
Figures & data
Table 1 Independent predictors of PAH in SLE
Figure 1 A schematic representation of the pathogenesis of PAH in SLE.
Notes: Pulmonary and cardiac involvement as well as disequilibrium between vasodilators (prostacyclin, PGI2) and vasoconstrictors (ET-1 and, TXA-2) will lead to hypoxia and vasoconstriction. Hyperexpression of HIF and EPO will drive impaired smooth muscle, endothelial, and adventitial cell proliferation and apoptosis. In parallel, the accumulation of inflammatory cells into the elastic lamina of the pulmonary arteries and the secretion of certain cytokines and growth factors will lead to abnormal vascular remodeling, and thus increased PVR. In selected cases, thrombosis of the pulmonary circulation in the presence of antiphospholipid antibodies and other prothrombotic factors, will also contribute to increased PVR and PAH. The role of the anti-endothelial cell antibodies AECA and other immune mediators has not been clarified yet.
Abbreviations: PAH, pulmonary arterial hypertension; SLE, systemic lupus erythematosus; ET-1, endothelin-1; TXA-2, thromboxane A2; HIF, hypoxia-inducible factor; EPO, erythropoietin; PVR, pulmonary vascular resistance; AECA, anti-endothelial cell antibodies.
Abbreviations: PAH, pulmonary arterial hypertension; SLE, systemic lupus erythematosus; ET-1, endothelin-1; TXA-2, thromboxane A2; HIF, hypoxia-inducible factor; EPO, erythropoietin; PVR, pulmonary vascular resistance; AECA, anti-endothelial cell antibodies.
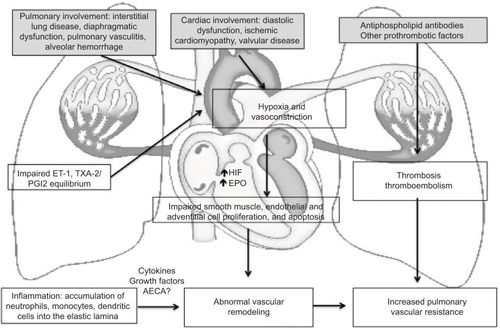
Table 2 Studies with immunosuppressive medications for SLE-PAH
Table 3 Studies with PAH-targeted therapy medications for SLE-PAH