
ABSTRACT
Background: Many individuals with alcohol-use disorders who had experienced alcohol craving before joining Alcoholics Anonymous (AA) report little or no craving after becoming long-term members. Their use of AA prayers may contribute to this. Neural mechanisms underlying this process have not been delineated. Objective: To define experiential and neural correlates of diminished alcohol craving following AA prayers among members with long-term abstinence. Methods: Twenty AA members with long-term abstinence participated. Self-report measures and functional magnetic resonance imaging of differential neural response to alcohol-craving-inducing images were obtained in three conditions: after reading of AA prayers, after reading irrelevant news, and with passive viewing. Random-effects robust regressions were computed for the main effect (prayer > passive + news) and for estimating the correlations between the main effect and the self-report measures. Results: Compared to the other two conditions, the prayer condition was characterized by: less self-reported craving; increased activation in left-anterior middle frontal gyrus, left superior parietal lobule, bilateral precuneus, and bilateral posterior middle temporal gyrus. Craving following prayer was inversely correlated with activation in brain areas associated with self-referential processing and the default mode network, and with characteristics reflecting AA program involvement. Conclusion: AA members’ prayer was associated with a relative reduction in self-reported craving and with concomitant engagement of neural mechanisms that reflect control of attention and emotion. These findings suggest neural processes underlying the apparent effectiveness of AA prayer.
Introduction
Alcoholics Anonymous (AA) is an abstinence-oriented fellowship with over 1.2 million members in the United States, of which 73% report over 1 year of abstinence, and attend an average of 2.6 meetings weekly (Citation1). Narcotics Anonymous also employs the Twelve Step approach, and meeting attendees report an average of 6.1 years of abstinence (Citation2).
The majority of long-term Twelve Step members who we have surveyed report no alcohol or drug craving; for AA, 70% reported no craving for alcohol (Citation3,Citation4), and for NA, 49% reported no craving for alcohol or drugs (Citation2). This is notable, since people joining and persisting in attending these fellowship meetings are among the more severely addicted, having suffered from considerable craving for their principal substances of use. In fact, “craving, or a strong desire to use alcohol (or another drug)” is one of the formal criteria for diagnosing an addiction in the diagnostic manual of the American Psychiatric Association (Citation5). Unlike other criteria, it is listed as potentially persisting, even in an addicted person in remission. In light of this, a framework based on recent neural findings can be constructed to encompass the impact of the Twelve Step experience on the recovery process (Citation6). The diminution of craving in long-term Twelve Step members therefore merits investigation to ascertain the nature of craving, an important aspect of persistent remission.
Craving
Assessments of cue reactivity and craving have typically been conducted on subjects who are either non-treatment seeking, in a detoxification unit, or in treatment, as reflected in a recent review of 28 such studies (Citation7). Findings in these studies illustrate how craving is triggered in association with enhanced dopamine signaling in subjects with deficits in dopamine activity and acquired prefrontal and striatal reward dysregulation (Citation8). This mechanism also impacts on a clinical level, individuals with alcohol-use disorders who have entered treatment. Their self-reports of temptation to drink were predictive of subsequent relapse (Citation9). Similarly, on a neurophysiological level, the degree of activation in the ventromedial prefrontal cortex (vmPFC) was correlated with the induced craving during neutral-relaxing trials, and was also predictive of subsequent relapse (Citation10).
Nonetheless, there is evidence that both self- and therapist-initiated interventions can alter the relationship between cue exposure and craving. Smokers can be taught cognitive strategies to control craving, resulting in activation in prefrontal areas reflecting active control, with diminished activation in limbic areas associated with use of the drug (Citation11). Similarly, for individuals with alcohol-use disorders expression of change talk following motivational interviewing can result in inhibition in brain regions that respond to the alcohol cues (Citation12).
Prayer and craving
The practice of prayer is quite common in the United States; 57% of Americans report that they pray every day (Citation13). Among AA members surveyed, the figure was even higher, 73% (Citation14). Effects of prayer on brain functioning have been studied in circumstances unrelated to drinking, demonstrating how, on imaging, participants’ experience of communicating with God taps into areas associated with interpersonal communication (Citation15). Overlap in specific brain regions that are activated during prayer to God and while speaking to a loved one among religious Christian subjects have been associated with Theory of Mind, including medial prefrontal cortex, the posterior cingulate cortex, and the parietal lobe at the temporo-parietal junction (Citation15).
Consideration of whether prayer can serve acutely as a means of avoiding alcohol-craving has not been addressed empirically. There are, however, studies which may shed light on this. Regarding alcoholism, Kaskutas et al. (Citation16) reported that the experience of a spiritual awakening among individuals with alcohol-use disorders was associated with diminished alcohol use following treatment. In another study, participants who were assigned to engage in prayer (unrelated to drinking) every day for four weeks drank about half as much as those who were not (Citation17).
Top-down and bottom-up control
The management of responses to external and internal stimuli occurs either in a top-down voluntary or bottom-up involuntary fashion. The dorso-lateral prefrontal cortex, intra-parietal sulcus and frontal eye field areas are involved in the slower more effortful top-down voluntary cognitive processes, such as conscious decision making, goal maintenance and voluntary attention; while bilateral insular cortex, anterior cingulate cortex, ventromedial prefrontal and orbitofrontal cortex, inferior frontal gyrus and inferior parietal lobule, are involved in a more automatic bottom-up involuntary processes, such as salience detection, interoception, conflict monitoring and resolution, reward valuation, and involuntary attention (Citation18–Citation20). Control of emotion in the brain is likewise thought to occur via two such different groups of areas, the dorsal voluntary and the ventral involuntary one. They are commonly seen as forming two distinct networks in the brain (Citation21).
