Abstract
Objective
This randomized crossover trial assessed the effects of 5 weeks of consuming low-fat dairy (one serving/day each of 1% fluid milk, low-fat cheese, and low-fat yogurt) versus nondairy products (one serving/day each of apple juice, pretzels, and cereal bar) on systolic and diastolic blood pressures (SBP and DBP), vascular function (reactive hyperemia index [RHI] and augmentation index), and plasma lipids.
Methods
Patients were 62 men and women (mean age 54.5 years, body mass index 29.2 kg/m2) with prehypertension or stage 1 hypertension (mean resting SBP/DBP 129.8 mmHg/80.8 mmHg) while not receiving antihypertensive medications. A standard breakfast meal challenge including two servings of study products was administered at the end of each treatment period.
Results
Dairy and nondairy treatments did not produce significantly different mean SBP or DBP in the resting postprandial state or from premeal to 3.5 hours postmeal (SBP, 126.3 mmHg versus 124.9 mmHg; DBP, 76.5 mmHg versus 75.7 mmHg), premeal (2.35 versus 2.20) or 2 hours postmeal (2.33 versus 2.30) RHI, and premeal (22.5 versus 23.8) or 2 hours postmeal (12.4 versus 13.2) augmentation index. Among subjects with endothelial dysfunction (RHI ≤ 1.67; n = 14) during the control treatment, premeal RHI was significantly higher in the dairy versus nondairy condition (2.32 versus 1.50, P = 0.002). Fasting lipoprotein lipid values were not significantly different between treatments overall, or in subgroup analyses.
Conclusion
No significant effects of consuming low-fat dairy products, compared with low-fat nondairy products, were observed for blood pressures, measures of vascular function, or lipid variables in the overall sample, but results from subgroup analyses were consistent with the hypothesis that dairy foods might improve RHI in those with endothelial dysfunction.
Introduction
Hypertension, defined as systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg, is a common condition worldwide.Citation1 In the United States alone it affects ~31% of adults aged at least 20 years of age; 64% and 69% of men and women aged 65–74 years of age, respectively; and 72% and 81% of men and women aged 75 years and above, respectively.Citation2 Hypertension is a major risk factor for the development of stroke, coronary heart disease (CHD), heart failure, and end-stage renal disease.Citation3 Prehypertension, defined as SBP 120–139 mmHg and/or DBP 80–89 mmHg, has a prevalence of 30% in the US population.Citation4,Citation5 The designation of prehypertension was created to identify individuals at risk who might reduce their risk for progression to hypertension by adopting healthy diet and lifestyle practices.Citation4
Diet is one of the strongest environmental factors influencing blood pressure.Citation6 The Dietary Approaches to Stop Hypertension (DASH) trial demonstrated that a dietary pattern that reduced total and saturated fat intakes, included low-fat dairy products, and was rich in fruits and vegetables significantly lowered blood pressure in normotensive and hypertensive individuals.Citation7 Furthermore, the low-fat dairy-containing diet resulted in a more pronounced blood pressure-lowering effect than a diet rich in fruits and vegetables without dairy.Citation7 Results from other cross-sectional and prospective observational studies and randomized clinical trials have also suggested an inverse association between consumption of dairy products, particularly low-fat products, and the risk of developing hypertension.Citation8–Citation20 A recent meta-analysis reported a relative risk of 0.87 (95% confidence interval, 0.81–0.94) for the development of elevated blood pressure in adults consuming higher versus lower quantities of dairy.Citation19 Evidence from intervention studies examining the effects of dairy products on blood pressure is limited, but results from a recent trial of 35 healthy overweight and obese men and women indicated that daily consumption of low-fat dairy products versus carbohydrate-rich products for 8 weeks significantly reduced SBP by 2.9 mmHg (P = 0.027).Citation18
The mechanisms responsible for the association between consumption of dairy products and lower risk for hypertension have not been fully defined. Endothelial dysfunction is regarded as an early pivotal event in the development of hypertension, and has been linked to increased risk for clinical cardiovascular events such as myocardial infarction and cardiac death.Citation21 Reactive hyperemia index (RHI) values measured by peripheral arterial tomography have been shown to be predictive of cardiovascular outcomes.Citation22 A single high-fat meal produces an acute endothelial insult, as evidenced by a decline in brachial artery flow-mediated dilation after a period of occlusion-induced ischemia.Citation23–Citation31 Studies have shown that ingestion of selected foods and nutrients can reduce or prevent the acute endothelial dysfunction induced by a high-fat meal.Citation24,Citation25,Citation32–Citation36 Chaves et alCitation35 demonstrated that acute and chronic consumption by healthy normal subjects of grape products equivalent to 1.25 cups of fresh grapes did not affect heart rate, hemodynamics, or lipids, but completely prevented high-fat meal-induced endothelial dysfunction. Interventions such as aerobic exercise training, weight loss, smoking cessation, and drug therapies to treat hypertension, dyslipidemia, and hyperglycemia have also been shown to improve endothelial function.Citation37–Citation41
This study was designed to assess the effects of consuming low-fat dairy versus nondairy products on fasting and postprandial blood pressures, endothelial function, and fasting lipoprotein lipids in men and women with prehypertension or stage 1 hypertension (SBP 140–159 mmHg and/or DBP 90–99 mmHg), who were not receiving antihypertensive medication.
