Clinical Trials Group Study. J Infect Dis. 2005;192:1931–1942. doi:10.1086/49761016267764
- Di Francia R, et al. Selected pharmacogenetic panel test for toxicity prevention of drug-drug interactions between Highly Active Antiretroviral Therapy (HAART) and antiblastic chemotherapy. WCRJ. 2015;2:e492.
- Ritchie MD, Haas DW, Motsinger AA, et al. Drug transporter and metabolizing enzyme gene variants and nonnucleoside reverse-transcriptase inhibitor hepatotoxicity. Clin Infect Dis. 2006;43(6):779–782. doi:10.1086/50710116912956
- Rodríguez-Nóvoa S, Martín-Carbonero L, Barreiro P, et al. Genetic factors influencing atazanavir plasma concentrations and the risk of severe hyperbilirubinemia. AIDS. 2007;21:41–46. doi:10.1097/QAD.0b013e328011d7c117148966
- Falagas ME, Pitsouni EI, Malietzis GA, Pappaet G. Comparison of pubmed, scopus, web of science, and google scholar: strengths and weaknesses. FASEB J. 2008;22:338–342. doi:10.1096/fj.07-9492LSF17884971
- Crews KR, Hicks JK, Pui CH, Relling MV, Evans WE. Pharmacogenomics and individualized medicine: translating science into practice. Clin Pharmacol Ther. 2012;92:467‐475. doi:10.1038/clpt.2012.120
- Ahsan T, Urmi NJ, Sajib AA. Heterogeneity in the distribution of 159 drug-response related SNPs in world populations and their genetic relatedness. PLoSOne. 2020;15(1):e0228000. doi:10.1371/journal.pone.0228000
- Sanders JM, Monogue ML, Jodlowski TZ, Cutrell JB. Pharmacologic treatments for Coronavirus Disease 2019 (COVID-19): a review. JAMA. 2020;323:1824–1836. doi:10.1001/jama.2020.601932282022
- Siddiqi HK, Mehra MR. COVID-19 illness in native and immunosuppressed states: a clinical-therapeutic staging proposal. J Heart Lung Transplant. 2020;39(5):405–407. doi:10.1016/j.healun.2020.03.01232362390
- Thorn CF, Klein TE, Altman RB. PharmGKB: the pharmacogenomics knowledge base. Methods Mol Biol. 2013;1015:311–320. doi:10.1007/978-1-62703-435-7_2023824865
- Mitra-Ghosh T, Callisto SP, Lamba JK, et al. PharmGKB summary: lamotrigine pathway, pharmacokinetics and pharmacodynamics. Pharmacogenet Genomics. 2020;30(4):81–90. doi:10.1097/FPC.000000000000039732187155
- den Dunnen JT, Dalgleish R, Maglott DR, et al. HGVS recommendations for the description of sequence variants: 2016 update. Hum Mutat. 2016;37(6):564–569. doi:10.1002/humu.2298126931183
- Kitts A, Sherry S. The Single Nucleotide Polymorphism Database (dbSNP) of Nucleotide Sequence Variation McEntyre J, Ostell J editors, The NCBI Handbook; 2002 Bethesda (MD): National Center for Biotechnology Information (US) Available from: https://www.ncbi.nlm.nih.gov/books/NBK21088/.
