
Abstract
Objectives
To revise the Living with Medicines Questionnaire version 2 (LMQ-2), which measures the burden of using prescribed medicines, to include cost and expand side effects and social issues.
Methods
New statements were developed and validated through cognitive interviews with medicine users, and these and a global visual analog scale (VAS) were added to the 42-item LMQ-2. Construct validity was assessed through exploratory and confirmatory factor analyses using an online public survey. Criterion-related validity was measured against the Treatment Satisfaction Questionnaire with Medication (TSQM-II) and the EuroQoL 5-level quality of life measure (EQ-5D-5L), in patients using community pharmacies, general practices, and outpatient clinics. Reliability was assessed by test–retest using online public distribution.
Results
The 58-item interim instrument (n=729) was reduced to 41 items after factor analysis, which confirmed an eight-domain structure: relationships with health professionals, practicalities, interferences, effectiveness, side effects, concerns, cost, and autonomy, constructed as medicine burden. All subscales, except autonomy, were loaded onto this construct and showed acceptable internal consistency. LMQ-VAS correlated with total LMQ scores (r=0.571). Criterion validation (n=422) demonstrated total LMQ scores negatively correlated with TSQM scores for global satisfaction (r=–0.616); domain scores showed similar correlations: effectiveness (r=–0.628), side effects (r=–0.597), and practicalities (r=–0.529). Total LMQ score was negatively correlated with EQ VAS (r=–0.383) and showed weak/moderate relationships with individual EQ-5D-5L dimensions. Test–retest (n=30) reliability showed intra-class correlation coefficients of 0.954 (total LMQ score), 0.733–0.929 (domain scores), and 0.789 (global item).
Conclusion
The LMQ version 3 (LMQ-3) instrument has acceptable construct, criterion-related and known-groups validity, and is internally consistent as a measure of medicine burden, although reliability requires further confirmation. It could be used to measure the outcome of interventions designed to reduce the burden of polypharmacy.
Introduction
Polypharmacy, defined as the use of multiple medicines on a daily basis by an individual, is a growing phenomenon worldwide, due to increases in life expectancy and the prevalence of chronic medical conditions such as cardiovascular disease, type 2 diabetes, arthritis, osteoporosis, and the increasing use of medicines to manage these conditions.Citation1 However, while the number of medicines is potentially an indicator of the frequency with which problems such as drug interactions may occur,Citation2 the patient experience of using multiple medicines is often overlooked.Citation3 Yet, it is increasingly recognized that the treatments imposed on individuals by health professionals can be burdensome. Treatment burden, which covers everything patients do to take care of their health,Citation4 for most patients includes managing one or more medicines.Citation5
From the biomedical perspective, “problematic polypharmacy” has been defined as “multiple medications prescribed inappropriately, or where the intended benefit of the medication is not realized,”Citation6 and a range of interventions have developed which could be used to reduce the number of medicines and optimize their use.Citation7,Citation8 A key element of optimizing medicine use in individual patients is the need to understand their experience, including any difficulties and concerns. In England, both the Medicines Optimisation Strategy, developed by the Royal Pharmaceutical Society,Citation9 and other national guidanceCitation10 emphasize the need to determine the patient experience as the first stage in this process. Patients’ attitudes toward and experiences with using medicines (positive and negative), their attempts at experimentation and prioritizing, together with issues relating to obtaining medicines and their relationship to prescribers all contribute to the success of any intervention aiming to reduce problems with medicines.Citation11,Citation12 A means of quantifying the patient’s individual medicine experience is thus essential for practice, while appropriate outcome measures are also necessary for evaluating interventions. However, there are few patient-reported outcome measures available which focus solely on medicine use and which thus have the potential to demonstrate change following interventions designed to reduce problems with medicines in patients using polypharmacy.Citation13,Citation14
We have developed an instrument designed to measure the patient experience of long-term polypharmacy conceptualized as medicine burden, the Living with Medicines Questionnaire version 2 (LMQ-2).Citation15 This instrument, unlike most other patient-reported measures, was developed from the patient perspective.Citation16 The instrument consists of 42 statements accompanied by a 5-point Likert-type scoring system. Eight domains were identified through factor analysis, relating to: perceptions about effectiveness, concerns about medicine use, patient–provider relationships and communication about medicines, practical difficulties, interferences to daily life, autonomy/control over medicine, and acceptance of medicine use, all areas which have been cited by users of long-term medicines as burdensome.Citation15
Some respondents to this instrument identified that it lacked a domain covering cost burden, which can be an issue of concern to some patients, even in countries with good access to free medicines.Citation17–Citation19 Cost burden has also been recognized as potentially important in the measurement of overall treatment burden.Citation4 Other respondents suggested that greater emphasis needed to be placed on the social aspects of using medicines and experiences of side effects. Review of the 42 statements included in the LMQ-2 showed that the two covering social aspects were indeed limited and the two covering side effects did not emphasize the effect of these on daily life. We therefore set out to develop a revised version of this instrument, which addressed these issues more fully, without enlarging it, and to undertake a rigorous validation of the revised instrument.