Methods
Study design
This randomized, controlled, two-period crossover study was conducted at Biofortis Clinical Research (Addison, IL, USA) according to Good Clinical Practice Guidelines, the Declaration of Helsinki (2000), and the United States 21 Code of Federal Regulations. It included seven clinic visits: two during screening, two at the conclusion of both 5-week treatment periods, and one after a two-week washout period between treatment periods. In addition, subjects were contacted by telephone 2 weeks into each 5-week treatment period in order to reinforce dietary instructions. The study protocol was approved by an Institutional Review Board (Quorum Review IRB, Seattle, WA, USA), and a signed informed consent form and authorization for disclosure of protected health information were obtained from all subjects before protocol-specific procedures were carried out. Subjects were informed of their right to withdraw from the study at any time.
After assessment of entry criteria, eligible subjects were randomly assigned to one of two treatment sequences: consumption of dairy products during the first 5-week treatment period and nondairy products during the second 5-week treatment period, or vice versa. The treatment periods were separated by a washout period of at least 2 weeks. During the dairy product treatment period, subjects incorporated into their diets 1 serving/day each of 1% fluid milk, low-fat cheese, and low-fat yogurt, and during the nondairy product treatment period, subjects incorporated into their diets 1 serving/day each of apple juice, pretzels, and a cereal bar (). All subjects were instructed to consume ≤1 serving/day of other dairy foods during each treatment period. A registered dietitian counseled the subjects on how to incorporate the dairy or nondairy study products into their diets while maintaining caloric balance and avoiding consumption of more than 1 serving/day of nonstudy dairy products throughout the trial. Dairy and nondairy products were provided; subjects picked up the study products approximately every 2 weeks during the study. They maintained a daily study product log and returned unconsumed servings of the study products to the clinic for determination of study product compliance.
Table 1 Nutritional composition of study products (per serving)Table Footnotea
Subjects
Participants included normally active, healthy men and postmenopausal women 20–69 years of age, inclusive, each with a body mass index of 18.5–39.9 kg/m2 and with resting blood pressure at screening meeting the criteria for prehypertension (SBP 120–139 mmHg and/or DBP 80–89 mmHg) or stage 1 hypertension (SBP 140–159 mmHg and/or DBP 90–99 mmHg). Volunteers were ineligible for participation if they had SBP ≥160 mmHg or DBP ≥100 mmHg. Subjects were also required to have a history of consumption, on average, of ≤2 servings/day of dairy foods as part of their normal diets, and to be willing to consume ≤1 serving/day of dairy foods, other than the study products provided, during each treatment phase. Additional requirements were to maintain stable body weight, habitual alcohol intake and smoking habits, physical activity patterns, use of vitamin and/or mineral supplements, and diet (other than the study products) throughout the trial. Subjects were also required to avoid vigorous physical activity and alcohol consumption 24 hours prior to each clinic visit, and to abstain from tobacco products at least 1 hour prior to and during each clinic visit.
Individuals were excluded if they had known CHD or a CHD risk equivalent including diabetes mellitus or fasting glucose ≥126 mg/dL; clinical signs of atherosclerosis including peripheral arterial disease, abdominal aortic aneurysm, carotid artery disease (symptomatic [eg, transient ischemic attack or stroke of carotid origin] or >50% stenosis on angiography or ultrasound) or other forms of clinical atherosclerotic disease (eg, renal artery disease); or the presence of multiple risk factors that confer greater than 20% probability for developing coronary artery disease within 10 years (Framingham Risk Score).Citation42 Subjects with a history of clinically important endocrine, cardiovascular, pulmonary, biliary or gastrointestinal disorders that, in the opinion of the investigator, might interfere with the interpretation of the study results were also excluded, as were those with a history of cancer in the prior 2 years (except for nonmelanoma skin cancer), history of any major trauma or major surgical event within 2 months, an active infection or taking antibiotic therapy, extreme dietary habits or a history of an eating disorder, recent history or strong potential for alcohol or substance abuse, a latex allergy or allergy/sensitivity to any of the study products or ingredients in the study products or breakfast challenge meal, or digital deformities that would prevent endothelial function measurements. Subjects who had abnormal laboratory test results of clinical importance at screening, including but not limited to total cholesterol (total-C) >300 mg/dL, triglyceride (TG) concentration ≥400 mg/dL, alanine aminotransferase or aspartate aminotransferase ≥1.5 times the upper limit of normal, and/or creatinine ≥1.5 mg/dL were also excluded.
The use of medications or dietary supplements with the potential to influence blood pressure or endothelial function; unstable use (initiation or change in dose) of lipid-altering supplements, ingredients, and/or drugs, including statins, bile acid sequestrants, cholesterol absorption inhibitors, fibrates, or prescription formulations of niacin; use of medications known to alter body weight (including over-the-counter medications) or weight loss supplements/foods; and use of meal replacement products or programs for weight loss purposes were not allowed within 4 weeks prior to screening.
Assessments
To ensure that subjects were well hydrated at each clinic visit, they were dispensed a 500 mL bottle of water and instructed to consume the full volume of water, but no other foods or beverages, the morning of their next clinic visit. Seated resting SBP, DBP, and heart rate were measured at each clinic visit; five measurements were taken, each separated by ~3 minutes, and the final four measurements were averaged (the first was discarded). Additionally, at weeks 5 and 12, subjects underwent a breakfast meal challenge by consuming two servings of their assigned study products as part of a standard breakfast meal providing approximately 600 kcal (50% carbohydrate, 15% protein, and 35% fat). Subjects were allowed 20 minutes to consume the breakfast meal. Seated resting blood pressure and heart rate were assessed premeal (t = −1.0 hour) and at t = 0.5, 1.5, 2.5, and 3.5 hours, where t = 0 hour was the start of the test meal consumption. As described above, five measurements were taken at each time point and the final four values were averaged. Additionally, endothelial function was assessed premeal (t = −0.5 hour) and at t = 2 ± 0.25 hour using the EndoPAT System (Itamar Medical, Franklin, MA, USA), which measures peripheral arterial tone (PAT) in the index fingers of both hands simultaneouslyCitation43 The RHI is a ratio of the post-to-preocclusion PAT amplitude of the tested arm, divided by the post-to-preocclusion ratio of the control arm. An augmentation index (AI), a measure of wave refection and arterial stiffness calculated as a ratio from the blood pressure waveform, was also determined.