Addiction is thought to dysregulate both groups of the above-mentioned areas, biasing excessively the bottom-up salience areas toward processing of substance related cues, and impairing emotion regulation, while causing a hypofunction of cognitive control areas, except during the acute stages of craving and seeking when these areas become mobilized with the objective of obtaining the drug of choice (Citation22). Increased activation of the ventral striatum in response to alcohol-related triggers is regarded as one of the main indicators of dysfunctional bottom-up processing among individuals with alcohol-use disorders (Citation7,Citation23).
Ex-smokers (Citation24) and smokers actively suppressing their craving responses (Citation11) have been shown to manifest top-down responses to smoking triggers, presumably reflecting an active process. In contrast, mindfulness-based intervention reduced the cue-induced craving in smokers in a “bottom-up” fashion, relying on a change in salience detection and decision making, due to training (Citation25). In research conducted with established AA members (Citation26), participants indicated that they employ AA prayers to cope emotionally with the experience of drinking triggers. However, it is not known which of these two mechanisms plays a more prominent role in long-term recovery. To explore this issue, we designed a functional magnetic resonance imaging (fMRI) study to assess the impact of AA prayer on neurophysiological and subjective craving in the presence of alcohol cues to determine whether prayer resulted in greater activation of brain areas associated with top-down or bottom-up emotional control and attention.
Methods
Participants
For this within-subject design pilot study, a sample of 20 AA members were recruited as in our previous studies, through our established ties with AA-member-networks. Inclusion criteria were as follows: 1 – current abstinence from alcohol and other illicit drugs, 2 – at least two years of uninterrupted, 3 – regular AA meeting attendance, and 4 – having had a spiritual awakening as described in AA tradition. Exclusion criteria were as follows: 1 – history of mental illness, 2 – current use of psychiatric medication, and 3 – standard MRI safety concerns. Information collected during the initial screening to determine eligibility also included the following: years in AA, frequency of attending meetings, years of alcohol abuse prior to entering the AA program, other types of spiritual practice and frequency, weight (for the purpose of MRI calibration), age, sex, ethnicity, and education. All participants had normal or corrected-to-normal vision and provided written informed consent. The present study was conducted in accordance with the safety guidelines for fMRI research, and approved by the Institutional Review Board of the New York University School of Medicine.
Procedure
Upon arriving for the scan, participants first completed a questionnaire designed to assess depth and nature of their spiritual experience and involvement in AA (Citation3). This was followed by a short practice time for participants to familiarize themselves with experimental procedures, in order to minimize any learning effects, and the actual scan. During scanning, participants were exposed to images of alcohol-craving-inducing stimuli and asked to rate their craving on a scale of 1 – not at all, to 5 – very much. Upon successfully completing the scan, participants were given a short questionnaire to assess their experience during scanning.
Measures
The instruments and measures administered included items assessing demographics, substance abuse history, addiction treatment, and experience in AA adapted from our previous research (Citation3). Craving for alcohol as experienced in the past week was assessed by responses on a 10-point visual analog scale. To assess the strength of members’ social affiliative ties, two scales applied in our previous studies of AA members were included in the questionnaire (Citation3,Citation27). One scale reflects the level of affiliation with 10 AA members known best to respondents, and the other measure reflects the strength of affiliative ties with 10 individuals known best to respondents who are not AA members. Respondents’ spiritual and religious orientation was assessed by items employed in surveys of US national probability samples (Citation28–Citation30).
Alcohol cue task
As in previous studies (Citation11), participants viewed still photos of alcohol-craving-inducing images. Images were selected from the Normative Appetitive Picture System (Citation31), and supplemented with alcohol-related pictures from the web. In total 90 images were used (30 per condition). Stimuli were presented via an LCD projector and custom optics onto a rear-projection screen in the bore of the MRI scanner. Participants were supine and viewed the projected stimuli through an angled mirror. An infrared, video eye-tracker (ASL R- LRO-6, Bedford, MA, or EyeLink 1000, SR Research, Mississauga, ON, Canada) was used to visually monitor whether fixation was maintained and if the eyes were kept open, but the eye-position measurements were not recorded. Stimuli were shown under three experimental conditions: (a) “prayer” – following the reading of AA prayers that are related to promoting abstinence, (b) “passive” – following reading of instruction to view stimuli passively, and (c) “news” – following reading of unrelated information. For the “prayer” condition, the subjects read the standard AA prayer from Step 3 and the Serenity prayer, adjusted for length (Citation32) (see SI). They were asked to keep in mind the intent of the prayer while viewing the images. For the “passive” viewing condition, subjects read the instruction to view stimuli passively and allow their reaction to be as it was, without attempting to suppress it. And, for the “news” condition they were asked to read and keep in mind the content of the news passage. A degree of self-reported craving was collected via a button box pressed in response to each stimulus, on a 5-point scale. Each condition was followed by a “washout” period during which participants saw a rapid series of single-digit numbers and were asked to press a key corresponding to the number displayed as quickly as they could.