Methods
Item generation and content validation
New content was based on reanalysis of the 21 patient interviews used to elicit concepts in the original LMQCitation20 and free-text comments from survey participants completing this version of the instrument,Citation15 along with qualitative studies reported in the literature.Citation12,Citation21–Citation23 All items were reviewed and new items added through discussions among the researchers (BK, SC, JK). An interim instrument, which included 58 items (LMQ-2.1), was developed and assessed for face and content validity through cognitive interviews with long-term medicine users, recruited via a public engagement group. Members of the group who met the inclusion criteria (18 years or older, using regular prescription medicines, able to read and communicate in English, and living in England) participated themselves and/or recruited other eligible participants through snowballing.
Study instruments
The interim version (LMQ-2.1) was similar to the LMQ-2, but contained 58 statements, rated on a 5-point Likert-type scale (strongly agree to strongly disagree), utilizing reverse scoring as appropriate with higher scores reflecting worse experiences of medicine use (higher medicine burden). A 10 cm visual analog scale (VAS) was also included as a global item, with anchors indicating “no burden at all” to “extremely burdensome”, to assess the overall medicine burden (VAS-burden). Participant characteristics gathered included general demographics as well as number, frequency, and type of formulation of regular medicines and support with using medicines. The process of assessing construct validity in Stage 1 resulted in item reduction; therefore, the instrument used for Stages 2 and 3 (LMQ-3) differed in the number of Likert-type statements.
The instruments used to assess criterion-related validity of the LMQ-3 were the Treatment Satisfaction Questionnaire with Medication (TSQM-II), an 11-item instrument which measures satisfaction with prescription medicines in four subscales (effectiveness, side effects, convenience, and global satisfaction), and the EuroQoL 5-level quality of life measure (EQ-5D-5L). The latter is a widely used five-item measure of health-related quality of life (HRQoL), including a VAS which measures overall health status. Permission to use the TSQM-II and the EQ-5D-5L (UK English versions) was granted by the Quintiles group (Inc) and the EuroQol Research Foundation, respectively.
Psychometric testing
Different groups of participants were involved in psychometric testing of the LMQ, which was done over three stages. All participants were required to answer screening questions to ensure they met inclusion criteria stated earlier before completing the instrument. Consent was implied by return of completed paper questionnaires or electronic submission of online responses. IBM SPSS version 22 and AMOS version 22 were used for statistical analyses.
Construct validity and internal consistency (Stage 1)
This used an online survey, publicized via social media, including Twitter and Facebook posts through UK patient organizations, and health websites which permitted access to their memberships. A missing data analysis was undertaken, then respondents who had completed all 58 items (LMQ-2.1) were included in exploratory (EFA) and confirmatory factor analyses (CFA) to elucidate and confirm the underlying factor structure of the instrument. The sample was split randomly into two and both subsamples were assessed for normality prior to use in EFA and CFA. Sample size adequacy for factor analyses was examined via Kaiser–Meyer–Olkin Measure (KMO) and by the number of items per response, though there is no universally accepted method.Citation24 Bartlett’s Test of Sphericity and Pearson’s correlation matrix were used to assess factorability of data and potential multi-collinearity. All 58 items (LMQ-2.1) were initially subjected to principal axis factoring, using oblique factor rotation (promax) on the basis that domains were inter-related. Kaiser’s criterion (eigenvalues >1), scree plots, and parallel analysis were used to determine the number of factors for EFA.
Criteria for item reduction were: low communalities (<0.3), poor loadings on the primary factor (<0.32), and/or cross loading (>0.4) on two or more factors.Citation25–Citation27 Items loading on unstable (weak) factors, which had fewer than three items, and items with floor and ceiling effects were considered for removal, the latter defined as having skewness and kurtosis values above two or over 65% selecting either of the extreme options.
