
Figures & data
Figure 1 Eosinophil trafficking from bone marrow to airway.
Notes: Eosinophil activity occurs in tissue. Mature eosinophils leave bone marrow, circulate in blood, and migrate to tissue under the influence of various chemotactic factors. Infiltration into the airways is mediated through adhesion and transmigration across the bronchial vascular epithelium. Chemokines, such as CCL5 and CCL11, and other factors play roles in this process. Reprinted with permission of Sage Publications, Ltd. George L, Brightling CE. Therapeutic Advances in Chronic Disease. 2016;7(1):34–51, Copyright 2016.Citation12
Abbreviation: GM-CSF, granulocyte-macrophage colony-stimulating factor.
Abbreviation: GM-CSF, granulocyte-macrophage colony-stimulating factor.
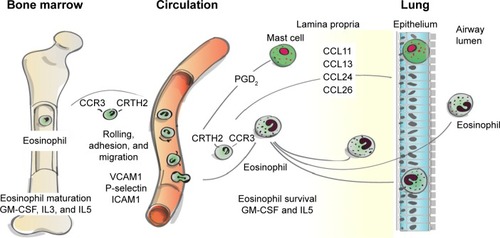
Table 1 Eosinophil thresholds and findings in recent COPD clinical trials
Figure 2 Hospital admissions due to exacerbations in COPD patients treated to optimize symptoms alone or in combination with minimizing eosinophil counts.
Notes: Patients treated to optimize symptoms only (□; n=11); and those treated to optimize symptoms and minimize airway eosinophil inflammation (minimize eosinophilia, keeping sputum eosinophil at <3%) (•; n=12). For patients in the optimize symptoms only group, the hierarchy of treatment was short-acting β2-agonist, regular anticholinergic, LABA, LAMA, theophylline, and then a trial with a nebulizer; inhaled corticosteroids continued at the same dosage if the patient was already receiving them. For patients in the optimize symptoms and minimize sputum eosinophils group, treatment hierarchy was the same as above. However, patients received the smallest appropriate dosage of anti-inflammatory treatment (ICS or oral CS) to keep sputum eosinophil counts <3%; if eosinophil counts were >3%, then anti-inflammatory treatment was increased. Reproduced with permission of the European Respiratory Society from Siva R, Green RH, Brightling CE, et al. Eosinophilic airway inflammation and exacerbations of COPD: a randomised controlled trial. Eur Respir J. 2007;29(5):906–913.Citation78 [Disclaimer: This material has not been reviewed prior to release; therefore, the European Respiratory Society may not be responsible for any errors, omissions, or inaccuracies, or for any consequences arising there from, in the content.]
Abbreviations: CS, corticosteroid; ICS, inhaled corticosteroid; LABA, long-acting β-agonist; LAMA, long-acting muscarinic antagonist.
Abbreviations: CS, corticosteroid; ICS, inhaled corticosteroid; LABA, long-acting β-agonist; LAMA, long-acting muscarinic antagonist.
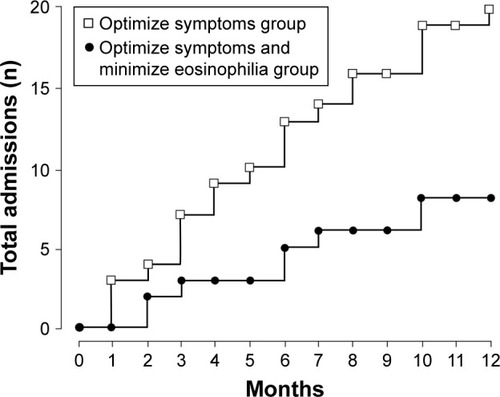
Table 2 Consideration for inclusion/exclusion of ICS as part of therapy
Table 3 Recent and ongoing trials for monoclonal antibody treatments targeting eosinophils in COPD