fMRI protocol
The fMRI protocol with still images was designed using E-Prime 2.0 Professional (Psychology Software Tools), and consisted of the following: for each condition participants first saw a fixation cross of jittered duration ~4 s, followed by an instruction for the condition for 40 s, followed by 10 images (4 s each). After each image display, a fixation cross of jittered duration ~2.5 s was displayed, followed by a question asking participants to provide a rating of their craving for 3 s, and then again a fixation cross jittered ~3.5 s. After 10 images for one condition, there was a washout period of 20 s while participants pressed a corresponding key for each rapidly displayed number (see Figure S1 in Supplementary Information). Each condition repeated three times for the total of 90 images, and the order of conditions was pseudo-randomized.
fMRI data acquisition and preprocessing
MR images were acquired at the NYU Center for Brain Imaging, using a Siemens Allegra 3T head-only scanner equipped with a 8-channel head coil (Nova Medical, Wakefield, MA). Blood oxygenation level-dependent (BOLD) contrast was obtained using a T2-sensitive echo planar imaging (EPI) pulse sequence (TR = 2000 ms, TE = 30 ms, 36 axial slices, 3 × 3 × 3 mm, 64 × 64 matrix in a 192 × 192 mm FOV). In addition to functional images, a high-resolution, T1-weighted anatomical volume of images was acquired for each participant, using an MPRAGE sequence (TR = 2500 ms, TE = 3.93 ms, TI = 900 ms, flip angle = 8°, 176 sagittal slices, 1 × 1 × 1 mm, 256 × 256 matrix in a 256 mm FOV).
fMRI data were preprocessed using SPM8 (Wellcome Department of Cognitive Neurology; (Citation33), as scripted in NeuroElf 1.0 (http://neuroelf.net/, JW) in MATLAB (MathWorks, Natick, MA). Standard preprocessing steps were used to perform slice-time correction, 3D motion correction using rigid-body alignment, and spatial normalization to the ICBM standard template space by applying the Unified Segmentation process implemented in SPM8 to the high-resolution anatomical images and subsequently warping the functional images into template space using the parameters determined during the segmentation with an output resolution of 3 × 3 × 3 mm. Finally, data were spatially smoothed using a 6 mm Gaussian kernel (FWHM).
fMRI statistical analysis
For the images task, a first-level robust (iteratively re-weighted least squares), multiple linear regression was performed, in which each condition, i.e., separate instruction and image-viewing periods as well as rating periods, was modeled as a separate regressor, created by convolving a box-car function with the canonical HRF. Robust regression was used to automatically down-weigh (up to fully reject) outliers in the fMRI time-series on a voxel-by-voxel basis. In addition to the conditions themselves, motion parameters and low-frequency regressors were added as confounds to account for non-BOLD-related signal variability.
On the second (group) level, random-effects (RFX) robust regressions were computed for the main effect of the critical difference of prayer vs. other (passive and news) conditions, as well as for estimating the correlations between this difference and the self-report measures. To ensure that the main effect was specific for prayer over either of the other two conditions, an additional conjunction analysis with prayer vs. passive and prayer vs. news was conducted, which revealed that indeed prayer was different from each of the other conditions. Given that this was merely a confirmatory step, the findings from the combined contrast (prayer vs. other) are reported in the tables and figures.
The significance of clusters was assessed using a combined height (uncorrected statistical) and required cluster size threshold, where the cluster size was determined using the Alphasim procedure as implemented in NeuroElf. The method automatically uses the estimated smoothness of the residual of the appropriate regression, taking the inherent correlation in the data into account which could lead to false positive clusters. We chose an uncorrected threshold of (two-tailed) p < 0.02 (equaling a t-score of 2.56, df = 17), which given the estimated smoothness of 8.0 mm led to a cluster size estimate of k = 104 (3 × 3 × 3 mm) voxels required to reach an FWE-corrected threshold of p < 0.05. Unless otherwise noted, all areas mentioned as significantly activated/correlated survived the whole-brain correction procedure.
Additionally, a targeted, a-priori-informed region of interest (ROI) analysis of ventral striatum (the nucleus accumbens, tested for both left and right hemispheric regions, defined by applying a 6-mm sphere around the peak of the nucleus-accumbens term map from NeuroSynth, http://neurosynth.org/) was performed for the main effect of condition (prayer over other) and for the correlation of the parameter estimates with the average of self-report ratings. To further elucidate the contributions of the individual (contrast component) conditions, we also computed correlations between the estimated betas for the prayer condition with the in-scanner craving ratings during the prayer condition, and likewise for the other two conditions, as well as, between the non-AA affiliation scores and each of the conditions separately.
To reduce the influence of signal components unrelated to BOLD contrast changes, the following regressors of no interest (nuisance covariates) were added during first-level robust regressions: (Citation1) a discrete-cosine-transform (DCT) basis function set with a cutoff of 240 s to account for temporal drifts, (Citation2) the six rigid-motion parameters estimated during the realignment preprocessing step, and (Citation3) the first six principle components estimated from a combined white-matter-and-CSF mask following the CompCor procedure (Citation34). In short, following this procedure we first extracted the time courses from white-matter and CSF voxels which typically do not exhibit BOLD-related variability, and can therefore be used to estimate noise components. This was followed by applying a principle component analysis (PCA) to the matrix of extracted time courses to determine those regressors explaining the most overall variance in all nuisance voxels. Finally, these regressors were then added to the first-level design matrices, allowing to account for variance that is not related to BOLD signals across the brain.
Results
Sample characteristics
Data from 20 participants were collected. Data from two participants were excluded from the analysis, due to falling asleep or moving more than a voxel size of 3 mm while in the scanner.
