
Abstract
This study reports the development and evaluation of Carbamazepine (CMP)-loaded microemulsions (CMPME) for intranasal delivery in the treatment of epilepsy. The CMPME was prepared by the spontaneous emulsification method and characterized for physicochemical parameters. All formulations were radiolabeled with 99mTc (technetium) and biodistribution of CMP in the brain was investigated using Swiss albino rats. Brain scintigraphy imaging in rats was also performed to determine the uptake of the CMP into the brain. CMPME were found crystal clear and stable with average globule size of 34.11 ± 1.41 nm. 99mTc-labeled CMP solution (CMPS)/CMPME/CMP mucoadhesive microemulsion (CMPMME) were found to be stable and suitable for in vivo studies. Brain/blood ratio at all sampling points up to 8 h following intranasal administration of CMPMME compared to intravenous CMPME was found to be 2- to 3-fold higher signifying larger extent of distribution of the CMP in brain. Drug targeting efficiency and direct drug transport were found to be highest for CMPMME post-intranasal administration compared to intravenous CMP. Rat brain scintigraphy also demonstrated higher intranasal uptake of the CMP into the brain. This investigation demonstrates a prompt and larger extent of transport of CMP into the brain through intranasal CMPMME, which may prove beneficial for treatment of epilepsy.
Introduction
Carbamazepine (CMP) is used for the treatment of epilepsy and several psychiatric diseases. It is traditionally given by oral administration but due to its poor water solubility (about 170 mg/L at 24 °C). It is characterized by slow and irregular gastrointestinal absorption. Reportedly, it has an oral bioavailability of less than 50% (Barakat et al., Citation2006).
Oral route of drug administration is most convenient and well accepted. However in many instances, oral administration is unsuitable when drug undergoes significant degradation in the gastrointestinal tract or is metabolized to a high degree via the first-pass effect in liver. Also patients who are unable to swallow cannot be medicated by oral route which limits its utility in this particular population of patients. Hence, an alternative route of administration should be preferable. Reportedly, nasal mucosal membrane offers a practical non-invasive route of administration for therapeutic effect of many drugs (Li et al., Citation2002; Vyas et al., Citation2006; Jogani et al., Citation2008; Kaur & Kim Citation2008; Elshafeey et al., Citation2009; Patel et al., 2013a, b, c, d). Nasal route has advantages of rapid absorption of drug, higher bioavailability allowing lower doses, fast onset of therapeutic action, avoidance of liver or gastrointestinal metabolism, avoidance of irritation of the gastrointestinal membrane, reduced risk of overdose, non-invasive administration, ease of convenience and self-medication, and improved patient compliance (Li et al., Citation2002; Vyas et al., Citation2006; Jogani et al., Citation2008; Kaur & Kim Citation2008; Elshafeey et al., Citation2009; Patel et al., 2013b). Researcher are making many attempts to find efficient and new way to prevent extensive first-pass metabolism and target the drug to the receptor site in brain for treating brain disorders.
However, the limitation for intranasal drug delivery is the fact that most drugs diffuse poorly and slowly through the nasal mucosa and thus the desired levels of the therapeutic agent cannot be achieved. Also the nasal cavity accommodate limited volume of formulation, approximately 150 µL per nostril and excess volume will drain out into the pharynx and be swallowed (Shinde et al., Citation2011; Patel et al., 2013a, b).
The present study solves above mention problem and explored the suitable drug delivery vehicle, microemulsion (ME) which is able to dissolve the CMP, in required concentration, yet which is not irritating to the nasal mucosa. The intranasal administration of drug can be increased by co-administering a permeation enhancer (Patel et al., 2013b). ME have been thoroughly studied as a drug carrier due to their special features, such as ease of preparation due to spontaneous formation, thermodynamic stability, high solublization capacity for the hydrophilic and lipophilic drugs, transparent and elegant appearance, enhanced penetration through the biological membranes, increased bioavailability, and less inter- and intra-individual variability in drug pharmacokinetics (Li et al., Citation2002; Zhang et al., Citation2004; Kaur & Kim, Citation2008; Elshafeey et al., Citation2009; Shinde et al., Citation2011).