The second half of the dataset was subjected to CFA to test a higher-order (second-order) model involving only the remaining items, using maximum likelihood estimation, based on the strength of correlations among domains derived from the EFA, and preliminary testing of a first-order model. We hypothesized that medicine burden could explain the variation among all domains within the LMQ. Goodness-of-fit indices used to assess the second-order model were: relative chi-square (chi-square statistic/degrees of freedom), root mean square error of approximation (RMSEA) with 90% confidence interval (90% CI), comparative fit index (CFI), and Tucker–Lewis index (TLI). The magnitude and direction of factor loadings was also examined to ascertain the relative contribution of different items and/or domains to the models.Citation28,Citation29
In addition, LMQ total scores were compared to scores from the VAS, “Overall, how much of a burden do you feel your medicines are to you?” using Pearson’s correlation coefficient to add further to construct validation. Cronbach’s α was examined to assess the internal consistency of the LMQ-3 subscales.
Criterion-related validity (Stage 2)
The LMQ-3 together with two other relevant measures, the TSQM-IICitation30,Citation31 and a HRQoL measure (EQ-5D-5L),Citation32 were distributed by hand to patients in community pharmacies, general practices, and hospital outpatient waiting areas. Spearman’s correlation coefficients were used to assess relationships between the three instruments, with coefficients <0.35 interpreted as weak, 0.35–0.5 as moderate, and >0.5 as strong, taking a p-value of 0.05 as representing statistical significance.Citation33 A negative relationship between overall medicine burden and treatment satisfaction (measured with the TSQM-II) was hypothesized, and LMQ-3 domain scores for side effects, lack of effectiveness, and practical difficulties were predicted to show negative correlations with scores on the TSQM-II global satisfaction, satisfaction with side effects, satisfaction with effectiveness, and satisfaction with convenience subscales. Medicine burden was hypothesized to be negatively, but weakly, related to overall health status (measured with the EQ VAS), since the two constructs were hypothesized as being distinct.
Known-groups validity
The same population was used to assess known-groups validity, using the demographic data contained in the LMQ-3. Medicine-related burden was hypothesized to relate positively with regimen complexity, particularly the number of medicines, frequency of administration, and the formulation used. The need for social support with managing medicines was also predicted to indicate higher medicine burden. In addition, cost burden was hypothesized to be associated with having to make co-payments for prescribed medicines and living in areas of higher relative deprivation. Relationships were assessed using independent samples t-tests or one-way analysis of variance.
Test–retest reliability (Stage 3)
This was assessed using online distribution to a cohort of the general public who had signed up to a research unit, with the instrument redistributed to respondents after 2 weeks. Stability of scores was assessed for subscales (domains), the LMQ-3 total score, and the global VAS score using intra-class correlation coefficients (ICCs) and their 95% confidence intervals, which were estimated by using the two-way mixed effects model for absolute agreement where rater effects were assumed constant, with an ICC value of ≥0.7 considered as acceptable.Citation34
Missing data analysis
The patterns of missing responses to Stage 1 and Stage 2 were assessed, and for Stages 2 and 3, the demographic characteristics of those with partial responses compared to those who fully completed the LMQ-3, using chi-squared tests, where appropriate.
Ethical approval
Approval was obtained from the Medway School of Pharmacy research ethics committee for studies involving the general public (instrument revision, Stages 1 and 3). Approval for stage 2 was granted from the National Health Service research ethics committee South Central Oxford C and relevant research governance obtained. All procedures performed were in accordance with the ethical standards of the institutional or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Results
Completion rates and participant demographics
Eleven participants, six of whom were male, aged 42–75 years and using between 1 and 12 regular medicines participated in the cognitive interviews. Recruitment was terminated after the 11th interview, as no new problems with the revised instrument emerged from the interviews, which showed similarities in interpretation of questionnaire items and general concepts underpinning the LMQ and no unique item meanings (i.e., data saturation). There were no major comprehension problems, and most participants understood the concept of the term burden as used in the VAS.
The few minor uncertainties which arose were resolved through discussions among the team, and revisions were made to item wording.