Description of AA member sample
As shown in , most of the participants were middle-aged, male, and employed, with a history of both drug and alcohol use. Although 38.9% reported prior substance-use treatment, the majority (61.1%) had received treatment for general psychological problems. Participants’ first encounter with AA, on average, dates back as far as nearly two decades prior to study entry. All reported being currently abstinent from substances, with a mean duration of 14.4 (SD 11.9) years. Reflecting their commitment in terms of both fellowship and spirituality aspects of AA program participation, all participants had had a sponsor, and most served as a sponsor of other AA members, with one-half having sponsored more than five other members. All reported performing service for the fellowship (e.g., greeting meeting attendees, making coffee at meetings) and were frequent meeting attenders in the past year. The levels of AA member affiliation and acceptance of Twelve Step beliefs were similar to that obtained in our prior research on long-term AA members (Citation3,Citation27). Most (72.2%) of the participants reported that they felt God’s presence at least most days and prayed on a daily basis.
Table 1. Relationship of subject characteristics to self-reported craving in the prayer condition during fMRI scan (n = 18).
Behavioral analysis
A repeated-measures MANOVA was performed to determine whether the 18 participants varied in their self-report ratings of alcohol craving in the prayer, passive, and news conditions, There was an overall effect for type of condition (Wilks’ Lambda, F = 8.589, df = (Citation2, Citation16), p < 01). Post-hoc tests at the .01 level showed that participants’ ratings in the prayer condition (mean = 1.310, SD = .366) were significantly lower than their ratings in both the passive (mean = 1.945, SD = .783), and news (mean = 1.898, SD = .788) conditions.
Relationship of subject characteristics to self-reported craving during fMRI scan
A series of correlational tests were conducted to assess the relationship between demographic, substance use, AA program, and emotional-distress-related characteristics to self-reported craving in the prayer condition. Over one-third (38.9%) of the sample craved alcohol during the week prior to study entry. Prior craving in the previous week was positively correlated with craving ratings during the prayer condition (r = .681, p < .01). As shown in , the older the participant and the greater the duration of abstinence, the lower the level of craving during the prayer condition (r = −.520, p < .05 and r = −.506, p < .05, respectively). Involvement in AA as represented by the number of years since participants’ first spiritual awakening was more strongly associated with lower craving during the prayer condition than acceptance of Twelve Step beliefs (r = −.474, p < .05 and r = −.465, p < .06, respectively) with the latter indicating a trend. Neither affiliation to AA members nor affiliation to non-AA members was associated with craving in the prayer condition. A similar set of analyses were conducted with respect to the passive and news conditions as shown in . In contrast to the prayer condition, age was unrelated to level of craving in both the passive and news conditions. As found in the prayer condition, both duration of abstinence and the number of years since the subjects’ first spiritual awakening were associated with less craving in the passive (r = −.588, p < .01; r = −.474, p < .05, respectively) and news conditions (r = −.632, p < .05; r = −.627, p < .01, respectively).
fMRI results
Viewing appetitive images during the “prayer” condition, as compared to “other” conditions (average of “passive” and “news” conditions with equal weighting), increased the activity in the left-anterior middle frontal gyrus (BA 10), left superior parietal lobule and bilateral precuneus (BA 7), and bilateral posterior middle temporal gyrus (BA 39) ( and , and ). During reading of the instructions, prayer compared to other conditions resulted in the increase of signal in the areas of right intraparietal sulcus (BA 7) and the bilateral lingual gyrus (BA 18).
Table 2. Regions of interest (ROI) activations for prayer > other. All coordinates are in MNI space.
Figure 1. Brain areas activated for main contrast (prayer > passive + news). The left-anterior middle frontal gyrus (l-MFG; BA 10), left-superior parietal lobule (l-SPL; BA 7), bilateral precuneus (BA 7), and bilateral posterior middle temporal gyrus (MTG, BA 39). Two-tail t-test (df 17) = 2.56, FWE alphasim p < 0.05 corrected, k = 104. The brain is displayed in neurological convention (right = right).
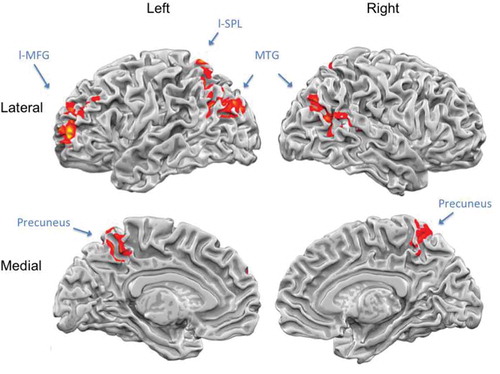
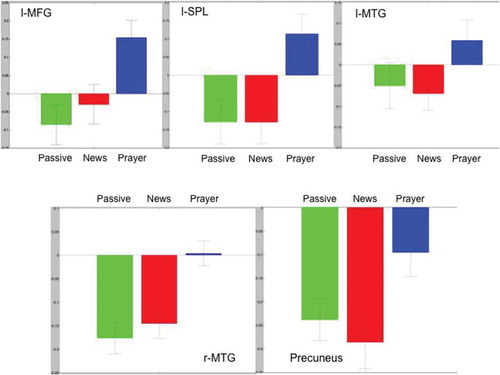
Figure 2. General linear model (GLM) beta plots for the main contrast regions of interest (ROIs). See for details. Green – Passive; Red – News; Blue – Prayer. x-axis: conditions, y-axis: percent BOLD signal change. The left-anterior middle frontal gyrus (l-MFG; BA 10), left-superior parietal lobule (l-SPL; BA 7), left- and right-posterior middle temporal gyrus (l/r-MTG, BA 39), and bilateral precuneus (BA 7).