An additional constraint concerning nasal administration is the natural defence mechanism; nasal mucociliary clearance. Therefore, it is essential to localize the formulation on a mucosal layer of nasal cavity to enhance drug absorption and prevent rapid nasal clearance. Addition of a well-designed mucoadhesive agent to ME can prevent rapid nasal clearance of formulation (Patel et al., 2013b).
This article describes development, characterization and preliminary brain-targeting study of CMZ-loaded MME designed using Generally Regarded As Safe (GRAS) listed ingredients and polycarpophil AA-1 as a mucoadhesive component.
Materials and methods
Drug and reagents
CMP pure powder was obtained as gratis sample from Max Pharma (India) with 99.9% purity. Oleoyl polyoxylglycerides and Diethylene glycol monoethyl ether (Gattefosse Saint-Priest, France) were procured as gratis samples from Gattefosse Asia Ltd. (Mumbai, India). Polyoxyl 40 hydrogenated castor oil was procured as gratis sample form BASF (Mumbai, India). Polycarbophil (AA-1, pharmagrade, molecular weight approximately 3.5 million) was procured as gratis sample from Lubrizol Advanced Material India Pvt. Ltd. (Mumbai, India). Potassium dihydrogen phosphate, methanol and propylene glycol were purchased from SDfine Chemicals (Ahmedabad, India). Ethanol was purchased from Baroda Chemical Ind. Ltd (Dabhoi, India). Double distilled water was used throughout the study. All other chemicals and solvents were of analytical reagent grade and used as received without further purification.
Preparation and characterization of formulations
The ME for CMP was prepared by the spontaneous emulsification method (Patel et al., 2013a). The calculated amount of CMP (5 mg/mL) was added to the oily phase (Oleoyl polyoxylglycerides) of ME and magnetically stirred until dissolved followed by addition of emulsifier mixture (Emix) [Polyoxyl 40 hydrogenated castor oil (Nonionic emulsifiers) to Diethylene glycol monoethyl ether (Coemulsifier)] in a fixed proportion (4:1) to produce clear mixture. Then a defined proportion of water was added to produce crystal clear ME of CMP (CMPME). The mucoadhesive ME of CMP (CMPMME) was prepared by initially preparing ME of the drug using minimum volume of external phase and then adding the required volume of polymer solution (1%, wt/vol) so that the final concentration of polymer in the MME was 0.5% (wt/wt). After the addition of polymer solution, the MME was allowed to homogenize for 10 min. The CMP solution (CMPS) meant for comparative evaluation of MME-based systems was prepared by dissolving CMP (50 mg) in 10 mL of propylene glycol resulting in a solution of 5 mg/mL (Patel et al., 2013a, d).
CMP content in the formulations was assayed using a high-performance thin layer chromatography (Patel et al., Citation2010). The average droplet size and polydispersity index (PDI) of ME was determined using photon correlation spectroscopy (PCS) with in-built Zetasizer (Nano ZS, Malvern Instruments, UK) at 633 nm. Helium – neon gas laser having intensity of 4 mW was the light source. The droplet size was calculated using Stokes–Einstein relationship by Zetasizer Software. Electrophoretic mobility (µm/s) was measured using small volume disposable zeta cell and converted to zeta potential by in-built software using Helmholtz–Smoluchowski equation (Vyas et al., Citation2006; Patel et al., 2013a, d). The pH value of ME was determined using digital pH meter (HI 98107, Hanna Instruments, India), standardized using pH 4 and 7 buffers before use (Patel et al., 2013a). The viscosity of ME was measured using a Brookfield Viscometer LVDV – IIIU (Brookfield Engineering LABS, Stoughton, MA) with spindle SC 18 at 100 rpm using interval of 30 s. All aspects of testing were controlled using Rheocalc Software (Patel et al., 2013a, d).
