Figures & data
Table 1. Common neuronal firing patterns and stimulation-induced effects encountered during deep brain stimulation surgery for movement disorders.
Table 2. Local field potentials associated with movement disorders.
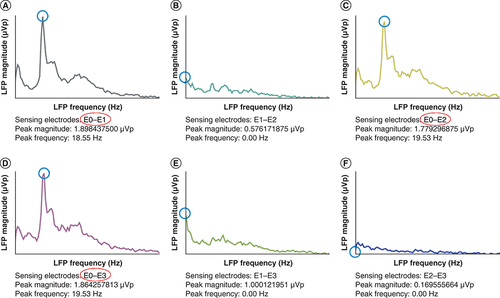
Conventional monopolar review based on acute clinical responses during initial DBS programming yielded equivalent therapeutic windows for contacts E0 and E1. Consistent with the monopolar review, the LFP survey demonstrated low beta (13–20 Hz) frequency peaks of higher amplitude in the regions between contacts (A) E0 and E1, (C) E0 and E2 and (D) E0 and E3. There were no significant beta peaks in the regions between contacts (B) E1 and E2, (E) E1 and E3 and (F) E2 and E3. Thus, initial DBS settings were programmed using contact E0 since the three regions with low beta LFPs shared contact E0 and the highest amplitude (1.89 μVp) was found in the region between contacts (D) E0 and E1. LFP measurements were obtained in the dopaminergic medication OFF state by the Percept DBS system (Medtronic).
DBS: Deep brain stimulation; LFP: Local field potential.
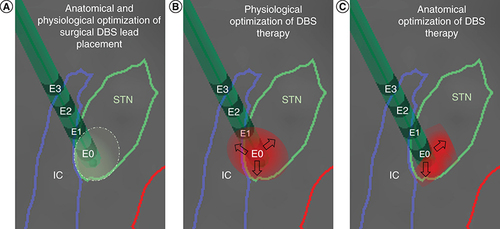
(A) During surgical implantation of the left STN DBS lead, microelectrode recordings and stimulation defined a physiologically optimized trajectory and target in the dorsolateral region of the anatomically defined left STN. (B) During the initial programming session described in , contact E0 was chosen to deliver DBS to the region with the highest peak of low beta LFPs. Upon subsequent DBS amplitude increase, the patient developed subtle side effects due to lateral spread of stimulation toward the IC, which limited the benefits of DBS. (C) With directional stimulation using segmented leads, this lateral spread of stimulation could be theoretically avoided and DBS therapy could be further optimized. Reconstruction of neuroanatomical structures and DBS lead localization were performed by merging pre-operative brain MRI and post-operative CT using BrainLab.
CT: Computed tomography; DBS: Deep brain stimulation; IC: Internal capsule; LFP: Local field potential; STN: Subthalamic nucleus.