
Figures & data
Figure 1 The pathophysiology of myasthenia gravis. Peripheral naive B-cells encounter an antigen and then, with the aid of T-cells in the thymus, produce memory antibody-producing B-cells, which later differentiate into either short-lived or long-lived plasma cells. These cells can secrete both AchR antibodies and Anti-MuSK antibodies. Both autoantibodies migrate to the neuromuscular junction and can interfere with the neuromuscular transmission, binding with AchR or by binding MuSK and impairing the neuromuscular transmission by blocking the interaction between LRP4 and MuSK, which is essential for the clustering of the AchR. Most of the AchR antibodies are of the IgG1 subclass, which can induce the complement cascade, while anti-MuSK antibodies are of the IgG4 subclass and are less effective in activating the complement pathway.
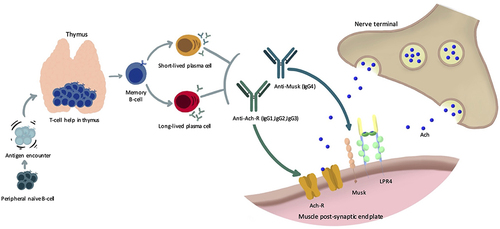
Figure 2 A 73-year-old lady was referred with a history of diplopia. Examination shows right ptosis and left upper lid retraction (Hering’s law). She had a bilateral adduction deficit (pseudo-bilateral internuclear ophthalmoplegia). MRI of the brain was normal, the ice test was positive, and she had positive AchR-antibodies.
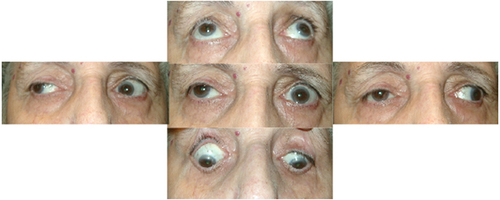
Figure 3 The ice test is unequivocally positive in this patient, presenting with progressive ptosis worsening with fatigue (above). Significant improvement is noticed after placing ice packs for 2 minutes over the eyelids (below).