Stability studies
The formulations, CMPME and CMPMME, were subjected to stability studies for a period of 6 months at room temperature and refrigerated conditions (4 °C). After 6 months of storage, the formulations were characterized for physical stability (creaming, phase separation, or flocculation), accelerated centrifugation cycle (3000 × g for 15 min), CMP content, particle size, and zeta potential determinations (Patel et al., 2013a, d).
Preliminary brain-targeting study
Preparation of radiolabeled formulations
CMP in CMPS and the formulations, CMPME and CMPMME, were radio-labeled using technetium – 99 (99mTc) by direct labeling method (Eckelman, Citation1995; Babbar et al., Citation2000; Li et al., Citation2002; Zhang et al., Citation2004; Vyas et al., Citation2006; Kaur & Kim, Citation2008; Patel et al., 2013b). To 1.0 mL of CMP formulation 200 µL of stannous chloride dehydrate (2 mg/mL in 10% acetic acid) was added, the pH was adjusted to 6.0–6.5 using 50 mM sodium bicarbonate solution. To the resultant mixture (filtered through 0.22µ nylon 66 membrane), required volume of sterile 99mTc-pertechnetate (5 mCi) was added over a period of 60 s with continuous mixing such that the resultant solution had a radioactivity of 5 mCi/mL and was incubated at 30 °C ± 5 °C for 30 min with continuous nitrogen purging. The final volume was made up to 2.5 mL using 0.9% (w/v) sterile sodium chloride solution. The resultant formulations obtained had 100 µCi/20 µL activity.
The radiochemical purity (Eckelman, Citation1995; Babbar et al., Citation2000; Patel et al., 2013b) of 99mTc-labeled CMPS (99mTc-CMPS), 99mTc-labeled CMPME (99mTc- CMPME) and 99mTc-labeled CMPMME (99mTc-CMPMME) was determined by ascending instant thin layer chromatography (TLC) using silica gel-coated fiberglass sheets and acetone as the mobile phase. The effects of incubation time, pH, and stannous chloride concentration on radiolabeling efficiency were studied to achieve optimum conditions. The radiolabeled formulations were challenged to assess bonding strength at different molar concentrations (25–100 mM) of diethylene triamine penta acetic acid (Eckelman, Citation1995; Babbar et al., Citation2000; Patel et al., 2013b). The optimized radiolabeled-CMP formulations were evaluated for in vitro stability in 0.90% (w/v) sodium chloride (normal saline) and in plasma (Eckelman, Citation1995; Babbar et al., Citation2000; Patel et al., 2013b). The optimized, stable radiolabeled CMP formulations were used for biodistribution study in rats.
Bio-distribution studies
The protocol for animal experimentation was approved by the Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA) and the Institutional Animal Ethics Committee (IAEC) of Veterinary Nuclear Medicine Centre, Bombay Veterinary College, Mumbai.
Wistar rats (male, aged 4–5 months), weighing between 200 and 250 g were selected for the study. Four rats for each formulation per time point were used in the study. The radiolabeled complex of 99mTc-CMPME (100 µCi/20 µL) containing 0.035–0.040 mg CMP (equivalent to 0.18–0.20 mg/kg body weight (B.W.)) was injected through tail vein of Wistar rats. Similarly, radiolabeled complex of 99mTc-CMPS/CMPME/CMPMME (100 µCi/20 µL) containing 0.035–0.040 mg CMP (equivalent to 0.18–0.20 mg/kg B.W.) was administered (10 µL) in each nostril. Prior to nasal administration of the formulations, the rats were anaesthetized using 50 mg/kg ketamine intramuscular injection and the formulations were instilled into the nostrils with the help of micropipette (10–100 µL) attached with low density polyethylene tube having 0.1 mm internal diameter at the delivery site. The rats were held from the back in slanted position during nasal administration of the formulations. The rats were sacrificed at predetermined time intervals and blood was collected using cardiac puncture. Subsequently, different tissues/organs including brain and spinal cord were dissected, washed twice using normal saline solution, and made free from adhering tissue/fluid and weighed. The radioactivity present in each tissue/organ was measured using shielded well-type gamma scintillation counter. The radiopharmaceutical uptake per gram in each tissue/organ was calculated as a fraction of administered dose by the following equation (Li et al., Citation2002; Zhang et al., Citation2004; Vyas et al., Citation2006; Jogani et al., Citation2008; Kaur & Kim, Citation2008).
