Figures & data
Figure 1. The 16 categories of the Neer classification. A fracture is considered displaced if one or more of the four anatomical segments (greater tuberosity, lesser tuberosity, the humeral head, or the humeral shaft) are displaced more than 1 centimeter or angulated more than 45°. Modified from Neer (Citation1970) 15 with permission from JBJS Am, Rockwater Inc.
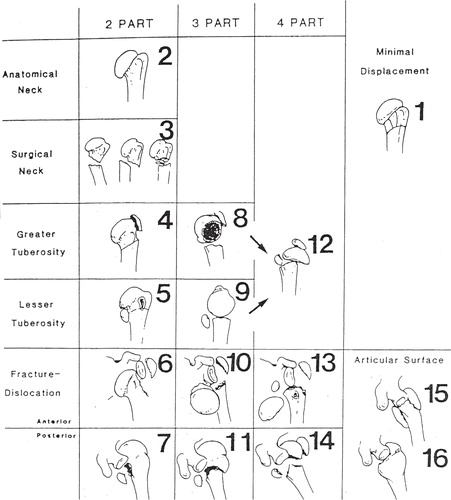
Figure 2. The AO/OTA classification consists of three types, nine groups, and 27 subgroups hierarchically organized according to prognosis. Type A fractures are unifocal and extraarticular, type B are bifocal and extraarticular while type C fractures are intraarticular. Reprinted from Marsh (Citation2007) 19 with permission from J Orthop Trauma, Copyright Clearance Center.
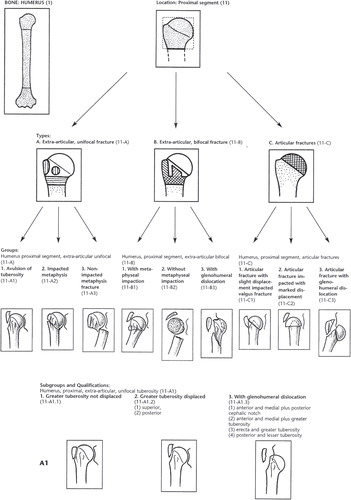
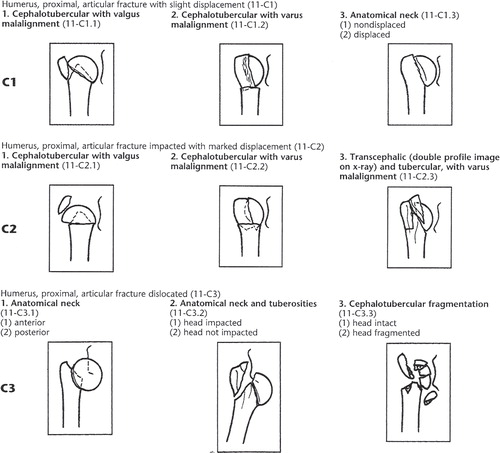
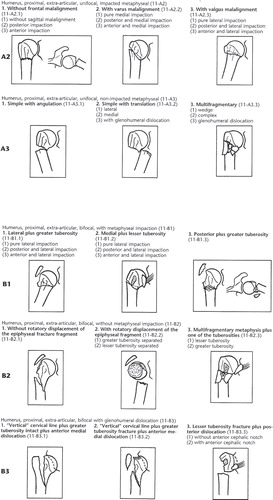
Figure 3. Locking plate for proximal humeral fractures (Philos). Reprinted with permission from Synthes.
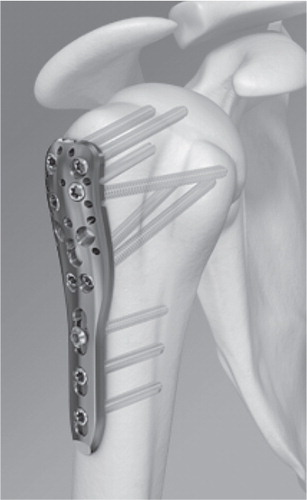
Figure 4. Reverse shoulder arthroplasty (DeltaXtend). Reprinted with permission from DePuy International Limited.