Fasting (9–15 hours) blood samples were collected for analysis of the lipid profile [total-C, high-density lipoprotein (HDL)-C, non-HDL-C (total-C minus HDL-C), low-density lipoprotein (LDL)-C, total-C/HDL-C, and TG] at every clinic visit. Laboratory analyses were performed by Elmhurst Memorial Hospital Laboratory (Elmhurst, IL, USA). Samples were analyzed according to the Standardization Program of the Centers for Disease Control and Prevention and the National Heart, Lung and Blood Institute. LDL-C concentration in mg/dL was calculated according to the Friedewald equationCitation44 as follows: LDL-C = total-C − HDL-C − TG/5. This equation is not valid when the TG concentration is >400 mg/dL; therefore, LDL-C was not calculated under those circumstances. Subjects also collected 24-hour urine samples the day prior to the final clinic visit of each treatment period (weeks 5 and 12). Urine samples were analyzed for creatinine, electrolytes, and minerals (sodium, potassium, magnesium, chloride, and calcium). Adverse events and body weight were also assessed at each clinic visit.
Subjects completed 3-day diet records recording all foods and beverages consumed in the 3 days prior to the baseline visit and at the end of each treatment period (weeks 5 and 12). The diet record from the baseline visit was given back to the subjects with instructions to replicate the same food and beverage choices, other than the study products consumed, where appropriate, on the day prior to the clinic visits at weeks 4, 5, 11, and 12. Analysis of diet records was performed using Food Processor® SQL Nutrition Analysis and Fitness Software (version 10.4.0, ESHA Research, Salem, OR, USA).
Statistical analyses
Statistical programming and analyses were performed using SAS for Windows, version 9.2 (SAS Institute, Cary, NC, USA). All tests of significance, unless otherwise stated, were performed at alpha = 0.05, two-sided. The targeted evaluable sample size of 57 subjects was expected to provide 80% power to detect a difference of 2.6 mmHg in SBP (total area under the curve [AUC] divided by 3.5 hours), assuming a pooled standard deviation of 6.8 mmHg for the SBP response (standardized effect size of 0.38).Citation18
Demographic, baseline, and safety analyses were performed on data collected from all subjects who were randomized and consumed at least one dose of study product. Efficacy evaluable analyses were performed on the sample of subjects who were randomized and provided at least one postrandomization outcome data point during each treatment phase. In addition, efficacy analyses were performed on data from the per protocol population, identified as a subset of the efficacy evaluable population, in which subjects were excluded for reasons such as violations of inclusion or exclusion criteria or noncompliance with the study protocol. The results from the efficacy evaluable sample are described herein; per protocol results did not differ materially and are therefore not presented.
Baseline comparability of treatment sequence groups for demographic, lipid parameters, and blood pressure variables were assessed by analysis of variance (ANOVA) or chi-square tests. The primary outcome variable was the total AUC for SBP for the two test conditions obtained premeal and at postmeal time points divided by 3.5 to obtain an average value throughout the test period. Secondary outcome variables included a comparable calculation for DBP, RHI, and AI for the two test conditions premeal and at 2 hours after the start of meal consumption, SBP and DBP at each of the time points, as well as percent changes from baseline (average of weeks −1 and 0) to end of each treatment (average of weeks 4 and 5 and average of weeks 11 and 12) in the fasting lipid profile variables. Differences between conditions in responses were assessed using SAS Proc Mixed repeated measures ANOVA. Initial repeated measures ANOVA models contained terms for treatment, sequence, and treatment by sequence, with subject as a random effect. Models were reduced in a stepwise manner until only significant (P < 0.05) terms or treatment remained in the model. Assumptions of normality of residuals were investigated for each response measurement. In cases where the normality assumption was rejected at the 1% level with the Shapiro-Wilks test,Citation45 an analysis using ranks was performed. Examination of responses by sequence suggested that no material differences were present that would bring into question the appropriateness of pooling data from the two sequence groups. Differences in the incidence of adverse events between treatments were assessed with McNemar’s test.Citation46
Subgroup analyses were conducted to examine responses in blood pressure and endothelial function in subjects with prehypertension versus stage 1 hypertension, age (split at the median, ≤54 years and >54 years of age), body mass index (split at the median ≤28.5 kg/m2 and >28.5 kg/m2), non-Hispanic white versus those with other race/ethnicity, and baseline (premeal assessment during the nondairy phase) RHI ≤ 1.67 or >1.67. The cut-point of ≤1.67 is recommended by the manufacturer of the EndoPAT device, to define endothelial dysfunction.Citation47,Citation48
Results
Of the 121 individuals screened for participation in the study, 73 were randomized and included in the safety population, and 62 subjects completed the study (29 in the dairy/nondairy sequence and 33 in the nondairy/dairy sequence) and were included in the efficacy evaluable population. Of the eleven subjects who discontinued from the study, six withdrew consent, two were lost to follow-up, one discontinued due to starting blood pressure medication use during the trial, one was removed from the trial due to noncompliance, and one subject discontinued due to an adverse event classified as moderate dyspepsia, which was judged by the study physician to probably be related to consumption of the study products.