- Culley CL, Kiang TKL, Gilchrist SE, Ensom MHH. Effect of the UGT1A1*28 allele on unconjugated hyperbilirubinemia in HIV-positive patients receiving Atazanavir: a systematic review. Ann Pharmacother. 2013;47(4):561–572. doi:10.1345/aph.1R55023548653
- Nishijima T, Tsuchiya K, Tanaka N, et al. Single-nucleotide polymorphisms in the UDP-glucuronosyltransferase 1A-3ʹ untranslated region are associated with atazanavir-induced nephrolithiasis in patients with HIV-1 infection: a pharmacogenetic study. J Antimicrob Chemother. 2014;69:3320–3328. doi:10.1093/jac/dku30425151207
- Johnson DH, Venuto C, Ritchie MD, et al. Genomewide association study of atazanavir pharmacokinetics and hyperbilirubinemia in AIDS Clinical Trials Group protocol A5202. Pharmacogenet Genomics. 2014;24:195–203. doi:10.1097/FPC.000000000000003424557078
- Bush WS, Crosslin DR, Owusu-Obeng A, et al. Genetic variation among 82 pharmacogenes: the PGRNseq data from the eMERGE network. Clin Pharmacol Ther. 2016;100:160–169. doi:10.1002/cpt.35026857349
- Lankisch TO, Moebius U, Wehmeier M, et al. Gilbert’s disease and atazanavir: from phenotype to UDP-glucuronosyltransferase haplotype. Hepatology. 2006;44:1324–1332. doi:10.1002/hep.2136117058217
- Tarr PE, Taffé P, Bleiber G, et al. Swiss HIV Cohort Study. Modeling the influence of APOC3, APOE, and TNF polymorphisms on the risk of antiretroviral therapy-associated lipid disorders. J Infect Dis. 2005;191:1419–1426. doi:10.1086/42929515809899
- Foulkes AS, Wohl DA, Frank I, et al. Associations among race/ethnicity, ApoC-III genotypes, and lipids in HIV-1-infected individuals on antiretroviral therapy. PLoS Med. 2006;3:e52. doi:10.1371/journal.pmed.003005216417409
- da Rocha IM, Gasparotto AS, Lazzaretti RK, Notti RK, Sprinz E, Mattevi VS. Polymorphisms associated with renal adverse effects of antiretroviral therapy in a Southern Brazilian HIV cohort. Pharmacogenet Genomics. 2015;25(11):541–547. doi:10.1097/FPC.000000000000016926287941
- Elens L, Tyteca D, Panin N, et al. Functional defect caused by the 4544G>A SNP in ABCC2: potential impact for drug cellular disposition. Pharmacogenet Genomics. 2011;21(12):884–893. doi:10.1097/FPC.0b013e32834d672b22027652
- Coelho AV, Silva SP, de Alencar LC, et al. ABCB1 and ABCC1 variants associated with virological failure of first-line protease inhibitors antiretroviral regimens in Northeast Brazil patients. J Clin Pharmacol. 2013;53:1286–1293. doi:10.1002/jcph.16523996099
- Tanaka Y, Nishida N, Sugiyama M, et al. Genome-wide association of IL28B with response to pegylated interferon-alpha and ribavirin therapy for chronic hepatitis C. Nat Genet. 2009;41:1105–1109. doi:10.1038/ng.44919749757
- Mpeta B, Kampira E, Castel S, et al. Differences in genetic variants in lopinavir disposition among HIV-infected Bantu Africans. Pharmacogenomics. 2016;17(7):679–690. doi:10.2217/pgs.16.1427142945
- Moltó J, Xinarianos G, Miranda C, et al. Simultaneous pharmacogenetics-based population pharmacokinetic analysis of darunavir and ritonavir in HIV-infected patients. Clin Pharmacokinet. 2013;52:543–553. doi:10.1007/s40262-013-0057-623494984
- Mahurkar S, Moldovan M, Suppiah V, et al. Response to interferon-beta treatment in multiple sclerosis patients: a genome-wide association study. Pharmacogenomics J. 2017;17:312–318. doi:10.1038/tpj.2016.2027001119
- Kowalec K, Wright GEB, Drögemöller BI, et al. Common variation near IRF6 is associated with IFN-β-induced liver injury in multiple sclerosis. Nat Genet. 2018;50:1081–1085. doi:10.1038/s41588-018-0168-y30013178
- Torbati S, Karami F, Ghaffarpour M, Zamani M. Association of CD58 polymorphism with multiple sclerosis and response to interferon ß therapy in a subset of Iranian population. Cell J. 2015;16:506–513. doi:10.22074/cellj.2015.50525685741
- Li M, Mulkey F, Jiang C, et al. Identification of a genomic region between SLC29A1 and HSP90AB1 associated with risk of bevacizumab-induced hypertension: CALGB 80405 (Alliance). Clin Cancer Res. 2018;24:4734–4744. doi:10.1158/1078-0432.CCR-17-152329871907