Figure 5. The Edwin Smith Papyrus (copied c. 1600 BC). Column XII and XIII including three cases on humeral fractures. Reprinted from Allen (Citation2005) 81 with permission from The New York Academy of Medicine Library.
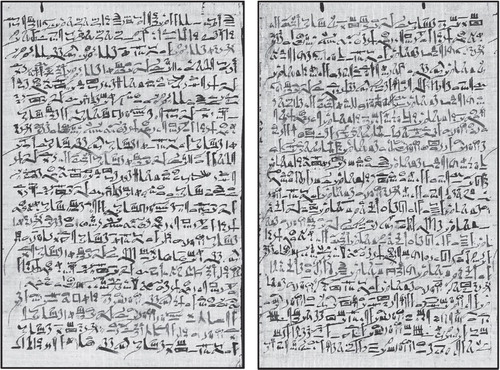
Figure 6. Healed fracture of a left proximal humerus (posterior view). Young woman. First or middle part of New Kingdom (c. 1539–1075 BC). Reprinted with permission from Laboratory of Biological Anthropology, University of Copenhagen.
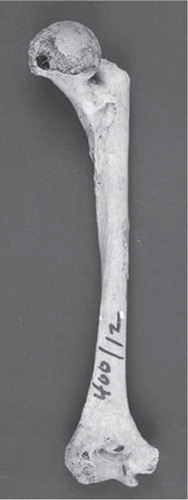
Figure 7. Reduction of a fractured humerus according to De Fracturis (c. 415 BC). Reprinted from É. Littré (Citation1841) 152.
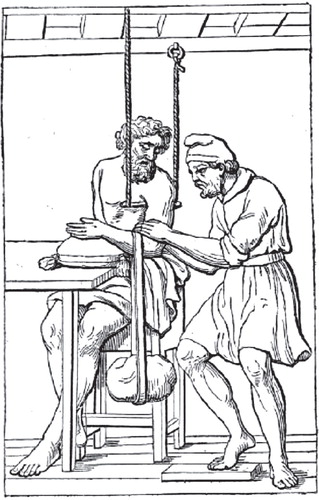
Figure 8. Velpeau’s bandage. Reprinted from Bergmann and Bruns (Citation1901) 153.
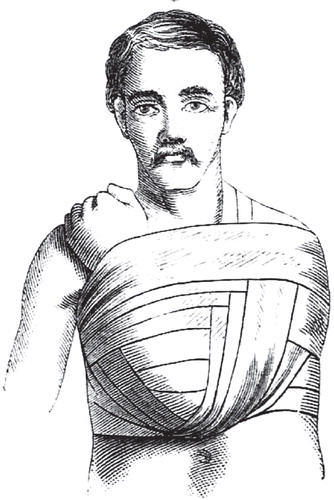
Figure 9. Leonardo da Vinci. The shoulder viewed from above (c. 1510–13)91.
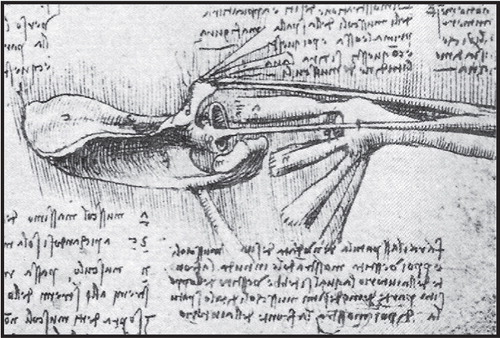
Figure 10. Desault’s three-layer bandage recommended for immobilisation of fractures of the clavicle and the proximal humerus. The bandage was also used for immobilisation of glenohumeral dislocations. Reprinted from Desault (Citation1805) 95.
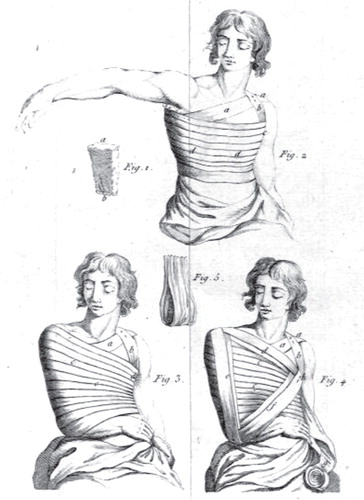
Table I. Classification of fractures of the proximal humerus. Translated and modified from Thudichum (Citation1851)
Figure 11. Unreduced fracture-dislocation of the proximal humerus. Reprinted from Thudichum (Citation1851) 100.