Demographic and baseline characteristics of all randomized subjects are listed in . The majority of subjects were non-Hispanic white (68%) and male (55%) with average age of 54.7 years and body mass index of 29.2 kg/m2. Mean baseline SBP and DBP were in the prehypertension range, 130 mmHg and 81 mmHg, respectively, reflecting that the majority of participants had prehypertension (84%), and fewer had stage 1 hypertension (16%). Overall median (interquartile limits) compliance with consumption of study products was 100% (99.0%, 103%) during the dairy products treatment and 100% (98.1%, 102%) during the nondairy products treatment (P = 0.149); because subjects were provided with more servings of study food than were required, some consumed slightly more than the recommended three servings on some days. Mean ± SEM body weight was not different during dairy (86.2 kg ± 2.0 kg) and nondairy treatments (86.2 kg ± 2.1 kg).
Table 2 Baseline demographic, anthropometric, and hemodynamic characteristics of subjects
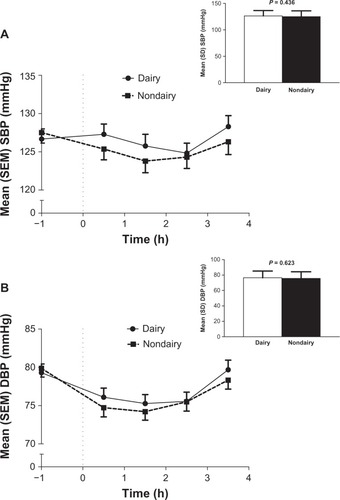
Mean SBP and DBP values from before the meal challenge (−1.0 hour) through time points up to 3.5 hours after consumption of the test meal (calculated as total AUC divided by 3.5 hours) are shown in and , respectively. There were no significant differences between dairy and nondairy treatments in mean SBP or DBP from premeal to 3.5 hours postmeal (SBP, 126.3 mmHg versus 124.9 mmHg; DBP, 76.5 mmHg versus 75.7 mmHg).
Figure 1 Mean systolic (A) and diastolic (B) blood pressure values at time points throughout a meal challenge test and overall mean (inset) for dairy and nondairy treatments (N = 62). The average blood pressure was calculated as total AUC0–3.5 h (h × mmHg) or divided by 3.5 h (inset).
RHI and AI for dairy and nondairy treatments before and after a meal challenge in all subjects, and in the subgroup of 14 subjects with premeal endothelial dysfunction during the control condition (defined as RHI ≤ 1.67), are shown in . There were no significant differences between dairy and nondairy treatments in premeal or 2 hours postmeal values in the overall sample. Among subjects with endothelial dysfunction who had a mean age of 56.7 years and resting SBP/DBP of 128.1 mmHg/79.5 mmHg, the mean ± SEM premeal RHI value was significantly higher in the dairy condition compared to the nondairy condition (2.32 ± 0.19 versus 1.50 ± 0.04; P = 0.002). Mean SBP and DBP values from premeal to 3.5 hours postmeal (SBP, 124.1 mmHg versus 121.3 mmHg; DBP, 75.5 mmHg versus 73.1 mmHg) did not differ significantly between treatments in this subgroup, nor did fasting lipoprotein lipids (data not shown). Other subgroup analyses showed no significant differences between subjects with prehypertension and stage 1 hypertension, older and younger subjects, individuals with body mass index above or below the median, or between non-Hispanic white subjects and those of other race/ethnicity categories in any of the blood pressure or vascular function parameters measured (data not shown).
Table 3 EndoPAT reactive hyperemia and augmentation indices of endothelial function for dairy and nondairy treatments before and after a meal challenge
Fasting lipoprotein lipid (total-C, LDL-C, HDL-C, non-HDL-C, and TG) analyses of the overall sample indicated that dairy and nondairy treatments did not produce significantly different lipid responses (). Dietary energy, macronutrient, and mineral intakes at baseline and during each treatment condition are presented in . During the dairy treatment, subjects consumed significantly greater percentages of protein, total fat and saturated fatty acids, as well as greater amounts of calcium, magnesium, and potassium, and significantly less carbohydrate and dietary fiber compared to the nondairy treatment. Creatinine-adjusted concentrations of magnesium, calcium, chloride, potassium, and sodium in 24-hour urine samples were not significantly different between dairy and nondairy treatments in the overall sample, or in the subgroup with endothelial dysfunction (data not shown).
Table 4 Fasting lipids at baseline and percent changes from baseline to the end of each treatment period after dairy and nondairy conditions (N = 62)
Table 5 Intake of energy, macronutrients, and minerals at baseline and during dairy and nondairy treatment periods
Adverse events were experienced by 9 (12.3%) subjects during the dairy treatment and 12 (16.4%) subjects during the nondairy treatment (P = 0.140). None of the events were serious and all were classified as mild or moderate in severity. The most common adverse event was upper respiratory tract infection, reported by 4 (5.5%) subjects in the dairy condition and 3 (4.1%) subjects in the nondairy condition. One report of abdominal pain during the dairy condition was judged by the study physician to be probably related to consumption of study products, and five events during the nondairy condition were considered to be possibly or probably related to treatment [dyspepsia (n = 1), flatulence (n = 1), hypertension (n = 1), and weight increase (n = 2)]. All other events were described as unrelated or unlikely to be related to consumption of study products.
Discussion
This randomized, crossover trial failed to demonstrate a significant effect of 5 weeks consumption of low-fat dairy products versus low-fat nondairy products on SBP and DBP, vascular function, or plasma lipids in men and postmenopausal women with prehypertension or stage 1 hypertension. However, among the subgroup of subjects with endothelial dysfunction, defined as baseline RHI ≤ 1.67,Citation47,Citation48 the RHI measured immediately prior to a meal challenge administered at the end of each treatment period was significantly higher in the dairy versus nondairy condition (2.32 versus 1.50, P = 0.002). A higher degree of reactive hyperemia is consistent with the hypothesis that dairy foods might be of value for improving endothelial function in those with endothelial dysfunction. However, this result should be interpreted with caution because, similar to what was shown in the overall analysis, blood pressures did not differ between the two treatment conditions, nor did the 2-hour-postmeal RHI values.