To evaluate the brain-targeting efficiency, two indexes drug targeting efficiency (DTE, %) and nose-to-brain direct transport percentage (DTP, %) were adopted as mentioned below. DTE (%): DTE (%) represents time average partitioning ratio, which has been derived from Equation (Equation1(1) ). In order to define nose–brain direct transport clearly, ‘‘the brain drug DTP (%)’’; which has been derived from Equations (Equation2
(2) ) and (Equation3
(3) ).
(1)
(2)
where,
(3)
Where, AUC – Area under the curve; Bx – Brain AUC fraction contributed by systemic circulation through the BBB following intranasal administration; Bi.v – AUC0 → 480 (brain) following intravenous administration; Pi.v. – AUC0 → 480 (blood) following intravenous administration; Bi.n. – AUC0 → 480 (brain) following intranasal administration; Pi.n. – AUC0 → 480 (blood) following intranasal administration.
Reports in the literature reveal that the drug uptake into the brain from the nasal mucosa mainly occurs via three different pathways (Vyas et al., Citation2006; Jogani et al., Citation2008). One is the systemic pathway by which some of the drug is absorbed into the systemic circulation and subsequently reaches the brain by crossing BBB. The others are the olfactory pathway and the trigeminal neural pathway by which partly the drug travels directly from the nasal cavity to CSF and brain tissue. We can conclude that the amount of drug reaches in the brain tissue after nasal administration is attributed to these three pathways. Thus, we can assume that the brain AUC fraction contributed by systemic circulation through BBB (represented by Bx), divided by plasma AUC from nasal route is equal to that of IV route (see Equation (Equation1(1) )). Therefore, DTP (%) represents the percentage of CMP directly transported to the brain via the olfactory pathway and the trigeminal neural pathway. DTP (%) and DTE (%) were calculated using tissue/organ distribution data following intranasal and intravenous administrations.
Gamma scintigraphy imaging
The protocol for animal experimentation was approved by the Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA) and the Institutional Animal Ethics Committee (IAEC). Wistar rats (male, aged 4–5 months), weighing between 200 and 250 g were selected for the study. The radiolabeled complex of 99mTc-CMPS (100 mCi/100 µL) containing 0.035–0.040 mg CMP (equivalent to 0.18–0.20 mg/kg BW was IV injected. Similarly, the radiolabeled complex of 99mTc-CMPS/99mTc-CMPME/99mTc-CMPMME (100 mCi/100 µL) containing 0.035–0.040 mg CMP (equivalent to 0.18–0.20 mg/kg BW) was administered IN (50 µL in each nostril). The rats were held from the back in slanted position during nasal administration of formulations. The rats were anesthetized using 1 mL ketamine hydrochloride intramuscular injection (50 mg/mL) and placed on the imaging platform. Imaging was performed using Single Photon Emission Computerized Tomography (SPECT, LC 75-005, Diacam, Siemens AG; Erlanger, Germany) gamma camera (Vyas et al., Citation2006; Jogani et al., Citation2008; Patel et al., 2013b).
Statistical analysis
All data are reported as mean ± SEM and the difference between the groups were tested using Student’s t test at the level of p < 0.05. More than two groups were compared using ANOVA, with p < 0.05 considered statistically significant.