- Gutierrez-Camino Á, Umerez M, Lopez-Lopez E, et al. Involvement of miRNA polymorphism in mucositis development in childhood acute lymphoblastic leukemia treatment. Pharmacogenomics. 2018;19:1403–1412. doi:10.2217/pgs-2018-011330479191
- Favis R, Sun Y, van de Velde H, et al. Genetic variation associated with bortezomib-induced peripheral neuropathy. Pharmacogenet Genomics. 2011;21:121–129. doi:10.1097/FPC.0b013e3283436b4521228734
- Gutierrez-Camino A, Martin-Guerrero I, Garcia-Orad A. PNPLA3 rs738409 and hepatotoxicity in children with b-cell acute lymphoblastic leukemia: a validation study in a Spanish cohort. Clin Pharmacol Ther. 2017;102:906. doi:10.1002/cpt.75628744905
- Thorn CF, Klein TE, Altman RB. PharmGKB summary: very important pharmacogene information for angiotensin-converting enzyme. Pharmacogenet Genomics. 2010;20:143–146. doi:10.1097/FPC.0b013e3283339bf319898265
- Devaux CA, Rolain JM, Colson P, Raoult D. New insights on the antiviral effects of chloroquine against coronavirus: what to expect for COVID-19? Int J Antimicrob Agents. 2020;55(5):105938. doi:10.1016/j.ijantimicag.2020.10593832171740
- Zhou D, Dai SM, Tong Q. COVID-19: a recommendation to examine the effect of hydroxychloroquine in preventing infection and progression. J Antimicrob Chemother. 2020;75(7):1667–1670. doi:10.1093/jac/dkaa11432196083
- Gao J, Tian Z, Yang X. Breakthrough: chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci Trends. 2020;14:72–73. doi:10.5582/bst.2020.0104732074550
- Colson P, Rolain JM, Lagier JC, Brouqui P, Raoult D. Chloroquine and hydroxychloroquine as available weapons to fight COVID-19. Int J Antimicrob Agents. 2020;55(4):105932. doi:10.1016/j.ijantimicag.2020.10593232145363
- Mohammad S, Clowse MEB, Eudy AM, Criscione-Schreiber LG. Examination of hydroxychloroquine use and hemolytic anemia in G6PDH-deficient patients. Arthritis Care Res (Hoboken). 2018;70:481–485. doi:10.1002/acr.2329628556555
- Wahie S, Daly AK, Cordell HJ, et al. Clinical and pharmacogenetic influences on response to hydroxychloroquine in discoid lupus erythematosus: a retrospective cohort study. J Invest Dermatol. 2011;131:1981–1986. doi:10.1038/jid.2011.16721734714
- Browning DJ. Hydroxychloroquine and chloroquine retinopathy: screening for drug toxicity. Am J Ophthalmol. 2002;133:649–656. doi:10.1016/s0002-9394(02)01392-211992862
- Leung LS, Neal JW, Wakelee HA, Sequist LV, Marmor MF. Rapid onset of retinal toxicity from high-dose hydroxychloroquine given for cancer therapy. Am J Ophthalmol. 2015;160:799–805. doi:10.1016/j.ajo.2015.07.01226189086
- Romano MR, Raimondi R, Montericcio A, Allegrini D. Hydroxychloroquine and ritonavir for COVID-19 infection: a possible synergic toxicity for retinal pigmented epithelium. Graefes Arch Clin Exp Ophthalmol. 2020;1. doi:10.1007/s00417-020-04727-331776657
- Chu CM, Cheng VC, Hung IF, et al. HKU/UCH SARS Study Group. Role of lopinavir/ritonavir in the treatment of SARS: initial virological and clinical findings. Thorax. 2004;59:252–256. doi:10.1136/thorax.2003.01265814985565
- de Wilde AH, Jochmans D, Posthuma CC, et al. Screening of an FDA-approved compound library identifies four small-molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture. Antimicrob Agents Chemother. 2014;58:4875–4884. doi:10.1128/AAC.03011-1424841269
- Chan KS, Lai ST, Chu CM, et al. Treatment of severe acute respiratory syndrome with lopinavir/ritonavir: a multicentre retrospective matched cohort study. Hong Kong Med J. 2003;9:399–406.14660806
- Cao B, Wang Y, Wen D, et al. A trial of lopinavir-ritonavir in adults hospitalized with severe Covid-19. N Engl J Med. 2020;382(19):1787–1799. doi:10.1056/NEJMoa200128232187464
- Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med. 2020:e200994. doi:10.1001/jamainternmed.2020.0994.
