Figures & data
Figure 1 The pathophysiological substrate of diabetic cardiomyopathy: in diabetes, hyperglycemia, excess free fatty acid (FFA) release, and insulin resistance, engender adverse metabolic events that affect the cardiac myocytes. Hyperglycemia is associated with decreased glucose transportation (GLUT), uptake, and oxidation, as well as increased formation of advanced glycation end products (AGEs) and increased activation of protein kinase C (PKC). Excess FFA release is followed by cardiac lipotoxicity, ie, increased cardiac lipid accumulation and increased generation of reduced reactive oxygen species (ROS) at the level of the electron transport chain. Together with insulin resistance and impaired insulin action and signaling, these metabolic paths augment vasoconstriction, produce and further aggravate arterial hypertension, increase inflammation with liberation of leukocyte-attracting chemokines, increase production of inflammatory cytokines, and augment expression of cellular adhesion molecules. Thrombosis is further promoted, together with platelet activation.
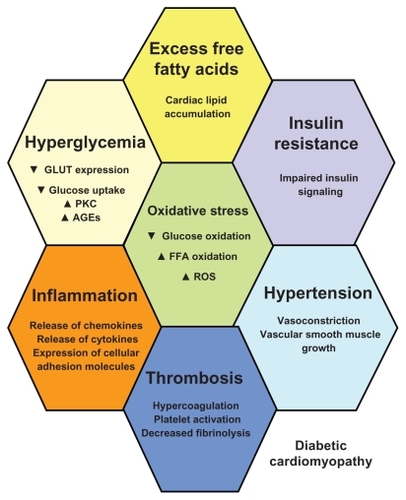
Table 1 Main and recent echocardiographic, population-based studies on diabetic cardiomyopathy
Table 2 Major studies on treatment strategies of diabetic cardiomyopathy