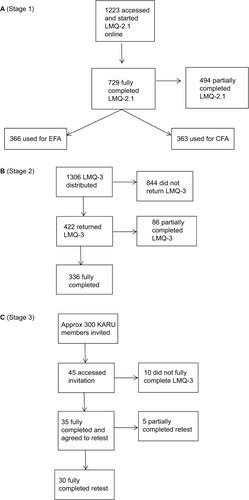
The details of respondent numbers for the remainder of the study are shown in . A total of 1223 individuals accessed the online survey in Stage 1 over a 3-month period, of whom 361 did not respond to any questions at all. The 729 participants who fully completed all 58 items (59.6% completion rate) were divided into two samples for EFA (366) and CFA (363). For Stage 2 (criterion-related validation), 1306 questionnaires were distributed: 220 in GP practices, 150 in community pharmacies, and 936 in outpatient clinics. Overall, 422 completed questionnaires were returned, representing a 32.3% completion rate, 36.4% (n=80), 44.7% (n=67), and 29.4% (n=275) for GP practices, community pharmacies, and outpatient clinics, respectively. Item-level completion rates were high (91.9%–100%), with 336 (79.6%) fully completing all 41 Likert-type statements. The Stage 3 invitation to complete the test–retest questionnaire was sent tô300 members of a research unit; however, no data were available on the proportion of the members eligible for this stage. Forty-five people responded: 35 (78%) completed the baseline questionnaire and 30 (86%) fully completed the retest questionnaire.
Figure 1 Flow diagrams illustrating respondent numbers in each stage of the study.
Demographic details of all the three participant groups are shown in . Overall, more than half of all participants were female, the majority were white and the number of medicines used was similar among all groups, the highest number used being 26. The patients involved in assessing criterion-related and known-groups validity (Stage 2) were older and had lower education levels than the public who were involved in the factor analysis study (Stage 1). There were sufficient numbers of respondents in Stage 2 who used medicines more than once a day, needed support from others to manage their medicines, and had to pay for their medicines to enable assessment of known-groups validity.
Table 1 Characteristics of study participants
Construct validity and internal consistency (Stage 1)
Responses to individual LMQ items were normally distributed, all having skewness values <2.0; only five items had skewness values >2. Potential floor/ceiling effects were observed for only five items, the most skewed having 59.1% of respondents selecting the lowest scoring option. The EFA sample size (n=366) met the minimum requirements for factor analysis of at least five participants per item, a KMO value of 0.902 (acceptable values ≥0.6) and Bartlett’s Test of Sphericity being significant (chi-square =10,585.7, df=1653; p<0.001).Citation35 All inter-variable correlations were <0.8, and there was thus no evidence of multi-collinearity (or redundancy) among items. Conversely, most correlations were >0.3, indicating sufficient commonality to justify the presence of underlying factors.
The initial EFA solution resolved into 13 factors with eigenvalues >1, explaining 63.4% of the total variance. The scree plot suggested retention of eight factors, while parallel analysis revealed seven factors met statistical inclusion criteria. An eight-factor solution was most stable and conceptually interpretable. The eight factors were termed: interferences with day-to-day life, relationships and communication about medicines, lack of effectiveness, general concerns about medicines, side effects, practical difficulties, cost-related burden, and lack of autonomy/control of medicine use.
A total of 17 items were deleted from the preliminary 58-item pool after exploratory factor analysis, leaving a 41-item questionnaire (LMQ-3). shows the 41 LMQ-3 items retained and the eight-factor structure.
Table 2 EFA-derived factor structure of the LMQ-3 (N=366)
The sample of 363 was adequate for CFA, and multivariate normality was acceptable as judged by Mardia’s coefficient (171.6, critical ratio =27.5). First-order factor loadings were in the range of 0.396–0.891 and were statistically significant (p<0.001) for all items. CFA confirmed inter-correlations among factors underlying the LMQ-3, although “autonomy” was least correlated with other factors. In the hypothesized second-order model (), factor loadings were in the range of 0.32–0.88 and statistically significant (p<0.001) for seven domains, being strongest for “interferences” (0.88), “side effects” (0.85), and “concerns” (0.81). “Autonomy” did not load significantly on medicine burden (0.11, p=0.224), but empirical attempts to exclude it were unable to significantly improve overall model fit and the domain was retained based on professional judgment. Relative chi-square values (2.083, acceptable value <3) and RMSEA coefficients (0.055, 90% CI 0.051–0.058, acceptable value <0.06) depicted an adequate model fit, although the TLI and CFI values of 0.866 and 0.874, respectively, were very slightly below the target of ≥0.90.
Figure 2 Hierarchical CFA model for the 41-item Living with Medicines Questionnaire version 3.