There was no significant difference in activation in the ventral striatum in any of the three conditions tested, applying the whole-brain analysis thresholds (for further details, see Figure S2 and Table S1 in Supplementary Information). Subsequent, targeted, a-priori-informed ROI analysis of the ventral striatum (the nucleus accumbens, tested for both left and right hemispheric regions) confirmed this and revealed neither a main effect of condition (prayer over other) nor a correlation of the parameter estimates with the average rating (all p’s > 0.05). A re-analysis of data, using principal component analysis (PCA) methods to reject nuisance covariates, also did not reveal a significant change in the activation of the ventral striatum either for the main contrast of interest, prayer > other, or for any of the three conditions compared to the baseline. However, it did reveal new areas of increased activation in the prayer condition compared to the non-prayer states: left caudate nucleus, right insula (BA 13), the right-inferior prefrontal gyrus (BA 47), and the right supramarginal gyrus (BA 40) (two-tailed t(Citation17) = 6.06, p < 0.05 FWE, k = 59), (see Table S2 in Supplementary Information).
For illustration purposes, the following are results comparing each of the three experimental conditions to baseline (see Figure S2 and Table S1 in Supplementary Information). During passive viewing of alcohol-related cues, as compared to baseline (FWE alphasim p < 0.05 corrected, k = 213), increased activation was observed in bilateral occipital lobe (BA 17, 18, 19), accompanied by deactivation in the bilateral precuneus and posterior cingulate gyrus (BA 7, 31), bilateral medial prefrontal gyrus and anterior cingulate sulcus (BA 32, 24), and the right-posterior superior temporal gyrus (BA 22, 39). The News condition as compared to baseline (FWE alphasim p < 0.05 corrected, k = 240) resulted in activation in the bilateral occipital lobe (BA 17,18,19) and deactivation in bilateral precuneus/posterior cingulate gyrus (BA 7, 31). The Prayer condition as compared to baseline (FWE alphasim p < 0.05 corrected, k = 318) resulted in activation in the bilateral occipital lobes (BA 17,18,19), left pre-central and inferior prefrontal gyri including insula (BA 6,44,13), and left pre-central gyrus/frontal eye-field (BA 6,8).
Relationship of fMRI signal change and self-reported measures
Difference in activation for prayer vs. other (news plus passive) was inversely correlated with self-reported ratings of alcohol craving in the prayer condition (compared to the averaged rating for passive plus news conditions) in the bilateral posterior cingulate gyrus (BA 23), bilateral supramarginal gyrus (BA39), the right-anterior middle prefrontal gyrus (BA 10), and the right medial frontal gyrus (BA 9) (for table see Supplementary Information). Likewise, affiliation to non-AA members was inversely correlated with the difference in activation during prayer condition compared to other in bilateral precuneus (BA 7), bilateral posterior cingulate cortex (BA 31) and left-posterior superior temporal sulcus (BA 39) (see Table 3S in Supplementary Information). None of the individual component correlations (e.g., of the first-level prayer beta maps with the in-scanner craving ratings during the prayer condition) yielded significant results (at whole-brain corrected levels).
Discussion
In order to better understand the neural mechanisms underlying diminished alcohol craving among long-term sober AA members, we used an fMRI paradigm that compared behavioral and neuronal-activity-dependent responses to alcohol-related cues following AA prayer, during passive viewing, and following the reading of irrelevant news. While interpreting the meaning of fMRI activations is limited by the issue of reverse inference, we interpret our findings as follows:
Our finding was that for AA members with long-term abstinence, praying to regulate the subjectively perceived experience of craving in presence of alcohol-related cues increased activation in the following areas of the cortex: 1 – prefrontal and parietal areas related to endogenous attention, goal maintenance, and voluntary control of emotions (Citation21,Citation35,Citation36); 2 – posterior temporal areas related to semantic reappraisal of emotion (Citation37), and 3 – medial parietal areas related to visuo-spatial processing and self-related cognition (Citation38,Citation39). In contrast, reading of the instructions, prayer compared to passive and news resulted only in the increase of activation in the attention-related area of the right intra-parietal sulcus, and the primary visual area of the lingual gyrus, possibly indicating heightened perception due to attentional feedback.
Due to complexity of neuronal activity contributing to BOLD signal, our analysis (GLM) does not allow us to make definitive interpretations about absence of activation in specific areas of the brain (Citation40). We therefore re-analyzed the data using PCA (see the section “Methods” to this paper), and, as previously, did not find any activations or deactivations in the ventral striatum, either for the main contrast or when comparing each condition to baseline. However, we did find additional areas of activation for the main contrast (prayer > other) in the right lateralized areas of insula, the inferior prefrontal cortex and the temporoparietal junction – areas known to be involved in bottom-up control, empathizing and theory of mind (Citation18,Citation19,Citation38) – as well as, in an area of the left caudate nucleus. The caudate area of the dorsal striatum is involved in motor functions and in learning outcomes that support complex goal-directed actions (Citation41). In addition, it is involved both in acquiring addictive habits and in controlling them (Citation42).