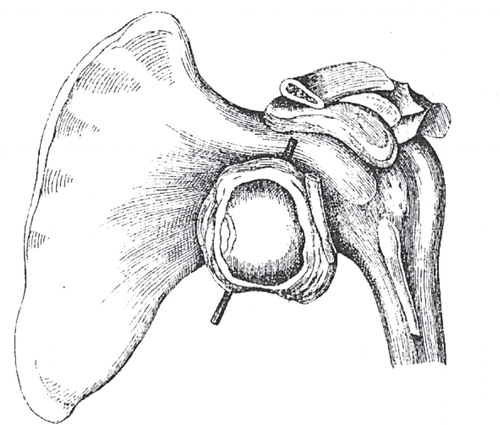
Figure 12. Liston’s bandage. Reprinted from Liston (Citation1838) 101.
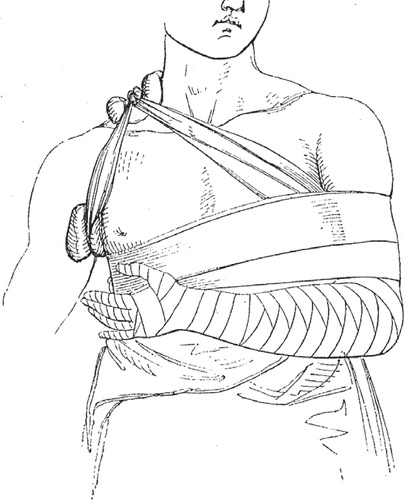
Figure 13. Middledorpf’s triangle. Reprinted from CitationStimson (1899) 102.
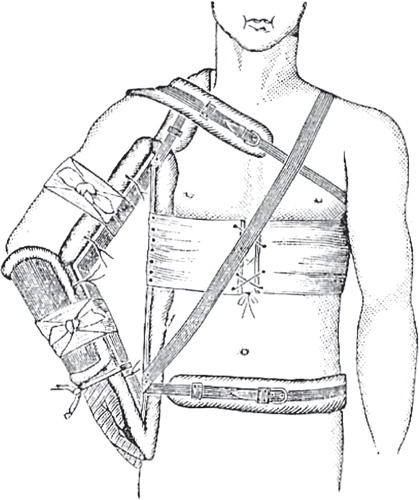
Figure 14. Adhesive plaster bandage and permanent traction. Reprinted from Hamilton (1865)154.
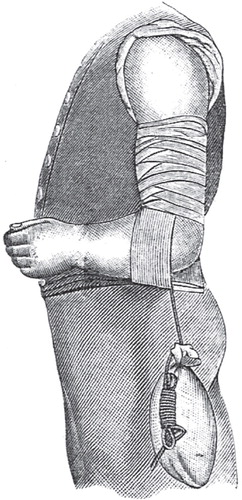
Figure 15. Bardenheuer’s extension apparatus. Reprinted from CitationHoffa (1888) 104.
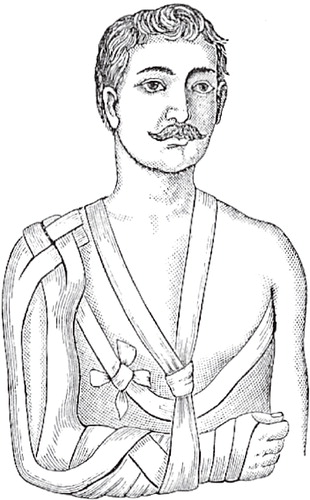
Figure 16. Hennequin’s plaster splint. Reprinted from Stimson (1887)102.