Results from the DASH trialCitation7 and several other cross-sectional and prospective cohort studies support an inverse association between chronic consumption of dairy products (most often low-fat dairy products) and blood pressure.Citation8–Citation14,Citation16,Citation17,Citation19,Citation20 A recent meta-analysis reported a 13% reduction in the risk for the development of elevated blood pressure in adults consuming higher versus lower quantities of dairy.Citation19 However, results in the literature regarding the relationship between dairy consumption and blood pressure are not entirely consistent, in part due to the wide variety of types of foods classified as dairy products (liquid and solid, low fat and whole fat, fermented and nonfermented)Citation49 and likely also due to the age and health of the individuals examined. An intervention trial of 8 weeks consumption of low-fat dairy versus carbohydrate-rich control products by overweight and obese men and women produced a significant SBP-lowering effect (−2.9 mmHg compared with the control period, P = 0.027),Citation18 but some clinical studies conducted in healthy older adults and in young normotensive adults have failed to detect an effect of fluid milk or low-fat dairy products on blood pressure.Citation50–Citation52
To the authors’ knowledge, this is the first clinical investigation of the effects of consumption of low-fat dairy products on RHI and AI. The effect of total dairy intake on arterial stiffness was recently examined by Crichton et alCitation53 in a cross-sectional analysis of a subset of the Maine-Syracuse Longitudinal Study. A linear decrease in carotid-femoral pulse wave velocity was observed across increasing intakes of dairy food consumption (ranging from never/rarely to daily dairy food intake).
Subjects in the present trial consumed 1 serving per day each of low-fat milk, cheese, and yogurt, which is in accordance with the American Heart Association recommendations to consume 2–3 servings/day of low-fat dairy products,Citation54 but the different nutrient compositions of these dairy foods may have heterogeneous effects on blood pressure.Citation55 In their meta-analysis, Ralston et alCitation19 examined specific categories of dairy foods and found that consumption of fluid dairy foods (including low-fat and full-fat milk and yogurt) was associated with an 8% reduction in the risk for elevated blood pressure (relative risk 0.92; 95% confidence interval, 0.87–0.98), whereas cheese consumption was not significantly associated with risk.Citation19 In the present trial, the inclusion of cheese may have attenuated the effects of milk and yogurt on blood pressure and/or endothelial function. Milk and other fluid dairy foods have higher potassium and lower sodium content than cheese, which may partly explain the lack of association between blood pressure and cheese consumption. Sodium is considered to be a pivotal dietary factor in the development of hypertension,Citation56 and in the DASH sodium study,Citation57 among others, reducing sodium intake decreased blood pressure. Conversely, potassium intake has been shown to have an inverse relationship with the risk for developing hypertension. A meta-analysis of randomized trials that evaluated the effects of increased potassium intake on blood pressure concluded that potassium supplementation (average of at least 60 mmol per day) lowered SBP and DBP by 4.4 and 2.5 mmHg, respectively, in hypertensive subjects, and by 1.8 and 1.0 mmHg in normotensive subjects.Citation58 In the DASH trial, a diet rich in fruits and vegetables, compared with the typical American diet, reduced SBP and DBP at a constant level of sodium intake.Citation7 The potassium content of the fruit and vegetable diet was more than twice that of the typical American diet, and this higher potassium:sodium ratio was speculated to account, at least in part, for the observed reduction in blood pressure. Several components in dairy foods are suspected of modulating the relationship between dairy consumption and blood pressure.Citation59 The majority of research results point to the benefits of increased calcium for maintaining smooth muscle tone in blood vessels.Citation60–Citation62 In the Women’s Health Study, consumption of dairy calcium, but not calcium supplementation, was associated with reduced risk of hypertension,Citation13 suggesting that other dairy food components such as magnesium,Citation63 potassium,Citation56 and vitamin DCitation64 could also play important roles.
Lactopeptides, bioactive peptides released during milk protein digestion (or during food processing), may also be involved in the relationship between dairy consumption and blood pressure.Citation65–Citation69 These inhibit the action of angiotensin I converting enzyme, thus reducing blood levels of angiotensin, preventing blood vessel constriction, and modulating endothelial function. Ballard et alCitation68 demonstrated that 2 weeks’ consumption of 5 grams per day of a novel whey-derived peptide (NOP-47) by healthy subjects significantly improved brachial artery flow-mediated dilation responses. Certain peptides derived from milk proteins may also modulate enothelin-1 release by endothelial cells.Citation70 Endothelins are proteins that constrict blood vessels, thereby raising blood pressure. The importance of dietary phosphorous for lowering blood pressure was also recently suggested.Citation71
In the present trial, total and saturated fat intakes were significantly higher in the dairy (30.0% and 9.9% of energy, respectively) versus nondairy treatments (26.9% and 8.1%, respectively), but intakes during both conditions were lower than at baseline (33.4% and 10.5%, respectively), and there was no apparent effect of the consumption of dairy versus nondairy products on lipid levels. There is a widespread, though not fully substantiated, belief that consumption of milk, which can contain significant quantities of saturated fat, increases plasma cholesterol concentration and risk for vascular disease.Citation6,Citation55,Citation72,Citation73 In the present study, no adverse effects were noted for lipids, blood pressure, or vascular function during the dairy and nondairy food treatment periods, despite greater total and saturated fat intakes during dairy food consumption.