Abbreviations: CFA, confirmatory factor analyses; Int, interferences with day-to-day life; SideE, side effects; Conc, general concerns about medicines; Effec, lack of effectiveness; Prac, practical difficulties; Relat, patient–doctor relationships and communication about medicines; Cost, cost-related burden; Auto, lack of autonomy/control over medicine use; e1–e41 = variance associated each item; eI–eA represent variance associated with each of the eight factors or domains (interferences to autonomy respectively); Q, question.
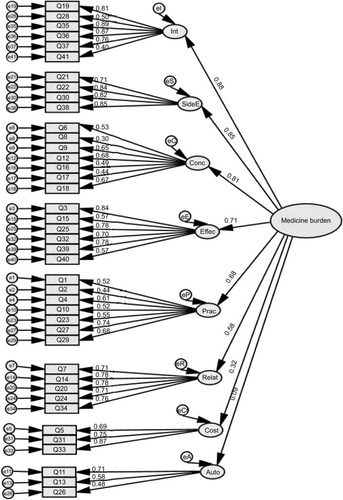
All LMQ-3 subscales, except for “autonomy”, showed acceptable internal consistency (Cronbach’s α coefficients >0.7) (). A positive correlation was found between LMQ total scores and VAS burden scores (r=0.571, p<0.001).
Criterion-related validity (Stage 2)
The correlation between scores on the LMQ-3 total scale and the global satisfaction scale of the TSQM-II was strong and negative (r=–0.616) as hypothesized, confirming that higher medicine burden was associated with lower satisfaction (). As predicted, correlations were strongest between thematically comparable subscales of the two instruments: LMQ-3 lack of effectiveness with TSQM-II satisfaction with effectiveness (r=–0.628); LMQ-3 side effect burden with TSQM-II satisfaction with side effects (r=–0.597); and LMQ-3 practical difficulties with TSQM-II satisfaction with convenience of medicine use (r=–0.529).
Table 3 Correlations between domains of the LMQ-3 and TSQM-II subscales
Correlations between LMQ-3 total score and EQ-5D-5L scores ranged from 0.284 to 0.436 (p<0.01), depicting weak to moderate relationships between medicine burden and individual HRQoL dimensions, the weakest correlation being for self-care and the strongest for anxiety/depression. LMQ-3 total score was negatively associated with general health status reported on the EQ VAS (r=–0.383; p<0.01), as hypothesized.
Known-groups validity
There were statistically significant differences in mean LMQ-3 total scores dependent on the number of medicines used, frequency of daily medicine taking, and need for support with managing medicines (). Age and employment status were not predicted to affect LMQ-3 total scores, but data showed that older people perceived themselves to have lower medicine burden than younger participants, while higher scores were also seen in those who were unemployed. One factor contributing to this latter finding was cost burden, which was higher in the unemployed (mean ± SD 8.8±3.2) compared to those employed (mean ± SD 7.3±3.2) (p<0.05). Total LMQ scores were also higher in those who made a co-payment for prescription medicines.
Table 4 Known-groups validity of the LMQ-3
Test–retest reliability (Stage 3)
The median test–retest duration was 15 days. All eight domain scores had satisfactory ICC values ranging from 0.733 to 0.929. The total LMQ-3 score was highly correlated between test and retest (r=0.91), mean scores being 91.07±18.92 and 92.14±19.55, respectively, and the ICC value being 0.954. In addition, the global item had an ICC of 0.789.
Missing data analysis
The online survey used for Stage 1 showed a pattern of non-response that was directly related to the length of the 58-item LMQ-2.1 instrument and its online presentation of 4–5 questions per page (). For Stage 2, there were 86 respondents who partially completed the LMQ-3 (); the most frequently omitted questions are shown in . The majority of missing responses could be due to the view that the statement was of no direct relevance, as there were 44 who missed at least one question covering cost burden, and 18 who only omitted questions from this domain. However, the pattern also suggests that the length of the LMQ-3 was also a potential reason for failure to fully complete the questionnaire. The 86 partial responders were younger, more highly educated, and using fewer medicines than the 336 who fully completed the LMQ-3 (). The respondents who failed to complete the second questionnaire in Stage 3 were similar in age, education, employment status, and number of medicines used to those who did, but three of the five were male, whereas the majority completing both questionnaires were female.
Figure 3 Number of missing responses to LMQ questions.