Results and discussion
Formulation development and characterization
ME formulations containing oleoyl polyoxylglycerides as an oil phase, were prepared at polyoxyl 40 hydrogenated castor oil and diethylene glycol monoethyl ether fixed Emix ratios of 4:1 (). The ME containing 6% wt/wt Oleoyl polyoxylglycerides, 32% wt/wt Emix and 62% wt/wt distilled water showed highest solubilizing capacity for CMP. Polycarbophil (0.5 %wt/wt) was used as a mucoadhesive polymer and incorporated in ME formulation to obtained CMP-loaded MME. All formulations were prepared and characterized for the various physicochemical parameters (). The CMP content (%) of CMPS, CMPME, and CMPMME was found to be 99.46 ± 1.38, 99.88 ± 1.25 and 100.14 ± 1.03, respectively, of the theoretical value (5 mg/mL). The narrow globule size range of 34.11 ± 1.41 nm and 40.57 ± 1.26 nm and PDI of 0.127 ± 0.012 and 0.134 ± 0.023 for CMPME and CMPMME, respectively, indicated that the ME approached a monodispersed stable system and could deliver the CMP effectively owing to larger surface area. The presence of zeta potential to the tune of −36.29 ± 3.03 and −48.58 ± 4.46 mV on the globules of CMPME, and CMPMME, respectively, conferred physical stability to the system. CMPME showed net negative charge and addition of mucoadhesive agent further contributed negativity to the system. This may be attributed to the fact that the increase in surfactant level resulted in a decrease in surface tension and surface free energy of the formed micelles. Therefore, net negative charge (anionic) of the ME increased (Li et al., Citation2002; Zhang et al., Citation2004; Vyas et al., Citation2006; Jogani et al., Citation2008; Kaur & Kim, Citation2008; Elshafeey et al., Citation2009; Shinde et al., Citation2011; Patel et al., 2013a, b). The MEs were expected to have good physical stability (phase separation) as zeta potential is less than −30 to −40 mV (Vyas et al., Citation2006; Jogani et al., Citation2008; Patel et al., 2013b). Moreover, addition of mucoadhesive polymer (polycarbophil) may further stabilize the system since it increased negative charge of the system (Vyas et al., Citation2006; Jogani et al., Citation2008; Patel et al., 2013b). A percentage transmittance of 99.97% for CMPME indicated clear dispersion, whereas CMPMME was hazy due to the presence of mucoadhesive component in the formulation. The samples were examined in a cross polarizer for sample homogeneity and birefringence. The CMPME appeared completely dark when observed under cross polarizer which confirmed its optically isotropic nature. The pH of all the CMPS, CMPME, and CMPMME ranged 5.17 to 5.54, approximating the normal pH range of nasal fluids, which is one of the formulation considerations that may help reducing the irritation produced upon instillation. It was observed that the viscosity of the ME formulations generally was very low. This was expected, because one of the characteristics of ME formulations is of lower viscosity. Low viscosity values of CMPME (186 ± 4.63 cp) and CMPMME (201 ± 6.82 cp), ensure easy handling, packing, and hassle-free nasal administration of formulations.
Table 1. Composition of carbamazepine microemulsion (CMPME) and carbamazepine mucoadhesive microemulsion (CMPMME).
Table 2. Characterization parameters of optimized carbamazepine microemulsions (CMPME) and carbamazepine mucoadhesive microemulsions (CMPMME) (n = 3).
In stability studies, the ME exhibited no precipitation of CMP, creaming, phase separation, and flocculation on visual observation and was found to be stable after centrifugation (3000 × g for 15 min) both at room temperature and at 2–8 °C. The results of stability studies showed that there are negligible changes in the parameters such as CMP content, % transmittance, globule size and zeta potential of CMPME and CMPMME after 6 months of storage at room temperature and refrigerated condition, thus substantiating the stability of formulations for 6 months (data not shown).
Preliminary brain-targeting study
CMPS, CMPME, and CMPMME formulations were effectively radiolabeled with Technetium-99 m (99mTc), optimized for maximum labeling efficiency and stability. Radiochemical purity achieved was 97.23%, 98.19%, and 98.46% for CMPS, CMPME, and CMPMME, respectively, when evaluated for reduced/hydrolyzed (R/H) 99mTc and free 99mTc. The optimal SnCl2.2H2O concentration was found to be 200 µL (2 mg/mL) at pH 6.0–7.0 with an incubation time of 30 min. 99mTc-CMPS/CMPME/CMPMME were found to be stable in normal saline solution and plasma up to 24 h (degradation <5% w/w). Bonding strength of 99mTc-CMPS/CMPME/CMPMME was also investigated by the DTPA challenging test, and the percent trans-chelation of the labeled complex was 1.73% w/w at 25 mM DTPA concentration, while at 100 mM, it increased to 3.59% w/w. The results suggested high bonding strength and stability of 99mTc-CMPS/CMPME/CMPMME. Thus, these formulations were found suitable for biodistribution studies of the CMP in rats.