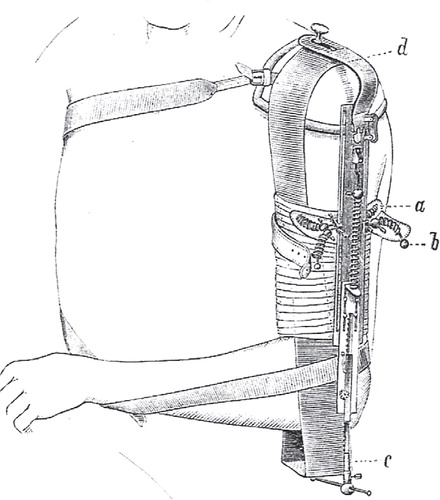
Figure 17. Kocher’s approach to classification of fractures of the proximal humerus and the proximal femur. Reprinted from Kocher (Citation1896) 108.
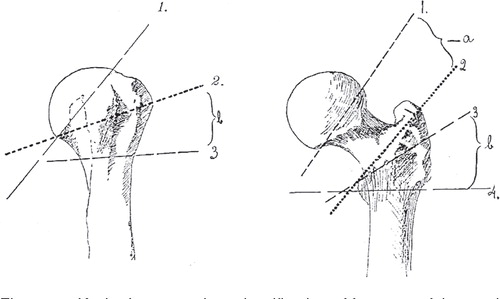
Figure 18. The four anatomical segments of the proximal humerus. Reprinted from Codman (Citation1934) 110 with permission from Krieger Publishing Company.
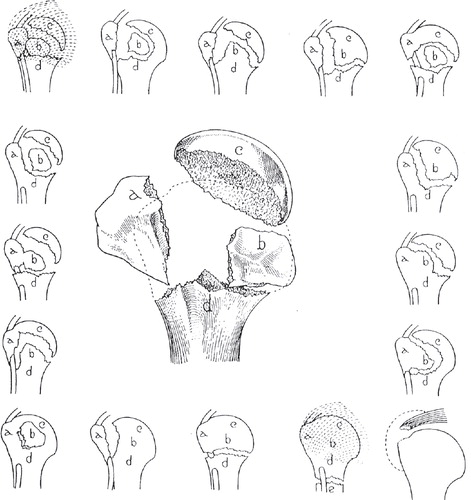
Table II. Mean kappa values (95% CI) for agreement on the Neer classification at three levels of clinical experience
Table III. Mean (95% CI) kappa values for classification according to Neer
Table IV. Inter-observer agreement in 12 observer-studies (mean kappa and/or range of kappa)
Table V. Mean kappa-values (95% CI) for interobserver agreement between five shoulder surgeons
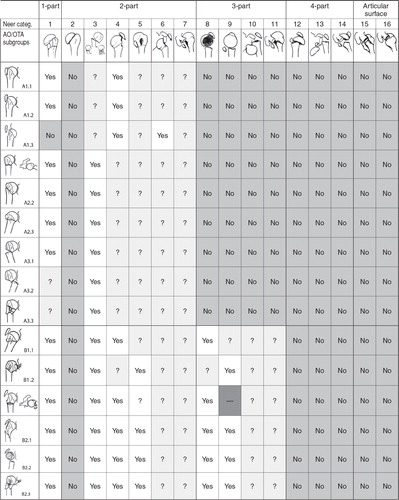
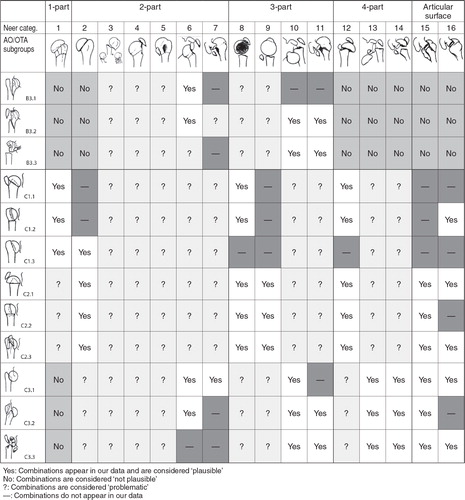
Table VI. Plausibility of combinations between the Neer- and the AO/OTA-classification