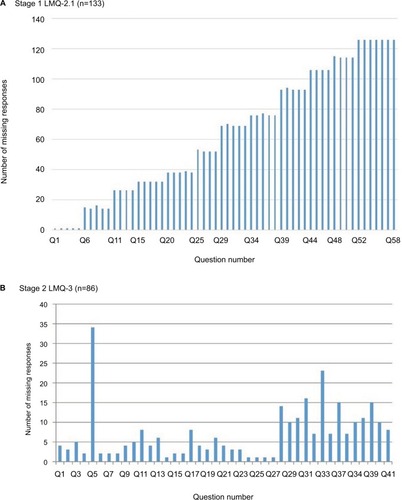
Table 5 Items with more than 2% missing data in Stage 2
Table 6 Differences between full and partial respondents of LMQ-3 in Stage 2
Discussion
This paper describes a revised version of a measure of overall medicine experiences, conceptualized as medicine burden. The LMQ-3 demonstrated adequate construct validity and was appropriately related to other instruments designed to measure relevant constructs, being negatively related to treatment satisfaction. Differences in medicine burden were shown in relation to key factors, in particular frequency of daily use and need for support with using medicines, and the instrument may also have acceptable test–retest reliability, although this requires confirmation in other studies. The eight domains incorporate all the issues covered by the previous version, with the exception of a domain relating specifically to communication with pharmacists. The inclusion of cost-related burden in this revised version was relevant as demonstrated by its clear association with paying prescription charges. Side effects were strengthened within this version into a separate domain and proved to be one of those most strongly associated with overall medicine burden, in addition to interferences with daily life and general concerns. The autonomy domain was less internally consistent and also loaded less well on the overall burden construct in the second-order model. Our decision to retain it was based on the need for this domain identified in the original qualitative interviews on which the instrument was based.Citation20 These interviews found that some people feel powerless to change their regimen and feel constrained as a result,Citation20 while others consider the decision whether or not to take any particular medicine is theirs alone. Given that this is fundamental to patient-centered medicine optimization, the autonomy domain was essential to the instrument.
It was notable that total LMQ-3 scores were not strongly related to age and their relationship with the number of medicines was not linear. This suggests that the medicine burden for individuals is dependent on a range of factors, and that neither age nor the number of medicines alone is likely to identify those in need of greater support. Indeed, the frequency with which medicines were administered and the need for support appeared to show relationships with overall burden. As with general treatment burden, any individual’s perception of the extent of their own medicine burden will depend on social circumstances and coping skills. However, there was a positive relationship between total LMQ-3 scores and VAS-burden score, suggesting that the instrument does measure the construct of medicine burden.
Strengths and limitations
The LMQ instrument was developed from the patient perspective and the modifications made which resulted in this revised version also used only material derived from and tested by users of long-term medicines. The data used for item generation were drawn from previous studies carried out in 2008 and 2014 and international literature published over several decades, thus covering issues of international and ongoing significance to medicine users.
The development and three stages of testing adhered to standard guidelines for patient-reported outcome measuresCitation34,Citation36,Citation37 and involved a total of 1197 individuals, both members of the public and patients, recruited using a range of methods from different areas across England and in different health care settings. The overall population included people aged from 18 to 92 years, using between 1 and 26 medicines regularly, with varying frequency of medicines administration and diverse formulations, some who have assistance in managing medicines, and some who contribute to paying for medicines. Stage 1 respondents were drawn from the whole of England, whereas those in Stages 2 and 3 were from South East England. However, we have no reason to suppose that patients and members of the public in the South East differ from those across the rest of England in their medicine experiences. The majority of respondents in Stages 1 and 3, which required access to the Internet, were female, and the samples were biased toward those with higher education levels. In contrast, males were well represented in Stage 2, with respondents also being older and less highly educated. However, the frail or housebound may have been excluded from this stage by virtue of the recruitment methods used. There is no gold standard for measuring medicine burden; hence, we used treatment satisfaction and HRQoL measures to assess criterion validity and confirmed that the LMQ measures a distinct concept. Test–retest assessment assumed that the sample population studied was stable in terms of their prescription medicine use experiences, hence medicine burden, and was not large enough to confirm this aspect of the instrument. Moreover, the length of the instrument is a potential barrier to completion, and some questions may be perceived as of no direct relevance to some individuals. The items covering cost and some social impacts, which this revised instrument was designed to incorporate, may thus need to include alternative responses.
