Figures & data
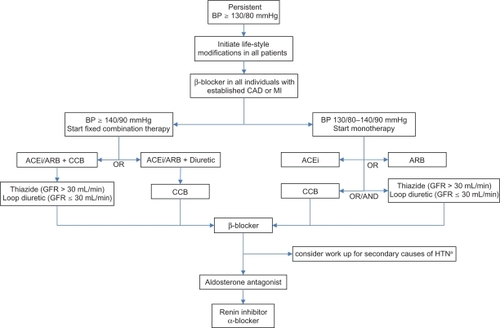
Figure 1 Algorithm for treatment of hypertension in inividuals with diabetes. Maximize dose before starting the next drug.
First line = ACEi or ARB (equivalence seen in DETAILCitation73 ONTARGETCitation75 and VALIANTCitation76).
Both reduce microalbuminuria and rate of nephropathy independently of their antihypertensive effect.
ACEi preferred over ARB (indirect evidence for cardiovascular outcomes; SCOPE,Citation70 VALUECitation71 and TRANSCENDCitation72).
Recommend against concomitant use of ARB with ACEi (ONTARGETCitation75 and VALIANTCitation76).
Second line = CCB or diuretic
Dihydropyridine CCB favored over diuretic (ACCOMPLISHCitation82 and GUARDCitation83) or in the presence of electrolyte anomalies.
Diuretic preferred in heart failure or edematous conditions.
Loop diuretic recommended if GFR ≤ 30 mL/min due to marked state of fluid overload.
If needed, CCB and diuretic can be combined.
Third line = β-blocker, primarily due to side effect profile. However, it is indicated in all patients with established CAD and MI.
Fourth line = Aldosterone antagonist (ASCOT-BPLACitation86).
Fifth line = Renin inhibitor or α-blocker, not enough comparative data from clinical trials for clear recommendation.
Peripheral α-blocker, due to orthostatic hypotension and results of ALLHAT.Citation78 It could be used earlier in patients with symptomatic BPH.
arenal artery stenosis, hyperaldosteronism, Cushing’s syndrome or pheochromocytoma.