While comparing a condition to baseline in fMRI experiments does not yield definitive results due to violation of pure insertion, we have included them for the purpose of illustration (Citation43). Passive viewing of alcohol-related images/cues, compared to the baseline, elicited neural responses characteristic of visual stimulus processing, with increased activation in the areas of occipital and lateral parietal lobes, accompanied by characteristic decreases in the areas involved in self-referential cognition: medial prefrontal cortex, precuneus, posterior cingulate gyrus, and the right temporoparietal junction. The news condition compared to baseline elicited similar neural responses and was not significantly different from passive viewing. Viewing images in the prayer condition compared to the baseline had a different pattern of neural responses. In addition to an expected increase of activity in the occipital areas for visual processing, activity increases were observed bi-laterally in the inferior prefrontal gyrus, involved in the language processing (left) and response inhibition (right); in the bilateral insula involved in interoception; in the left dorsolateral prefrontal cortex involved in working memory and decision making; in the left pre-central gyrus and left frontal eye-field involved in motor and visual attention control; and in the left dorsal anterior cingulate gyrus involved in conflict monitoring and resolution.
Thus, AA prayer resulted in subsequent differential modulation of a number of areas in the brain involved in regulation of experience reflective of reliance on both top-down and bottom-up processing and semantic control. In particular, the activation in the rostral middle prefrontal gyrus has been found to increase with decreased craving (Citation11), and to be involved, together with precuneus, in cognitive control related to recovery (Citation44). Somewhat surprisingly, we did not find activations in only one of the control systems. Instead, we found a co-activation of the areas associated both with the endogenous voluntary attention, such as the frontal eye-fields and the dorso-lateral prefrontal cortex, and those associated with bottom-up control, such as the right insula and the right-inferior prefrontal gyrus. This finding arguably points to a more integrated functioning of top-down and bottom-up control systems during AA prayer condition. Such integrated functioning may provide a more optimal control, and bears similarity to what has been found with other spiritual practices (Citation45).
Relationship between main fMRI finding and self-report measures
An inverse correlation between the subjectively perceived difference in craving during prayer and the main fMRI contrast for prayer compared to other, in a number of areas of the default mode network usually associated with self-referential processing (see Table S3 in Supplementary Information), could be interpreted to indicate that for participants who experienced prayer to reduce their perceived craving, the self-related aspects of experience did not need to be suppressed as much. This may be indicative of a shift in subjects’ self-schema to being a person who is not tempted by alcohol cues (see below). An inverse correlation was also found between the affiliation to non-AA members and the difference in signal for the main contrast in the posterior areas of the default network: bilateral precuneus and posterior cingulate gyrus, and the left-posterior superior temporal sulcus, indicating that AA prayer had less effect in those brain areas for those members with stronger ties to non-AA members. Given the lack of significant findings for the correlations or behavioral scores with the individual condition beta maps, we were unable to elucidate the exact nature of the contribution to the observed (and reported) correlation with the Prayer > Other contrast. Replications and future extensions of this work should address this question.
Notably, self-reported craving was inversely related to variables that can be understood to reflect a greater involvement in AA itself across all study conditions. These were duration of abstinence and the number of years since first experiencing spiritual awakening. Long-term abstinence may entail acquisition of enhanced functional capacities as reflected in diminished alcohol cue responsivity.
The superordinate impact of long-term membership
The concept of schemas, originally posited by Piaget (Citation46), relates to how multiple stimuli and responses are integrated in establishing complex thought and behavior patterns. One manifestation of schema development may lie in the integration of the many issues and components that go into the way people (individuals with alcohol-use disorders, in this case) perceive themselves. Indeed, young-adult substance-abusers have been found to be characterized by maladaptive schemas (Citation47). Although the data collected in this study did not address self-schemas directly, the potential role of self-schema in relation to disposition of long-term individuals with alcohol-use disorders in AA toward diminished craving has been discussed previously (Citation6). The alteration in cue responsivity among long-term AA members, like our subjects, may reflect experiences that have led to transformation in their self-schemas, their perception of themselves.
This may be reflected in neural functions which have recently been studied regarding the following: members’ exposure to the interpersonal context of AA can be affected by their capacity to mentalize and relate to others empathically in AA encounters (Citation48), but these encounters can be transformative relative to the impact of their identification with in-group members (Citation49) and consequent integration of input from them into long-term memory (Citation50). Indeed, the malleability in a person’s relation to substances has long been considered (Citation51). The aforesaid processes can thereby be understood to yield changes in how an alcoholic sees himself from one who is a responder to drinking-cues to one who understands himself to be less responsive. Ultimately, this may modify an alcoholic’s reactivity to such cues.
Limitations
The following limitations relating to the nature of the sample and the research study design bear upon the interpretation and generalizability of our findings. Due to the small sample size, all correlational findings and their interpretations must be considered preliminary and will require independent replication or otherwise corroboration. Although small, our subject pool had a considerable diversity, which reflects the realistic makeup of AA membership. The characteristics in our current sample related to commitment to the program are similar to other AA member samples we have studied with stable abstinence, not only those with 10 or more years of abstinence. Therefore, our findings may be suggestive of the larger population of members with stable abstinence. Nevertheless, a larger subject sample would have allowed us to explore individual difference factors in more depth. An objection could be raised that our experimental design may not have been sensitive enough to detect changes in the ventral striatum in the presence of alcohol-related images. A more complex factorial design could have allowed us to explore potential causal mechanisms; however, adding more variables would have also reduced the power of the design. Measures of smoking behavior, which may have influence on findings, were not assessed. Finally, there was no control group and comparisons to AA members in early abstinence or in non-abstinence states constitute an important area for further investigation particularly as they relate to striatal response in the context of alcohol triggers. Significance and conclusions
The findings of this study help put the reports of long-term AA members regarding diminished alcohol craving in perspective. We were not able to study the neural correlates of long-term members’ reports of ongoing diminished craving with subjects in their naturalistic setting. We were, however, able to use the responses of a sample of convenience of such members to the ritual of AA praying as a proxy for this.
