Figures & data
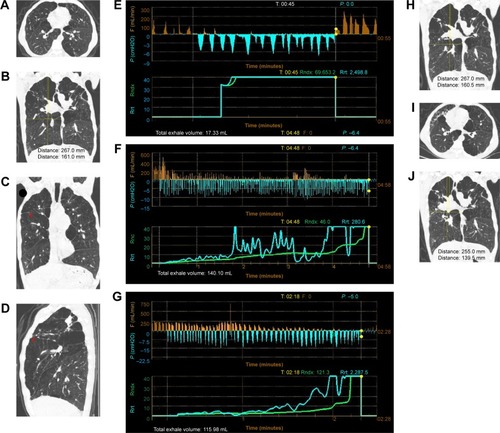
Figure 1 Chest HRCT and Chartis reading of the patient.
Notes: (A) HRCT of the chest upon admission in the horizontal section. (B) HRCT of the chest upon admission. Heterogeneous emphysema was present in both upper lobes and the middle lobe. The right diaphragm was lower than the left diaphragm, indicating significant hyperinflation. The long vertical line indicates the distance from the apex of the right lung to the highest point of the right diaphragm (267 mm). The short vertical line indicates the distance from the apex of the right lung to the oblique fissure (161 mm). (C) A minor leak in the horizontal fissure seen in a coronary view (red arrow). The minimal integrity of the horizontal fissure in a coronary view was 91.6%. (D) A minor peripheral leak in the horizontal fissure in the sagittal view (red arrow). The minimal integrity of the horizontal fissure was 91%. The lesions in the RUL had obvious calcification and no evidence of malignancy. (E) A Chartis reading for the RUL showing sudden stops in expiratory flow during the three breathing maneuvers that were accompanied by a sharp increase in the airway resistance index. The total expiratory volume was only 17.33 mL, confirming the low-flow phenotype that resulted from distal airway collapse. (F) A Chartis reading for the RML revealed a flow signal with a gradual downward trend that resulted in no flow until 4 min after the activation of the valve. This effect might have been related to the absence of CV or a CV-positive status with on and offs during deeper and lower breathing maneuvers related to mini-collaterals. (G) A Chartis reading for the RLL showing a good signal with a gradual downward trend that was indicative of CV-negative status. (H) HRCT of the chest 1 month after EBV insertion into the right upper bronchus. No obvious changes relative to the CT scan taken on admission were observed, and no evidence of RUL collapse was present. (I) Comparison of HRCT images of the chest taken at baseline to those acquired 2 weeks after EBV insertion into the middle bronchus. The mediastinum shifted to the right side, and the volume of the RML was decreased. (J) HRCT of the chest 2 weeks after EBV insertion into the middle bronchus. The RUL and RML had begun to shrink, and the RLL re-expanded. The right diaphragm appeared to be higher than before. The long vertical line indicates the distance from the apex of the right lung to the highest point of the right diaphragm (255 mm). The short line next to the long line indicates the distance from the apex of the right lung to the oblique fissure (139.5 mm). Both lines were obviously shortened compared with the baseline results.
Abbreviations: CT, computed tomography; CV, collateral ventilation; EBV, endobronchial valve; HRCT, high-resolution chest CT; RLL, right lower lobe; min, minutes; RML, right middle lobe; RUL, right upper lobe.
Abbreviations: CT, computed tomography; CV, collateral ventilation; EBV, endobronchial valve; HRCT, high-resolution chest CT; RLL, right lower lobe; min, minutes; RML, right middle lobe; RUL, right upper lobe.