In the meta-analysis by Ralston et al,Citation19 a comparison of low-fat versus whole-fat dairy foods indicated a 16% reduction in the risk for elevated blood pressure associated with low-fat dairy foods and no association with whole-fat dairy foods, resulting in an overall reduction in risk associated with total dairy foods of 13%. It has been proposed that when consumed with fat, the bivalent cations of calcium and magnesium in dairy products (both of which have been shown to be inversely associated with blood pressure and risk of developing hypertension) bind to fatty acids in the small intestine, forming insoluble soaps and partially preventing absorption of these minerals.Citation10,Citation74 The reduced mineral absorption might diminish the efficacy of whole-fat dairy products for lowering blood pressure. The processing of skim milk from whole milk introduces other changes in the nutritional composition besides simply removing the fat, and this could also contribute to the difference in blood pressure responses between low-fat and whole-fat dairy foods.Citation13 Individuals who consume more low-fat dairy foods also tend to have a healthier lifestyle than those who consume full-fat dairy foods, which may confound observational analyses of dairy intake. Additional research is necessary to more fully understand the relationship between consumption of dairy products and blood lipids.
Prior research regarding the induction of acute postprandial endothelial dysfunction has focused on changes in endothelial function and oxidative stress that occur 2–3 hours after a single high-fat or high-carbohydrate meal.Citation23–Citation25,Citation27,Citation31 The amount of fat administered in the high-fat meals typically ranges between ~35% and 50% of calories.Citation25,Citation26,Citation28–Citation30 In the present study, the standard meal provided 35% of calories as fat. Although the meal challenge appeared to induce endothelial dysfunction based on a nearly 50% decrease in the AI from premeal to postmeal, the RHI in both treatment conditions changed very little from premeal to postmeal. This brings into question whether the meal challenge was a sufficient “endothelial insult” from which to detect an acute effect of the dairy versus nondairy products, and whether 2 hours postmeal was the most appropriate postprandial time point for assessment.
A limitation of the present investigation is that the subjects studied had, as a group, mild blood pressure elevation and a low prevalence of endothelial dysfunction. Subjects were selected based on their blood pressure status of pre-hypertension (84%) or stage 1 hypertension (16%), but according to their baseline RHI scores (overall mean ~2.3) the subjects had relatively healthy endothelial responses. The results for the 14 subjects with endothelial dysfunction (RHI ≤ 1.67) suggest that a significant association between dairy intake and blood pressure and vascular measures might have been detectable in a larger sample selected specifically for the presence of endothelial dysfunction.
Conclusion
In conclusion, these results showed that among men and women with prehypertension or stage 1 hypertension, there were no significant effects of consuming low-fat dairy products, compared with nondairy products, on blood pressure, measures of vascular function, or lipid variables. However, in a subgroup of subjects with baseline endothelial dysfunction, the premeal RHI was significantly higher in the dairy versus nondairy condition. Further research is warranted to investigate the possibility that the consumption of dairy products might be of value for improving endothelial function in subjects selected for the presence of endothelial dysfunction at baseline.
Acknowledgments
This study was funded by Dairy Research Institute, Rosemont, IL. The authors also wish to thank Valerie Kaden and Kristen Sanoshy, MPH, RHIA, both with Biofortis Clinical Research, for their assistance with project oversight and data collection.
Disclosure
The authors report no conflicts of interest in this work. KC Maki, TM Rains, AL Schild, MR Dicklin, AL Lawless, and KM Kelley as employees of Biofortis Clinical Research received a research grant from Dairy Research Institute to conduct this research. KM Park was an employee of Dairy Research Institute/National Dairy Council at the time the study was initiated.
References
- KearneyPMWheltonMReynoldsKMuntnerPWheltonPKHeJGlobal burden of hypertension: analysis of worldwide dataLancet2005365945521722315652604
- Health, United States2011With Special Feature on Socioeconomic Status and HealthHyattsville (MD)National Center for Health Statistics (US)52012 Available from: http://www.cdc.gov/nchs/data/hus/hus11.pdfAccessed June 11, 2013
- US Department of Health and Human ServicesNational Institutes of Health National Heart, Lung, and Blood InstituteNational High Blood Pressure Education ProgramThe Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure NIH Publication No 04-523082004
- ChobanianAVBakrisGLBlackHRThe Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 reportJAMA2003289192560257212748199
- HsiaJMargolisKLEatonCBWomen’s Health Initiative InvestigatorsPrehypertension and cardiovascular disease risk in the Women’s Health InitiativeCirculation2007115785586017309936
- AppelLJBrandsMWDanielsSRDietary approaches to prevent and treat hypertension: a scientific statement from the American Heart AssociationHypertension200647229630816434724
- AppelLJMooreTJObarzanekEA clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research GroupN Engl J Med199733616111711249099655
