
Figures & data
Figure 1 (A) Clinical manifestation of palmar psoriasis. (B) Clinical manifestation of sacral psoriasis. (C) Clinical manifestation of nail psoriasis. All the three clinical images report the difficult-to-treat areas, recognized as unmet needs by patients and physician. (D) Histopathological features of plaque psoriasis. The classic epidermal psoriasiform hyperplasia is associated with hyperparakeratosis and loss of granular layer. Collections of neutrophils are observed in the upper stratum spinosum (spongiosiform pustules of Kogoj). In the dermis, thin capillary vessels reach almost the top of the dermal papillae and are surrounded by a chronic lymphocytic infiltrate with sparse neutrophils (Haematoxylin-eosin. Original magnification: 100x). (E) Histopathological features of genital psoriasis. The classic features observed in plaque psoriasis are attenuated in the genital area. The epidermal hyperplasia is associated with less extensive hyperparakeratosis, which is accompanied by mounds of neutrophils in the stratum corneum (Munro’s microabscesses). In the chorion, thin capillary vessels are surrounded by a chronic lymphocytic infiltrate, with sparse neutrophils (Haematoxylin-eosin. Original magnification: 200x).

Table 1 The Table Shows the Molecules Belonging to the Class of Jak Kinase Inhibitor Under Investigation for Psoriasis
Figure 2 Summary of drugs under investigation or with preliminary efficacy in psoriasis disease (red), and drugs with no data reporting efficacy (orange). A) The JAK inhibitor blocks the JAK-STAT pathway signaling in Th17 cells. Specifically, deucravacitinib inhibits TYK2. B) Tapinarof, an AhR agonist, reduces IL-17 and IL-22 in both Th17 cells and keratinocytes. C) Spesolimab and imsidolimab inhibit IL-36R. D) Imo-8400 inhibits TLR-7/8/9. E) BAY1834345, ND2110 and ND2158 inhibit IRAK4. F) Piclidenoson inhibits A3AR in keratinocytes. G) Ponesimod, a selective S1PR1 agonist, induces sequestration of lymphocytes into lymph nodes and decreases peripheral lymphocyte counts and tracking of lymphocytes to peripheral tissues. H) Namilumab has not shown efficacy in psoriasis. J) PDE4 inhibitors act on lymphocytes. K) Among RORγt, just ABVV-157 and AUR-101 have shown efficacy in psoriasis. L) KD025, a ROCK2 inhibitor, reduces IL-17 secretion in Th17 cells.
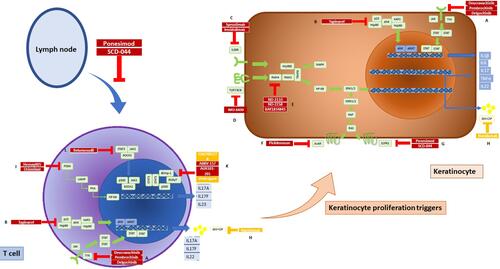
Table 2 The Table Shows the Molecules Belonging to the Class of Aryl Hydrocarbon Receptor Agonist Under Investigation for Psoriasis
Table 3 The Table Shows the Molecules Belonging to the Class of Retinoic Acid-Related Orphan Receptor γt Inverse Agonists Under Investigation for Psoriasis. Vimirogant and GSK2981278 are Reported in the Table S19 Due to Any Efficacy in the Pathology
Table 4 The Table Shows the Molecules Belonging to the Class of Sphingosine-1-Phosphate Receptor 1 Agonist Under Investigation for Psoriasis
Table 5 The Table Shows the Molecules Belonging to the Class of Rho-Associated Coiled-Coil Kinase 2 Inhibitor Under Investigation for Psoriasis
Table 6 The Table Shows the Molecules Belonging to the Class of Interleukin-1 Receptor Associated Kinase 4 Inhibitor Under Investigation for Psoriasis
Table 7 The Table Shows the Molecules Belonging to the Class of Phosphodiesterase-4 Inhibitors Under Investigation for Psoriasis
Table 8 The Table Shows the Molecules Belonging to the Class of A3 Adenosine Receptor Agonist Under Investigation for Psoriasis
Table 9 The Table Shows the Molecules Belonging to the Class of Toll-Like Receptor Antagonist Under Investigation for Psoriasis
Table 10 The Table Shows the Molecules Belonging to the Class of Interleukin-36 Receptor Inhibitors Under Investigation for Psoriasis