The merit of this approach is supported by reports from long-term members in both our clinical encounters and interviews that they often prayed to avoid craving and potential relapse when confronted with alcohol-related triggers. It is further supported by the positive relationship between subjects’ self-reported level of craving in the prayer state while in the scanner, and their self-reports of craving during the past week. We can therefore consider neural correlates of decreased craving following prayer as a potential proxy for craving management in naturalistic settings. Further investigation into neural mechanisms underlying such methods may be useful in improving the treatment outcomes for chronic individuals with alcohol-use disorders.
Declaration of interest
The authors declare no conflicting interests.
Supp._Information.docx
Download MS Word (2.1 MB)Acknowledgements
The authors express appreciation to Drs. Hedy Kober, John T. Cacioppo, and Stephen G. Post for consultation on this project.
Related Research Data
References
- AA World Services. A.A. fact file. New York, NY: AA World Services; 1956. Available at: http://www.aa.org/assets/en_US/m-24_aafactfile.pdf [last accessed 10 Jun 2014].
- Galanter M, Dermatis H, Post S, Santucci C. Abstinence from drugs of abuse in community-based members of Narcotics Anonymous. J Stud Alcohol Drugs 2013;74:349–352.
- Galanter M, Dermatis H, Santucci C. Young people in Alcoholics Anonymous: the role of spiritual orientation and AA member affiliation. J Addict Dis 2012;31:173–182.
- Galanter M, Dermatis H, Stanievich J, Santucci C. Physicians in long-term recovery who are members of Alcoholics Anonymous. Am J Addict 2013;22:323–328.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: American Psychiatric Publishing; 2013.
- Galanter M. Alcoholics Anonymous and twelve-step recovery: a model based on social and cognitive neuroscience. Am J Addict 2014;23:300–307.
- Schacht JP, Anton RF, Myrick, H. Functional neuroimaging studies of alcohol cue reactivity: a quantitative meta-analysis and systematic review. Addict Biol 2013;18:121–133.
- Koob GF, Volkow ND. Neurocircuitry of addiction. Neuropsychopharmacol Off Publ Am College Neuropsychopharmacol 2009;35:217–238.
- Witkiewitz K. Temptation to drink as a predictor of drinking outcomes following psychosocial treatment for alcohol dependence. Alcohol Clin Exp Res 2013;37:529–537.
- Seo D, Lacadie CM, Tuit K, Hong KI, Constable RT, Sinha R. Disrupted ventromedial prefrontal function, alcohol craving, and subsequent relapse risk. JAMA Psychiatry 2013;70:727–739.
- Kober H, Mende-Siedlecki P, Kross EF, Weber J, Mischel W, Hart CL, Ochsner KN. Prefrontal–striatal pathway underlies cognitive regulation of craving. Proc Natl Acad Sci 2010;107:14811–14816.
- Feldstein Ewing SW, Filbey FM, Sabbineni A, Chandler LD, Hutchison KE. How psychosocial alcohol interventions work: a preliminary look at what fMRI can tell us. Alcohol: Clin Exp Res 2011;35:643–651.
- National Opinion Research Center. General social survey 2010 cross-section and panel combined: frequency of prayer (Pie chart). The Association of Religion Data Archives; 2010. Available at: http://www.thearda.com/quickstats/qs_104.asp [last accessed 13 Jun 2014].
- Young LB. Characteristics and practices of sponsored members of Alcoholics Anonymous. J Groups Addict Recov 2013;8:149–164.
- Neubauer RL. Prayer as an interpersonal relationship: a neuroimaging study. Relig Brain Behav 2013;4:92–103.
- Kaskutas LA, Turk N, Bond J, Weisner C. The role of religion, spirituality and Alcoholics Anonymous in sustained sobriety. Alcohol Treat Quart 2003;21:1–16.
- Lambert NM, Fincham FD, Marks LD, Stillman TF. Invocations and intoxication: does prayer decrease alcohol consumption? Psychol Addict Behav 2010;24:209–219.
- Menon V, Uddin LQ. Saliency, switching, attention and control: a network model of insula function. Brain Struct Funct 2010;214:655–667.
- Corbetta M, Shulman GL. Control of goal-directed and stimulus-driven attention in the brain. Nat Rev Neurosci 2002;3:201–215.
- Spreng RN, Sepulcre J, Turner GR, Stevens WD, Schacter DL. Intrinsic architecture underlying the relations among the default, dorsal attention, and frontoparietal control networks of the human brain. J Cogn Neurosci 2012;25:74–86.
- Phillips ML, Ladouceur CD, Drevets WC. A neural model of voluntary and automatic emotion regulation: implications for understanding the pathophysiology and neurodevelopment of bipolar disorder. Mol Psychiatry 2008;13:833–857.
- Goldstein RZ, Volkow ND. Dysfunction of the prefrontal cortex in addiction: neuroimaging findings and clinical implications. Nat Rev Neurosci 2011;12:652–669.