- MillerGDDiRienzoDDReusserMEMcCarronDABenefits of dairy product consumption on blood pressure in humans: a summary of the biomedical literatureJ Am Coll Nutr200019Suppl 2147S164S10759140
- PereiraMAJacobsDRJrVan HornLSlatteryMLKartashovAILudwigDSDairy consumption, obesity, and the insulin resistance syndrome in young adults: the CARDIA StudyJAMA2002287162081208911966382
- AlonsoABeunzaJJDelgado-RodríquezMMartínezJAMartínez-GonzálezMALow-fat dairy consumption and reduced risk of hypertension: the Seguimiento Universidad de Navarra (SUN) cohortAm J Clin Nutr200582597297916280427
- RuidavetsJBBongardVSimonCIndependent contribution of dairy products and calcium intake to blood pressure variations at a population levelJ Hypertens200624467168116531795
- SnijderMBvan der HeijdenAAvan DamRMIs higher dairy consumption associated with lower body weight and fewer metabolic disturbances? The Hoorn StudyAm J Clin Nutr200785498999517413097
- WangLMansonJEBuringJELeeIMSessoHDDietary intake of dairy products, calcium, and vitamin D and the risk of hypertension in middle-aged and older womenHypertension20085141073107918259007
- EngberinkMFHendriksenMASchoutenEGInverse association between dairy intake and hypertension: the Rotterdam StudyAm J Clin Nutr20098961877188319369377
- HilpertKFWestSGBagshawDMEffects of dairy products on intracellular calcium and blood pressure in adults with essential hypertensionJ Am Coll Cardiol2009282142149
- Kris-EthertonPMGriegerJAHilpertKFWestSGMilk products, dietary patterns and blood pressure managementJ Am Coll Nutr200928Suppl 1103S119S19571168
- ToledoEDelgado-RodríguezMEstruchRLow-fat dairy products and blood pressure: follow-up of 2290 older persons at high cardiovascular risk participating in the PREDIMED studyBr J Nutr20091011596718492300
- van MeijlLMensinkRLow-fat dairy consumption reduces systolic blood pressure, but does not improve other metabolic risk parameters in overweight and obese subjectsNutr Metab Cardiovasc Dis201121535536120153619
- RalstonRALeeJHTrubyHPalermoCEWalkerKZA systematic review and meta-analysis of elevated blood pressure and consumption of dairy foodsJ Hum Hypertens201226131321307883
- Soedamah-MuthuSSVerberneLDDingELEngberinkMFGeleijnseJMDairy consumption and incidence of hypertension: a dose-response meta-analysis of prospective cohort studiesHypertension20126051131113722987924
- DharmashankarKWidlanskyMEVascular endothelial function and hypertension: insights and directionsCurr Hypertens Rep201012644845520857237
- RubinshteinRKuvinJTSofferMAssessment of endothelial function by non-invasive peripheral arterial tonometry predicts late cardiovascular adverse eventsEur Heart J20103191142114820181680
- VogelRACorrettiMCPlotnickGDEffect of a single high-fat meal on endothelial function in healthy subjectsAm J Cardiol19977933503549036757
- PlotnickGDCorrettiMCVogelRAEffect of antioxidant vitamins on the transient impairment of endothelium-dependent brachial artery vasoactivity following a single high-fat mealJAMA199727820168216869388088
- PlotnickGDCorrettiMCVogelRAHesslinkRJrWiseJAEffect of supplemental phytonutrients on impairment of the flow-mediated brachial artery vasoactivity after a single high-fat mealJ Am Coll Cardiol200341101744174912767658
- CuevasAMGuaschVCastilloOA high-fat diet induces and red wine counteracts endothelial dysfunction in human volunteersLipids200035214314810757544
- NappoFEspositoKCioffMPostprandial endothelial activation in healthy subjects and in type 2 diabetic patients: role of fat and carbohydrate mealsJ Am Coll Cardiol20023971145115011923038
- TushuizenMENieuwlandRSchefferPGSturkAHeineRJDiamantMTwo consecutive high-fat meals affect endothelial-dependent vasodilation, oxidative stress and cellular microparticles in healthy menJ Thromb Haemost2006451003101016689751
- BerrySETuckerSBanerjiRImpaired postprandial endothelial function depends on the type of fat consumed by healthy menJ Nutr2008138101910191418806100
- AyerJGHarmerJASteinbeckKCelermajerDSPostprandial vascular reactivity in obese and normal weight young adultsObesity (Silver Spring)201018594595119834470
- BarrigerTAHatcherLSasserHCPotential benefits on impairment of endothelial function after a high-fat meal of 4 weeks of flavonoid supplementationEvid Based Complement Alternat Med2011201179695818955351
- KatzDLNawazHBoukhalilJAcute effects of oats and vitamin E on endothelial responses to ingested fatAm J Prev Med200120212412911165454
- LingLZhaoS PGaoMZhouQCLiYLXiaBVitamin C preserves endothelial function in patients with coronary heart disease after a high-fat mealClin Cardiol200225521922412018880
- CortésBNuñezICofánMAcute effects of high-fat meals enriched with walnuts or olive oil on postprandial endothelial functionJ Am Coll Cardiol20064881666167117045905
- ChavesAAJoshiMSCoyleCMVasoprotective endothelial effects of a standardized grape product in humansVascul Pharmacol2009501–2202618805507
- KatoTInoueTNodeKPostprandial endothelial dysfunction in subjects with new-onset type 2 diabetes: an acarbose and nateglinide comparative studyCardiovasc Diabetol201091220334663
- VehkavaaraSMäkimattilaSSchlenzkaAVakkilainenJWesterbackaJYki-JärvinenHInsulin therapy improves endothe-lial function in type 2 diabetesArterioscler Thromb Vasc Biol200020254555010669655
- GuvenGSAtalarEYavuzBSimvastatin treatment improves endothelial function and increases fibrinolysis in patients with hypercholesterolemiaJ Natl Med Assoc200698462763016623076
- HosokawaSHiasaYMiyazakiSEffects of smoking cessation on coronary endothelial function in patients with recent myocardial infarctionInt J Cardiol20081281485217643513