Table 3. Compartmental distribution of 99mTc-CMPME (IV), 99mTc-CMPME (IN), 99mTc-CMPMME (IN), and 99mTc-CMPS (IN) at different time intervals in normal Wistar ratsa.
Table 4. Pharmacokinetics of 99mTc-CMPME (IV), 99mTc-CMPME (IN), 99mTc-CMPMME (IN), and 99mTc-CMPS (IN) at different time intervals in normal Wistar ratsa.
Biodistribution studies (Chow et al., Citation1999; Vyas et al., Citation2006; Jogani et al., Citation2008; Patel et al., 2013b) of 99mTc-CMP formulations following IV administration (CMPME) and intranasal (CMPS, CMPME, and CMPMME) administration on Wistar rats were performed and the radioactivity was estimated at predetermined time intervals up to 8 h. The brain/blood ratio of the CMP at all time points for different formulations were also calculated and recorded in . The pharmacokinetic parameters were calculated from and recorded in .
Figure 1. (A) CMP concentration in rat blood at different time intervals following 99mTc-CMPME (IV), 99mTc-CMPME (IN), 99mTc-CMPMME (IN), and 99mTc-CMPS (IN) administrations. (B) CMP concentration in rat brain at different time intervals following 99mTc-CMPME (IV), 99mTc-CMPME (IN), 99mTc-CMPMME (IN), and 99mTc-CMPS (IN) administrations.
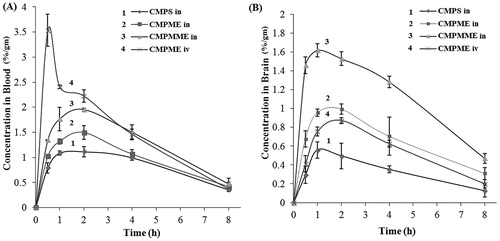
Table 5. Brain-targeting efficiency and direct nose-to-brain transport following intranasal administration of 99mTc-CMPME, 99mTc-CMPMME, and 99mTc-CMPSa.
CMP concentrations in brain following intranasal administrations of CMPME and CMPMME were found to be significantly higher at all sampling time points compared with IV administration of CMPME. The brain/blood ratio at 0.5 hour for CMPME (IN) and CMPMME (IN) was found to be 2- to 3- fold higher as compared with CMPME (IV). This finding may be attributed to direct nose-to-brain transport. Reports in the literature revealed that following intranasal administration, preferential nose-to-brain transport bypassing the BBB occurred due to the unique connection between the nose and the CNS (Vyas et al., Citation2006; Jogani et al., Citation2008; Patel et al., 2013b). The substantially higher uptake in the brain with intranasal administration suggests a larger extent of selective transport of CMP from nose-to-brain. Many researchers (Vyas et al., Citation2006; Jogani et al., Citation2008; Patel et al., 2013b) have reported a unique connection between the nose and the brain and intranasal delivery of drugs to the brain by passing the blood–brain barrier (Vyas et al., Citation2006; Jogani et al., Citation2008; Patel et al., 2013b). The T1/2 of 2.29–3.52 h (blood), 2.76–3.55 h (brain), and Kel 0.19–0.35 (blood), 0.19–0.25 (brain) were observed irrespective of the routes of administration and the type of the formulations ().
When CMPME (IV) was compared to CMPME (IN) and CMPS (IN), significantly lower Cmax and AUC were observed. The mucociliary clearance under normal circumstances rapidly clears the instilled formulation. However, when mucoadhesive agent was incorporated in the formulation (CMPMME), significant improvement in Cmax and AUC was observed. Comparable AUC to CMPME (IV) was achieved with CMPMME (IN). This demonstrates the value of the mucoadhesive agent in prolonging the contact time of the formulation with the nasal mucosa. Significantly higher AUC (8.74 ± 1.12) and Cmax (1.62 ± 0.54) for CMPME (IN) nasal compared to CMPS (IN) are attributed to ME formulation (Li et al., Citation2002; Zhang et al., Citation2004; Kaur & Kim, Citation2008).