- Foolad F, Aitken SL, Shigle TL, et al. Oral versus aerosolized ribavirin for the treatment of respiratory syncytial virus infections in hematopoietic cell transplant recipients. Clin Infect Dis. 2019;68:1641–1649. doi:10.1093/cid/ciy76030202920
- Stockman LJ, Bellamy R, Garner P. SARS: systematic review of treatment effects. PLoS Med. 2006;3:e343. doi:10.1371/journal.pmed.003034316968120
- Muller MP, Dresser L, Raboud J, et al. Adverse events associated with high-dose ribavirin: evidence from the toronto outbreak of severe acute respiratory syndrome. Pharmacotherapy. 2007;27:494–503. doi:10.1592/phco.27.4.49417381375
- Hadziyannis SJ, Sette H Jr, Morgan TR, et al. Peginterferon-alpha2a and ribavirin combination therapy in chronic Hepatitis C: a randomized study of treatment duration and ribavirin dose. Ann Intern Med. 2004;140:346–355. doi:10.7326/0003-4819-140-5-200403020-0001014996676
- Lian N, Xie H, Lin S, Huang J, Zhao J, Lin Q. Umifenovir treatment is not associated with improved outcomes in patients with coronavirus disease 2019: a retrospective study. Clin Microbiol Infect. 2020;26(7):917–921. doi:10.1016/j.cmi.2020.04.02632344167
- Sallard E, Lescure FX, Yazdanpanah Y, Mentre F, Peiffer-Smadja N. Type 1 interferons as a potential treatment against COVID-19. Antiviral Res. 2020;178:104791. doi:10.1016/j.antiviral.2020.10479132275914
- Hung IF, Lung KC, Tso EY, et al. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: an open-label, randomised, Phase 2 trial. The Lancet. 2020;395(10238):1695–1704. doi:10.1016/S0140-6736(20)31042-4
- Totura AL, Bavari S. Broad-spectrum coronavirus antiviral drug discovery. Expert Opin Drug Discov. 2019;14(4):397–412. doi:10.1080/17460441.2019.158117130849247
- Wang M, Cao R, Zhang L, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020;30(3):269–271. doi:10.1038/s41422-020-0282-032020029
- Rossignol JF. Nitazoxanide, a new drug candidate for the treatment of Middle East respiratory syndrome coronavirus. J Infect Public Health. 2016;9(3):227–230. doi:10.1016/j.jiph.2016.04.00127095301
- Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181(2):271–280.e8. doi:10.1016/j.cell.2020.02.05232142651
- Andreani J, Le Bideau M, Duflot I, et al. In vitro testing of combined hydroxychloroquine and azithromycin on SARS-CoV-2 shows synergistic effect. Microb Pathog. 2020;145:104228. doi:10.1016/j.micpath.2020.10422832344177
- Al-Tawfiq JA, Al-Homoud AH, Memish ZA. Remdesivir as a possible therapeutic option for the COVID-19. Travel Med Infect Dis. 2020;34:101615. doi:10.1016/j.tmaid.2020.10161532145386
- Siegel D, Hui HC, Doerffler E, et al. Discovery and synthesis of a phosphoramidate prodrug of a pyrrolo[2,1-f][triazin-4-amino] adenine C-nucleoside (GS-5734) for the treatment of Ebola and emerging viruses. J Med Chem. 2017;60(5):1648–1661. doi:10.1021/acs.jmedchem.6b0159428124907
- Cao YC, Deng QX, Dai SX. Remdesivir for severe acute respiratory syndrome coronavirus 2 causing COVID-19: an evaluation of the evidence. Travel Med Infect Dis. 2020;35:101647. doi:10.1016/j.tmaid.2020.10164732247927
- Furuta Y, Komeno T, Nakamura T. Favipiravir (T-705), a broad spectrum inhibitor of viral RNA polymerase. Proc Jpn Acad Ser B Phys Biol Sci. 2017;93(7):449–463. doi:10.2183/pjab.93.027