- TyldumGASchjerveIETjønnaAEEndothelial dysfunction induced by post-prandial lipemia: complete protection afforded by high-intensity aerobic interval exerciseJ Am Coll Cardiol200953220020619130989
- BigorniaSJMottMMHessDTLong-term successful weight loss improves vascular endothelial function in severely obese individualsObesity (Silver Spring)201018475475920057371
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III)Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final reportCirculation2002106253143342112485966
- KuvinJTPatelARSlineyKAAssessment of peripheral vascular endothelial function with finger arterial pulse wave amplitudeAm Heart J2003146116817412851627
- FriedewaldWTLevyRIFredricksonDSEstimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifugeClin Chem19721864995024337382
- ShapiroSSWilkMBAn analysis of variance test for normality (complete samples)Biometrika1965523–4591611
- McNemarQNote on the sampling error of the difference between correlated proportions or percentagesPsychometrika19471215315720254758
- BonettiPOPumperGMHiganoSTHolmesDRJrKuvinJTLermanANoninvasive identification of patients with early coronary atherosclerosis by assessment of digital reactive hyperemiaJ Am Coll Cardiol200444112137214115582310
- Itamar-Medical.com [webpage on the Internet] Available from: http://www.itamar-medical.com/EndoPAT/FAQ.htmlAccessed March 19, 2013
- McGraneMMEsseryEObbagyJDairy consumption, blood pressure, and risk of hypertension: an evidence-based review of recent literatureCurr Cardiovasc Risk Rep20115428729822384284
- BarrSIMcCarronDAHeaneyRPEffects of increased consumption of fluid milk on energy and nutrient intake, body weight, and cardiovascular risk factors in healthy older adultsJ Am Diet Assoc2000100781081710916520
- SteffenLMKroenkeCHYuXAssociations of plant food, dairy product, and meat intakes with 15-y incidence of elevated blood pressure in young black and white adults: the Coronary Artery Risk Development in Young Adults (CARDIA) StudyAm J Clin Nutr20058261169117716332648
- AlonsoAZozayaCVázquezZAlfredo MartínezJMartínez-GonzálezMAThe effect of low-fat versus whole-fat dairy product intake on blood pressure and weight in young normotensive adultsJ Hum Nutr Diet200922433634219486260
- CrichtonGEEliasMFDoreGAAbhayaratnaWPRobbinsMARelations between dairy food intake and arterial stiffness: pulse wave velocity and pulse pressureHypertension20125951044105122431583
- Heart.org [webage on the Internet] Available at: http://www.heart.org/HEARTORG/GettingHealthy/NutritionCenter/HealthyDietGoals/Suggested-Servings-from-Each-Food-Group_UCM_318186_Article.jspAccessed March 19, 2013
- GibsonRAMakridesMSmithersLGVoevodinMSinclairAJThe effect of dairy foods on CHD: a systematic review of prospective cohort studiesBr J Nutr200910291267127519682399
- AndroguéHJMadiasNESodium and potassium in the pathogenesis of hypertensionN Engl J Med2007356191966197817494929
- SacksFMSvetkeyLPVollmerWMEffects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) dietN Engl J Med200134431011136953
- WheltonPKHeJCutlerJAEffects of oral potassium on blood pressure: meta-analysis of randomized controlled clinical trialsJAMA1997277162416329168293
- RiceBHCifelliCJPiloskyMAMillerGDDairy components and risk factors for cardiometabolic syndrome: recent evidence and opportunities for future researchAdv Nutr20112539640722332081
- AllenderPSCutlerJAFollmannDCappuccioFPPryerJElliottPDietary calcium and blood pressure: a meta-analysis of randomized clinical trialsAnn Intern Med199612498258318610952
- BucherHCCookRJGuyattGHEffects of dietary calcium supplementation on blood pressure: a meta-analysis of randomized controlled trialsJAMA199627513101610228596234
- GriffithLEGuyattGHCookRJBucherHCCookDJThe influence of dietary and non-dietary calcium supplementation on blood pressure: an updated meta-analysis of randomized controlled trialsAm J Hypertens1999121 Pt 1849210075392
- JeeSHMillerER3rdGuallarESinghVKAppelLJKlagMJThe effect of magnesium supplementation on blood pressure: a meta-analysis of randomized clinical trialsAm J Hypertens200215869169612160191
- NemerovskiCWDorschMPSimpsonRUBoneHGAaronsonKDBleskeBEVitamin D and cardiovascular diseasePharmacotherapy200929669170819476421
- ClareDASwaisgoodHEBioactive milk peptides: a prospectusJ Dairy Sci20008361187119510877382
- FitzGeraldRJMurrayBAWalshDJHypotensive peptides from milk proteinsJ Nutr20041344980S988S15051858
- SéverinSWenshuiXMilk biologically active components as nutraceuticals: reviewCrit Rev Food Sci Nutr2005457–864565616371332
- BallardKDBrunoRSSeipRLAcute ingestion of a novel whey-derived peptide improves vascular endothelial responses in healthy individuals: a randomized, placebo controlled trialNutr J200983419624856
- BoelsmaEKloekJLactotripeptides and antihypertensive effects: a critical reviewBr J Nutr2009101677678619061526
- MaesWVan CampJVermeirssenVInfluence of the lactokinin Ala-Leu-Pro-Met-His-Ile-Arg (ALPMHIR) on the release of endothelin-1 by endothelial cellsRegul Pept20041181–210510914759563
- AlonsoANettletonJAIxJHDietary phosphorous, blood pressure, and incidence of hypertension in the Atherosclerosis Risk In Communities study and the Multi-Ethnic Study of AtherosclerosisHypertension201055377678420083730
- GermanJBGibsonRAKraussRMA reappraisal of the impact of dairy foods and milk fat on cardiovascular disease riskEur J Nutr200948419120319259609
- ElwoodPCPickeringJEGivensDIGallacherJEThe consumption of milk and dairy foods and the incidence of vascular disease and diabetes: an overview of the evidenceLipids20104592593920397059
- VaskonenTDietary minerals and modifications of cardiovascular risk factorsJ Nutr Biochem200314949250614505811