The DTE (%) and brain drug DTP (%) were also calculated for nasally administered formulations and are shown in . The CMPMME showed the highest DTE (%) and DTP (%) values among all the three formulations followed by CMPME and then CMPS. The 2.20 fold higher DTE (%) and 6.62 fold higher DTP (%) for CMPMME compared to CMPS show the benefit of the mucoadhesive ME formulation. The higher DTE (%) and DTP (%) suggest that CMPMME has better brain-targeting efficiency mainly because of substantial direct nose-to-brain transport. These findings are in congruence with the observations reported in literature (Li et al., Citation2002; Zhang et al., Citation2004; Vyas et al., Citation2006; Jogani et al., Citation2008; Kaur & Kim, Citation2008; Patel et al., 2013b) that ME increases nose-to-brain uptake of the drugs.
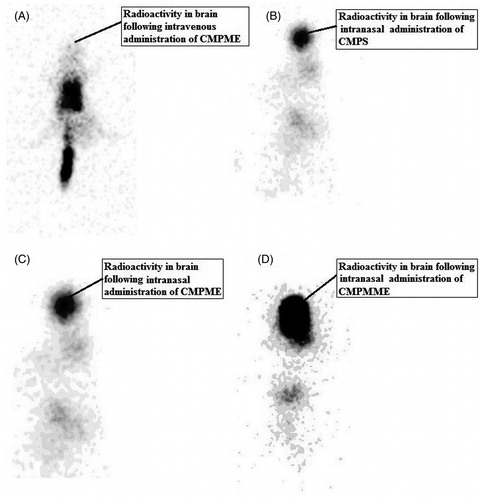
In order to visualize brain uptake following IN and IV administrations of 99mTc-CMP formulation, we used a gamma scintigraphy camera to derive comprehensive biodistribution information. The gamma scintigraphy images of rats 0.50 h post IV injection and IN administrations are shown in . Gamma scintigraphy images showed accumulation of significantly higher radioactivity in the rat brain after IN administration of CMP compared with IV administration. Among IN formulations, CMPMME shows higher radioactivity compared with CMPME and CMPS. The scintigraphy images were consistent with the results shown in and high uptake of CMPMME into the brain was observed.
Figure 2. Gamma scintigraphy of antero-posterior (AP) view of rat following intravenous administration of 99mTc-CMPME (A), intranasal administration of 99mTc-CMPS (B), 99mTc-CMPME (C), and 99mTc-CMPMME (D). Rats were administered 100 µCi radioactivity by intravenous and intranasal administration.
Conclusion
In the present investigation, the utility of ME as carrier for nasal delivery of CMP was studied. All formulations were successes fully prepared, characterized and found suitable for intranasal administration. The results demonstrate superior delivery of CMP to the brain via intranasal route from the formulation containing mucoadhesive agent polycarbophil. The brain-targeting studies reveal that the intranasal administration of CMPMME provide higher brain CMP concentrations compared to the intravenous administration. As a consequence of this, decrease in the dose and frequency of administration for drugs is possible to achieve the desired therapeutic activity. Also, intranasal administration of the drugs will avoid unwanted peripheral tissue distribution of the drugs and hence the associated peripheral side effects. These together will improve the therapeutic efficacy of the drugs.
Given the results of this investigation, the in vitro and in vivo studied demonstrated the potential of developed MME for intranasal delivery of CMP and confirms the existence of a transport pathway for a CMP to the brain directly from the nasal cavity. However, clinical benefits to the risk ratio of the formulation developed in this investigation will decide its appropriateness in the clinical practice for the treatment of epilepsy.
