Figures & data
Table 1 FGFs and Its Specific FGF Receptors
Figure 1 An overview of the FGF signaling pathways. (A) Activation of FGFRs by FGFs via the paracrine pathway, mediated by HS cofactor. (B) Activation of FGFR by FGF-Klotho-FGFR ternary complex. The complex formation is regulated via the Endocrine pathway, mediated by Klotho protein cofactor. (C) Regulation of functioning of various signal transduction pathways such as growth and development in the human body by FGF-activated FGFR.
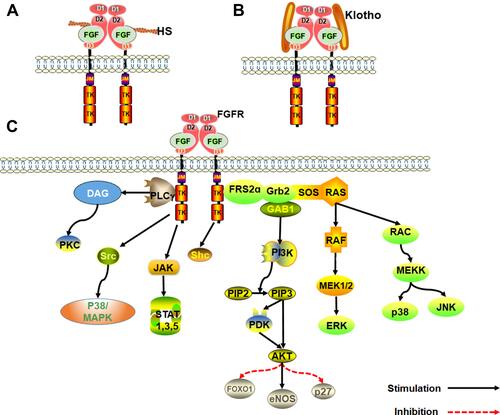
Figure 2 Pathological characteristics of DN. The first clinical manifestation of classical DN is the increase of urinary albumin excretion. The glomerular filtration rate is normal or even increased before urinary albumin excretion, but the glomerular filtration rate decreases after continuous urinary proteinuria, and eventually even developed into ESRD. And with increased urinary albumin excretion and an independent decline in glomerular filtration function, the patient’s risk of cardiovascular disease increases. According to the Tervaert classification of DN, the glomerular lesions of DN can be divided into four grades. I: Irregular thickening of the glomerular basement membrane was observed under an electron microscope. II: Mesangial hyperplasia and mesangial dilatation occur. III: There is at least one recognized tuberous sclerosis. IV: Advanced diabetic glomerulosclerosis of glomeruli.
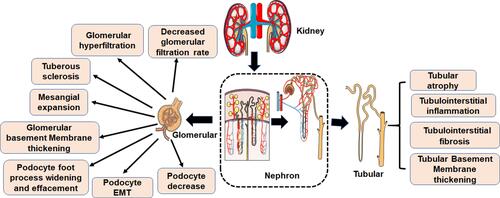
Table 2 Ongoing Human Clinical Trials of FGF
Figure 3 Effect of FGF1 on DN. FGF1 can ameliorate cell stress, inflammation, fibrosis and kidney injury.
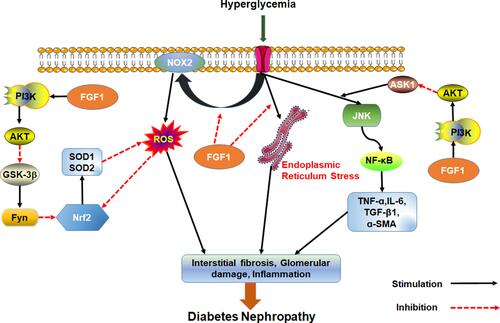
Figure 4 The effect of FGF2 on EMT in renal tubular epithelial cells. The effect of Albuminuria, AGEs and FGF2 on PI3K/AKT pathway mediated expression of HPSE. HPSE can hydrolyze HSPG to generate HS fragments and inhibit the overexpression of multiligand proteoglycan-1, essential for FGF2 activation of. In addition, HPSE regulate the expression and activity of TGF-β.
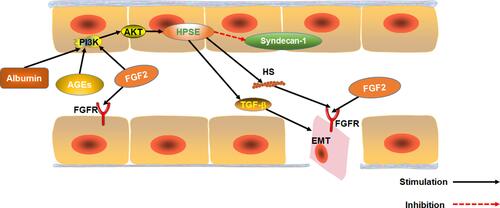
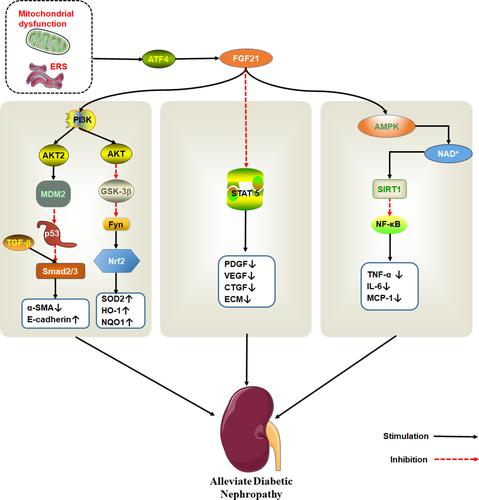
Figure 5 The therapeutic effect of FGF21 on DN. Endoplasmic reticulum stress activates ATF4, which induce FGF21 expression. FGF21 protects kidney damage by activating multiple signaling pathways. PI3K/AKT pathway is shown to the left, STAT5 pathway in the middle and AMPK/SIRT1 on the right.