Relevance to research and practice
Other measures of treatment burden either focus on individual disease states or involve aspects of care beyond medicines,Citation4,Citation13 but many of the domains and issues included in these instruments are similar to those covered by the LMQ-3. This suggests that the LMQ-3, as a generic measure of medicine use, may be particularly useful as a patient-reported outcome measure in studies designed to reduce the burden of polypharmacy in patients with multimorbidity. The finding that the relationship between medicine burden and the number of medicines is not clear-cut is important for practice. As has been found by others, some individuals may be burdened by relatively few medicines, while others do not perceive large quantities of medicines to be burdensome.Citation4,Citation12,Citation38,Citation39 Current guidelines produced by National Institute for Health and Care Excellence on multimorbidity suggest that the number of regular medicines prescribed is used as a marker of increased treatment burden and suggests using an approach which takes into account multimorbidity for those prescribed 10 or more regular medicines or those prescribed fewer than 10 regular medicines who are at particular risk of adverse events.Citation40
Further work to confirm reliability, assess sensitivity to change, and to determine whether greater perceived burden relates to adherence and clinical outcomes is desirable. To date, the LMQ-3 has been successfully translated into ArabicCitation41 and is also being used in studies in several other countries, which will contribute to obtaining a fuller picture of the usefulness of this instrument and provide comparative data on the burden of using long-term medicines across settings.
Author contributions
All authors conceived and designed the study. BK conducted the research, including data collection and analysis, and all authors interpreted the findings. All authors contributed to drafting and critical appraisal of the manuscript, and agreed the final version presented. Overall guarantor of the article is JK. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
We thank all study participants, patient organizations, health websites, community pharmacies, general practices, hospital clinics, and the Kent Adult Research Unit that permitted survey distribution. We also thank our undergraduate students for support in data collection. This work was supported by the Medway School of Pharmacy and the Commonwealth Scholarship Commission, as a PhD program. Some preliminary results of this work were presented at the International Social Pharmacy Workshop in Aberdeen, UK (July 2016), and at the Pharmaceutical Care Network Europe Working Conference in Bled, Slovenia (February 2017). The work constitutes part of the PhD thesis of Barbra Katusiime, which is available online at https://kar.kent.ac.uk/62939/.
Disclosure
The authors report no conflicts of interest in this work.
References
- BarrettKLucasEAlexanderGCHow polypharmacy has become a medical burden worldwideClinical Pharmacist201686
- GuthrieBMakubateBHernandez-SantiagoVDreischulteTThe rising tide of polypharmacy and drug-drug interactions: population database analysis 1995–2010BMC Med20151311025563062
- HeatonJBrittenNKrskaJReeveJPerson-centred medicines optimisation policy in England: an agenda for research on polypharmacyPrim Health Care Res Dev201718243427306579
- TranV-TMontoriVMEtonDTBaruchDFalissardBRavaudPDevelopment and description of measurement properties of an instrument to assess treatment burden among patients with multiple chronic conditionsBMC Med2012106822762722
- EtonDRidgewayJEggintonJFinalizing a measurement framework for the burden of treatment in complex patients with chronic conditionsPatient Relat Outcome Meas2015611712625848328
- DuerdenMAveryTPayneRPolypharmacy and Medicines Optimisation – Making it Safe and SoundLondonThe King’s Fund2013
- CooperJACadoganCAPattersonSMInterventions to improve the appropriate use of polypharmacy in older people: a Cochrane systematic reviewBMJ Open20155e009235
- RyanRSantessoNLoweDInterventions to improve safe and effective medicines use by consumers: an overview of systematic reviewsCochrane Database Syst Rev20144CD007768
- Royal Pharmaceutical SocietyMedicines optimisation: helping patients to make the most of medicines. Good practice guidance for healthcare professionals in England2013 Available from: http://www.rpharms.com/promoting-pharmacy-pdfs/helping-patients-make-the-most-of-their-medicines.pdfAccessed May 6, 2016
- National Institute for Health and Care ExcellenceMedicines optimisation: the safe and effective use of medicines to enable the best possible outcomes. NG52015 Available from: https://www.nice.org.uk/guidance/ng5Accessed February 10, 2017
- BokhofBJunius-WalkerUReducing polypharmacy from the perspectives of general practitioners and older patients: a synthesis of qualitative studiesDrugs Aging20163324926626915076