Acknowledgements
Authors are thankful to Max Pharmaceutical (India) for providing the gift sample of pure powder of drugs, Gattefosse (Saint-Priest, France), BASF (Mumbai, India), Noveon (Cleveland, OH) for readily providing gratis samples of excipients, to Veterinary Nuclear Medicine Centre, Bombay Veterinary College, Mumbai, for permitting me to carry out experimental work, to Sophisticated Instrumentation Center for Applied Research and Testing (SICART), Vallabh Vidyanagar, for providing facilities and research assistant.
Declaration of interest
All India Council for Technical Education (AICTE), New Delhi is gratefully acknowledged for financial support (Grant No.8023/BOR/RID/RPS-147). The author(s) confirm that this article content has no conflicts of interest.
References
- Babbar AK, Singh AK, Goel HC, et al. (2000). Evaluation of 99mTc-labeled Photosan-3, a hematoporphyrin derivative, as a potential radiopharmaceutical for tumor scintigraphy. Nucl Med Biol 27:419–26
- Barakat NS, Omar SA, Ahmed AAE. (2006). Carbamazepine uptake into rat brain following intra-olfactory transport. J Pharm Pharmacol 58:63–72
- Chow HS, Chen Z, Matsuura GT. (1999). Direct transport of cocaine from the nasal cavity to brain following intranasal cocaine administration in rats. J Pharm Sci 88:754–58
- Eckelman WC. (1995). Radiolabeling with technetium-99m to study highcapacity and low-capacity biochemical systems. Eur J Nucl Med 22:249–63
- Elshafeey AH, Bendas ER, Mohamed OH. (2009). Intranasal microemulsion of sildenafil citrate: in vitro evaluation and in vivo pharmacokinetic study in rabbits. AAPS PharmSciTech 10:361–4
- Jogani VV, Shah PJ, Mishra P, et al. (2008). Intranasal mucoadhesive microemulsion of tacrine to improve brain targeting. Alzheimer Dis Assoc Disord 22:116–24
- Kaur P, Kim K. (2008). Pharmacokinetics and brain uptake of diazepam after intravenous and intranasal administration in rats and rabbits. Int J Pharm 364:27–35
- Li L, Nandi I, Kim KH. (2002). Development of an ethyl laurate-based microemulsion for rapid-onset intranasal delivery of diazepam. Int J Pharm 237:77–85
- Patel RB, Patel MR, Bhatt KK, Patel BG. (2013a). Formaulation and evaluation of microemulsion based drug delivery system for intranasal administration of olanzapine. Int J Bimed Pharm Sci 7:20–7
- Patel RB, Patel MR, Bhatt KK, et al. (2013b). Risperidone microemulsion for transnasal delivery: pharmacodynamic and pharmacokinetic evaluation. Pharm Nanotech 1:44–53
- Patel RB, Patel MR, Bhatt KK, Patel BG. (2013c). Paliperidone loaded mucoadhesive microemulsion in treatment of schizophrenia: formulation consideration. J Pharm Inn 8:195–204
- Patel RB, Patel MR, Bhatt KK, Patel BG. (2013d). Formulation consideration and characterization of microemulsion drug delivery system for transnasal administration of Carbamazepine. Bul Facul Pharm Cairo Uni 51:243–53
- Patel RB, Patel MR, Bhatt KK, Patel BG. (2010). Development and validation of HPTLC method for estimation of carbamazepine in formulations and its in vitro release study. Chromatogr Res Inter 2011:1–8. (DOI:10.4061/2011/684369)
- Shinde RL, Jindal AB, Devarajan PV. (2011). Micromeulsions and Nanoemulsions for targeted drug delivery to the brain. Current Nanosci 7:119–33
- Vyas TK, Babbar AK, Sharma RK, et al. (2006). Intranasal mucoadhesive microemulsions of clonazepam: preliminary studies on brain targeting. J Pharm Sci 95:570–80
- Zhang Q, Jiang X, Jiang W, et al. (2004). Preparation of nimodipine-loaded microemulsion for intranasal delivery and evaluation on the targeting efficiency to the brain. Int J Pharm 275:85–96