- Dong L, Hu S, Gao J. Discovering drugs to treat coronavirus disease 2019 (COVID-19). Drug Discov Ther. 2020;14(1):58–60. doi:10.5582/ddt.2020.0101232147628
- Chinello P, Petrosillo N, Pittalis S, et al. INMI Ebola Team. QTc interval prolongation during favipiravir therapy in an Ebolavirus-infected patient. PLoS Negl Trop Dis. 2017;11(12):e0006034. doi:10.1371/journal.pntd.000603429283993
- Kumagai Y, Murakawa Y, Hasunuma T, et al. Lack of effect of favipiravir, a novel antiviral agent, on QT interval in healthy Japanese adults. Int J Clin Pharmacol Ther. 2015;53(10):866–874. doi:10.5414/CP20238826308176
- Savic RM, Barrail-Tran A, Duval X, et al. ANRS 134-COPHAR 3 Study Group. Effect of adherence as measured by MEMS, ritonavir boosting, and CYP3A5 genotype on atazanavir pharmacokinetics in treatment-naive HIV-infected patients. Clin Pharmacol Ther. 2012;92(5):575–583. doi:10.1038/clpt.2012.13723033116
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. The Lancet. 2020;395:1054–1062.
- Mehta P, McAuley DF, Brown M, et al. HLH Across Speciality Collaboration, UK. COVID-19: consider cytokine storm syndromes and immunosuppression. The Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
- Xu X, Han M, Li T, et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci USA. 2020;117(20):10970–10975. doi:10.1073/pnas.200561511732350134
- Russell CD, Millar JE, Baillie JK. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. The Lancet. 2020;395(10223):473–475. doi:10.1016/S0140-6736(20)30317-2
- Arabi YM, Mandourah Y, Al-Hameed F, et al. Saudi Critical Care Trial Group. Corticosteroid therapy for critically ill patients with Middle East respiratory syndrome. Am J Respir Crit Care Med. 2018;197(6):757–767. doi:10.1164/rccm.201706-1172OC29161116
- Yan J, Liu A, Huang J, Wu J, Fan H. Research progress of drug treatment in novel Coronavirus pneumonia. AAPS Pharm Sci Tech. 2020;21(4):130. doi:10.1208/s12249-020-01679-z
- Gurwitz D. Angiotensin receptor blockers as tentative SARS-CoV-2 therapeutics. Drug Dev Res. 2020;81(5):537–540. doi:10.1002/ddr.2165632129518
- Saavedra JM. Angiotensin receptor blockers and COVID-19. Pharmacol Res. 2020;156:104832. doi:10.1016/j.phrs.2020.10483232304747
- Teutsch SM, Bradley LA, Palomaki GE, et al., EGAPP Working Group. The Evaluation of Genomic Applications in Practice and Prevention (EGAPP) initiative: methods of the EGAPP Working Group. Genetics Medi. 2009;11(1):3–14. doi:10.1097/GIM.0b013e318184137c
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; Board on the Health of Select Populations; Committee on the Evidence Base for Genetic Testing. An Evidence Framework for Genetic Testing. Washington (DC): National Academies Press (US); 20173 27: 3 https://www.ncbi.nlm.nih.gov/books/NBK425803/. Accessed 924, 2020.
- Smit RAJ, Noordam R, le Cessie S, Trompet S, Jukema JW. A critical appraisal of pharmacogenetic inference. Clin Genet. 2018;93(3):498–507. doi:10.1111/cge.1317829136278
- Dotson WD, Bowen MS, Kolor K, Khoury MJ. Clinical utility of genetic and genomic services: context matters. Genet Med. 2016;18(7):672–674. doi:10.1038/gim.2015.15326656648