
Figures & data
Table 1 Characteristics of Severe Acute Pancreatitis-Associated Cardiac Injury
Figure 1 Data related to acute pancreatitis. (A and B): proportion and mortality in acute pancreatitis of different severity. (C and D): proportion and mortality of acute pancreatitis complicated with organ failure.
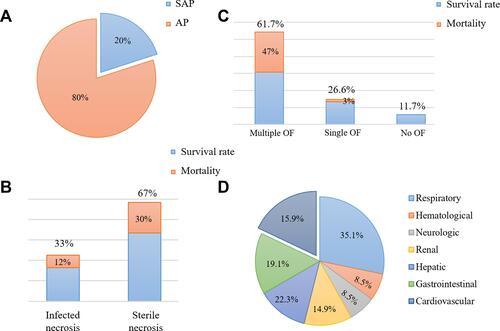
Figure 2 Pathophysiological mechanisms influencing the development of cardiac injury in SAP. Various risk factors (gallstones, alcohol, diet and drugs) cause acinar cell damage and the release of pancreatic hydrolase, leading to excessive activation and autocrine of macrophages and neutrophils, resulting in the accumulation of a large number of pro-inflammatory factors. Then the local inflammation at the lesion is amplified through the inflammatory cascade effect, which eventually results in necrosis and hemorrhage of most pancreatic tissue, releasing more and more cytokines, and induces hypercytokinemia (a cytokine storm). As the disease progresses and pancreatic inflammation involves the intestine, it causes dysfunction of intestinal barrier, which leads to the migration of intestinal flora to the pancreas and blood, followed by pancreatic infection and sepsis. These high levels of risk factors (including trypsin, endotoxin and cytokines) in the blood can damage vascular endothelial cells, trigger systemic inflammatory response, lead to myocardial microcirculatory disturbance, autonomic nerve dysfunction and abnormal autophagy, and eventually result in myocardial injury and cardiac dysfunction.
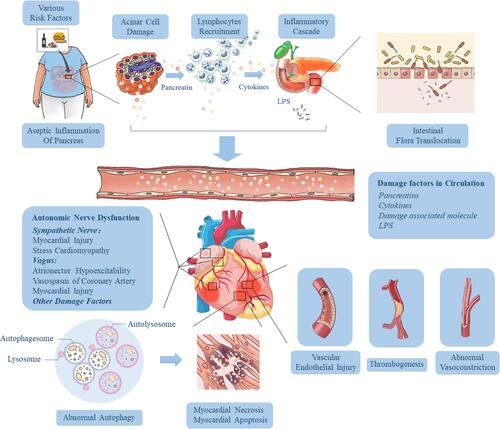
Figure 3 The specific pathways of myocardial injury and cardiac dysfunction caused by inflammation-related factors. DAMPs and PAMPs such as HMGB1, ATP and endotoxin from the pancreas and intestine act on membrane receptors such as TLR and P2X7R to recruit inflammatory cells (macrophages, neutrophils and dendritic cells) in serum, activate classical inflammatory pathways such as NF-κB and NLRP3 inflammasome in inflammatory cells, release a large number of pro-inflammatory cytokines, and form a cascade reaction (upper). These inflammatory factors eventually act on cardiomyocytes, causing myocardial energy metabolism disorder, systolic myocardial dysfunction, myocardial hypertrophy, apoptosis and fibrosis through a complex network of signaling pathways (lower).
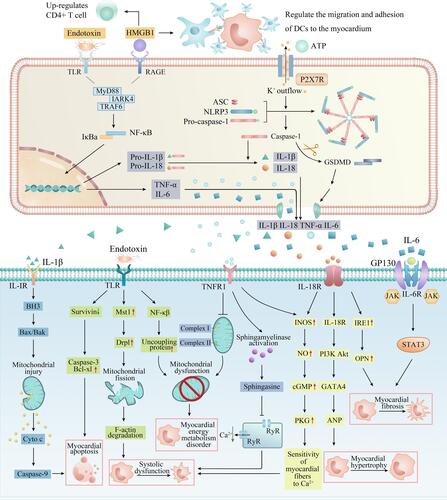
Table 2 Markers with Predictive or Prognostic Value for SAP-Associated Cardiac Injury
Table 3 Prevention and Treatment of SAP-Associated Cardiac Injury