Figures & data
Figure 1. Radiobiology of the bystander effect. (A, B) The figure summarizes the main features of the reported radiation technique for the induction of the bystander effect by partially irradiating only the hypoxic tumor segment. An 18F-FDG PET in combination with a contrast enhanced CT, previously fused with the simulation CT, was used for the definition of the hypoxic tumor segment, a so called ‘bystander target’ (a smaller contour). This area, which includes the junctional region between the necrotic tumor segment (central region) and the contrast-enhanced and PET-positive remainder peripheral tumor (a bigger contour that was not targeted for irradiation), was targeted with high-dose radiation. The arrows represent the bystander signals (pellets) released by the irradiated hypoxic segment, which transmit damage to the remainder of the un-irradiated part of the tumor, causing regression of the whole tumor, both in the targeted and non-targeted region.
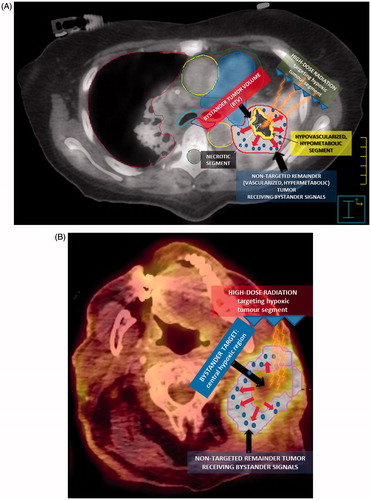
Table 1. Main characteristics of seven patients treated at radiotherapy institute ‘KABEG Klinikum, Klagenfurt am Wörthersee’.
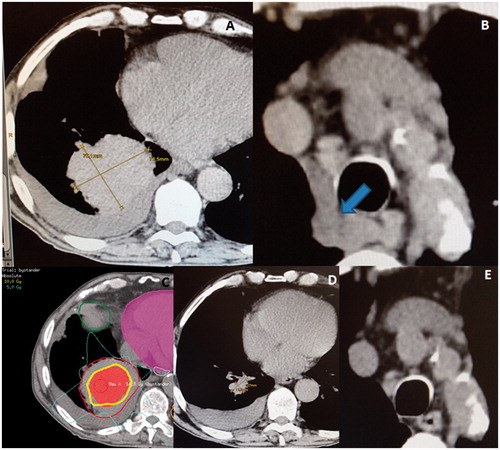
Figure 2. (A) A very voluminous squamous cell carcinoma of the right lung, with a maximum diameter of 10 × 9 cm at the time of the radiotherapy. (B) The arrow showing the asymptomatic mediastinal lymphadenopathies. (C) An induction of the bystander effect with a high-dose partial irradiation of the gross tumor volume (GTV, bigger contour) by targeting the central hypoxic region (smaller area). The centrally located isodose-line corresponds to 10 Gy. (D) A dramatic regression of the treated lesion only 3 weeks later. (E) An abscopal effect among the untreated mediastinal lymphadenopathies.