- Volkow ND, Wang G-J, Fowler JS, Tomasi D. Addiction circuitry in the human brain. Annu Rev Pharmacol Toxicol 2012;52:321–336.
- Nestor L, McCabe E, Jones J, Clancy L, Garavan H. Differences in “bottom-up” and “top-down” neural activity in current and former cigarette smokers: evidence for neural substrates which may promote nicotine abstinence through increased cognitive control. NeuroImage 2011;56:2258–2275.
- Westbrook C, Creswell JD, Tabibnia G, Julson E, Kober H, Tindle HA. Mindful attention reduces neural and self-reported cue-induced craving in smokers. Soc Cogn Affect Neurosci 2013;8:73–84.
- Galanter M, Dermatis H, Sampson C. Spiritual awakening in Alcoholics Anonymous: empirical findings. Alcohol Treat Quart 2014;32:319–334.
- Galanter M, Talbott D, Gallegos K, Rubenstone E. Combined Alcoholics Anonymous and professional care for addicted physicians. Am J Psychiatry 1990;147:64–68.
- Davis JA, Smith TW, Marsden PV. General social surveys, 1972–2008: cumulative codebook. Principal Investigator, Davis JA; Director and Co-Principal Investigator, Smith TW. Chicago, IL: National Opinion Research Center, 2009 ( National Data Program for the Social Sciences Series, no. 18).
- Beliefnet.com (Internet). Newsweek/Beliefnet Poll Results; 2005. Available at: http://www.beliefnet.com/News/2005/08/Newsweekbeliefnet-Poll Results.aspx [last accessed 6 Jun 2011].
- Kosmin B, Keysar A. American religious identification survey (ARIS 2008). Hartford, CT: Trinity College; 2009.
- Stritzke WG, Breiner MJ, Curtin JJ, Lang AR. Assessment of substance cue reactivity: advances in reliability, specificity, and validity. Psychol Addict Behav 2004;18:148–159.
- Alcoholics Anonymous. Twelve steps and twelve traditions. New York, NY: A.A. World Services; 1953.
- Friston KJ, Ashburner J, Kiebel SJ, Nichols TE, Penny WD, editors. Statistical parametric mapping: the analysis of functional brain images. New York, NY: Academic Press; 2007.
- Behzadi Y, Restom K, Liau J, Liu TT. A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. Neuroimage 2007;37:90–101. doi:10.1016/j.neuroimage.2007.04.042
- Ochsner KN, Gross JJ. Cognitive emotion regulation: insights from social cognitive and affective neuroscience. Curr Direct Psychol Sci 2008;17:153–158.
- Vincent JL, Kahn I, Snyder AZ, Raichle ME, Buckner RL. Evidence for a frontoparietal control system revealed by intrinsic functional connectivity. J Neurophysiol 2008;100:3328–3342.
- Buhle J, Silvers J, Wager TD, Lopez R, Onyemekwu C, Kober H, Weber J, et al. Cognitive reappraisal of emotion: a meta-analysis of human neuroimaging studies. Cereb Cort 2014;24:2981–2990.
- Andrews-Hanna JR, Reidler JS, Sepulcre J, Poulin R, Buckner RL. Functional-anatomic fractionation of the brain’s default network. Neuron 2010;65:550–562.
- Margulies DS, Vincent JL, Kelly C, Lohmann G, Uddin LQ, Biswal BB, Virlinger A, et al. Precuneus shares intrinsic functional architecture in humans and monkeys. Proc Natl Acad Sci 2009;106:20069–20074.
- Xu J, Calhoun VD, Potenza MN. The absence of task-related increases in BOLD signal does not equate to absence of task-related brain activation. J Neurosci Methods 2014;240:125–127.
- Grahn JA, Parkinson JA, Owen AM. The cognitive functions of the caudate nucleus. Prog Neurobiol 2008;86:141–155.
- Kalivas PW. Addiction as a pathology in prefrontal cortical regulation of corticostriatal habit circuitry. Neurotoxic Res 2008;14:185–189.
- Poldrack RA. Can cognitive processes be inferred from neuroimaging data? Trends Cogn Sci 2006;10:59–63.
- Konova AB, Moeller SJ, Goldstein RZ. Common and distinct neural targets of treatment: changing brain function in substance addiction. Neurosci Biobehav Rev 2013;37:2806–2817.
- Vago DR, Silbersweig DA. Self-awareness, self-regulation, and self-transcendence (S-ART): a framework for understanding the neurobiological mechanisms of mindfulness. Front Hum Neurosci 2012;6:296.
- Piaget J, Kegan P. The child’s conception of the world. London: Routledge; 1929.
- Shorey RC, Stuart GL, Anderson S. Differences in early maladaptive schemas between a sample of young adult female substance abusers and a non-clinical comparison group. Clin Psychol Psychother 2014;21:21–28.
- Lombardo MV, Chakrabarti B, Bullmore ET, Wheelwright SJ, Sadek SA, Suckling J, MRC AIMS Consortium, et al. Shared neural circuits for mentalizing about the self and others. J Cogn Neurosci 2009;22:1623–1635.
- Morrison S, Decety J, Molenberghs P. The neuroscience of group membership. Neuropsychologia 2012;50:2114–2120.
- Spreng RN, Mar RA. I remember you: a role for memory in social cognition and the functional neuroanatomy of their interaction. Brain Res 2012;1428:43–50.
- Zinberg NE. Drug, set, and setting: the basis for controlled intoxicant use. New Haven, CT: Yale University Press; 1984.