- MohammedMAMolesRJChenTFMedication-related burden and patients’ lived experience with medicine: a systematic review and metasynthesis of qualitative studiesBMJ Open20166116
- EtonDTElraiyahTAYostKJA systematic review of patient-reported measures of burden of treatment in three chronic diseasesPatient Relat Outcome Meas2013472023833553
- WillkeRJBurkeLBEricksonPMeasuring treatment impact: a review of patient-reported outcomes and other efficacy endpoints in approved product labelsControl Clin Trials20042553555215588741
- KrskaJKatusiimeBCorlettSAValidation of an instrument to measure patients’ experiences of medicine use: the Living with Medicines QuestionnairePatient Prefer Adherence20171167167928405159
- KatusiimeBCorlettSReeveJLKrskaJMeasuring medicines related experiences from the patient perspective: a systematic reviewPatient Relat Outcome Meas2016715717127785116
- SchafheutleEIPatients’ views on the UK policy of prescription charges – insights from qualitative interviewsRes Social Adm Pharm2008434335419064241
- Prescription Charges CoalitionPaying the price: prescription charges and people with long-term conditions2013 Available from: http://www.prescriptionchargescoalition.org.uk/uploads/1/2/7/5/12754304/paying_the_price_report.pdfAccessed March 2, 2017
- The Prescription Charges CoalitionPaying the price: prescription charges and employment2014 Available from: http://www.prescrip-tionchargescoalition.org.uk/uploads/1/2/7/5/12754304/prescription_charges_and_employment_report_feb_2014.pdfAccessed September 21, 2015
- KrskaJMorecroftCWPooleHRowePHIssues potentially affecting quality of life arising from long-term medicines use: a qualitative studyInt J Clin Pharm2013351161116923990332
- PoundPBrittenNMorganMResisting medicines: a synthesis of qualitative studies of medicine takingSoc Sci Med20056113315515847968
- BrittenNPatients’ ideas about medicines: a qualitative study in a general practice populationBr J Gen Pract1994444654687748635
- BrittenNMedicines and Society: Patients, Professionals and the Dominance of PharmaceuticalsHampshire, NYPalgrave Macmillan2008
- AnthoineEMoretLRegnaultASébilleVHardouinJ-BSample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measuresHealth Qual Life Outcomes20141217625492701
- KahnJHFactor analysis in counseling psychology research, training, and practice principles, advances, and applicationsCouns Psychol200634684718
- BeaversASLounsburyJWRichardsJKHuckSWSkolitsGJEsquivelSLPractical considerations for using exploratory factor analysis in educational researchPARE201318113
- CostelloAOsborneJBest practices in exploratory factor analysis: four recommendations for getting the most from your analysisPARE20051019
- ByrneBMStructural Equation Modeling with AMOS Basic Concepts, Applications, and Programming2nd edNew YorkTaylor and Francis Group LLC2010
- KlineRBPrinciples and Practice of Structural Equation Modeling3rd edNew YorkThe Guilford Press2011
- AtkinsonMJSinhaAHassSLValidation of a general measure of treatment satisfaction, the Treatment Satisfaction Questionnaire for Medication (TSQM), using a national panel study of chronic diseaseHealth Qual Life Outcomes200421214987333
- AtkinsonMJKumarRCappelleriJCHassSLHierarchical Construct Validity of the Treatment Satisfaction Questionnaire for Medication (TSQM Version II) among outpatient pharmacy consumersValue Health20058S92416336491
- HerdmanMGudexCLloydADevelopment and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L)Qual Life Res2011201727173621479777
- JuniperEGuyattGJaeschkeRHow to develop and validate a new health-related quality of life instrumentSpilkerBQuality of Life and Pharmacoeconomics in Clinical TrialsNew YorkRaven Press19964956
- TerweeCBBotSDMde BoerMRQuality criteria were proposed for measurement properties of health status questionnairesJ Clin Epidemiol200760344217161752
- TabachnickBGFidellLSUsing Multivariate Statistics6th edBostonPearson Education2013
- MokkinkLBTerweeCBPatrickDLThe COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi studyQual Life Res20101953954920169472
- US Department of Health and Human Services Food and Drug AdministrationGuidance for industry. Patient-reported outcome measures: use in medical product development to support labeling claims2009 Available from: www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatory-Information/Guidances/UCM193282.pdfAccessed October 30, 2015
- ZarowitzBJPolypharmacy: when is enough, enough?Geriatr Nurs20113244744922055638
- CadoganCARyanCHughesCMAppropriate polypharmacy and medicine safety: when many is not too manyDrug Safety20163910911626692396
- National Institute for Health and Care ExcellenceMultimorbidity: clinical assessment and managementNICE guideline [NG56]2016 Available from: https://www.nice.org.uk/guidance/ng56Accessed August 2, 2017
- ZidanAAwaisuAHasanSKheirNThe Living with Medicines Questionnaire: translation and cultural adaptation into the Arabic contextValue Health Reg Issues201610364027881275