
Abstract
Purpose
With undergraduate medical education shifting to an integrated, student-centered approach, self-regulated learning (SRL) skills are critical for student success. Educational research holds that learning strategy effectiveness is context dependent. Our study aims to explore what strategies medical students use to support SRL when engaged in the specific context of an integrated, student-centered curriculum.
Approach
This study took place in two medical schools with integrated, student-centered curricula. Semi-structured interviews were conducted with first-year medical students from both schools, asking them to reflect on the learning strategies they used throughout their first year of medical school. Interview data was analyzed first deductively using the SRL framework and then inductively to understand the specific strategies being used.
Findings
Students engaged in strategies to support SRL in ways that were unique to the integrated, student-centered context. We found that medical students developed strategies to plan for integration and building connections across material during all three phases of self-regulated learning.
Insights
By identifying specific tasks and behaviors students utilized during their first year of medical school, this study provides a roadmap that students and educators can use to help students become self-regulated learners.
Practice points
Engaging in self-regulated learning is an important skill for medical students to master, however they may not have a specific plan for how to implement such a learning style.
This study provides a roadmap for the learning strategies students use in the forethought, performance, and self-reflection phases of self-regulated learning in an integrated, student-centered medical school curriculum.
Students described shifting their forethought behaviors to better plan for the integration of material, and to develop connections to existing learning and frameworks.
Students used performance phase strategies, especially elaborating and organizing, to further support integration of their existing content knowledge, or develop the foundational knowledge needed for future integration.
Diagnosing gaps in learners’ self-regulated learning process can facilitate a conversation which includes concrete suggestions for new strategies, tasks, and behaviors to improve future learning.
Introduction
During the last few decades, undergraduate medical education (UME) curricula have shifted toward an educational model that focuses on integrating clinical and scientific knowledge from the start of medical school (Brauer and Ferguson Citation2015; Cooke et al. Citation2006). Integrated curriculum refers to any curriculum designed to help students understand the interaction between basic, clinical, and social sciences within a specific course. The move to integrated curricula is rooted in adult learning theory which suggests that students need to make meaningful connections with the material to learn it (Brauer and Ferguson Citation2015; Kaufman and Mann Citation2010). To support the shift in integrated content, many UME programs have also shifted to a student-centered approach (Ginzburg et al. Citation2019), requiring learners to actively participate in classes they have prepared for, rather than passively attending lectures (Cooke et al. Citation2006). Students spend significant time during the first year of medical school learning how to learn in this environment and when students are unable to transition efficiently, their academic performance suffers (White Citation2007). Educational research demonstrates that the effectiveness of any individual learning strategy changes based on the environment in which it is applied (Scouller Citation1998; Nijhuis et al. Citation2005).
This integrated, student-centered environment requires students to organize, prioritize and synthesize their learning in new ways that differ from many of their prior educational experiences.
Success in medical school requires students to become self-regulated learners. Self-regulated learning (SRL) is defined as a ‘proactive process that students use to acquire academic skills, such as setting goals, selecting and developing learning strategies, and self-monitoring one’s effectiveness (Zimmerman Citation2008). SRL describes the cognitive work students must do to engage in learning. Medical educators identify SRL as an important skill set for physicians in a career that requires life-long learning. SRL strategies need to be explicitly taught (Scouller Citation1998; Zimmerman Citation2008; White et al. Citation2013) and the specific SRL strategies used will vary based on the learning environment (Scouller Citation1998; Nijhuis et al. Citation2005)
The majority of research in medical education on SRL has examined the relationship between SRL strategies and student learning within either a basic science (West and Sadoski Citation2011), or clinical context (Cho et al. Citation2017). For example, by examining first-year medical students’ SRL strategies in an anatomy class, one study found that three SRL strategies (i.e. elaboration, critical thinking, and effort regulation) were significantly associated with students’ class performance (Pizzimenti and Axelson Citation2015). A review of studies that examined SRL during the clerkship years suggests that SRL is associated with students’ academic achievement and clinical skills (Cho et al. Citation2017). Another systematic review in the clerkship years found that individual, contextual, and social factors had a significant impact on SRL strategies (van Houten‐Schat et al. Citation2018). These studies took place in traditional learning environments. Few studies have examined SRL strategy use in an integrated, student-centered context. One such study (Zheng and Zhang Citation2020), found that peer learning and help seeking were significantly associated with UME students scaled Comprehensive Basic Science Exam (CBSE) scores in an integrated, flipped classroom learning environment. Another study (Zheng et al. Citation2020), found that students in an integrated curriculum were more likely to use forethought and self-reflection strategies than performance strategies. However, neither study explored the specific tasks and behaviors students employed while engaged in self-regulated learning in this context.
Little work has been done to examine exactly what learning strategies students use (tasks), and how they use them (behaviors), during their first year in an integrated, student-centered medical school curriculum. This information is often sought by students experiencing difficulty with the transition to medical school as well as the educators seeking to support them. This study, therefore, focuses on exploring the following research question: What SRL strategies do students use during their first year of an integrated student-centered medical school curriculum, and how do students use these strategies?
Approach
Context
This study takes place on two medical school campuses, School 1 and School 2. School 1 is a community medical school affiliated with a midwestern land grant university, which implemented a competency-based, integrated, student-centered curriculum in the fall of 2016. At School 1, during the first two years of medical school, students are given weekly objectives and significant preparatory material. Students must then use the weekly learning activities/experiences and preparatory material to learn the objectives. Throughout the week students work in small groups of 8 students to apply and extend their knowledge using a case-based structure. Students also have a four-hour interactive large group didactic session designed to support them in integrating basic, clinical and social sciences. Students attend histology, simulation, and anatomy labs as well as clinic each week to further support learning the weekly objectives. School 2, located on the east coast of the US, is a young medical school that graduated its first class in 2015. School 2 was designed with an integrated, student-centered curriculum at its inception (Ginzburg et al. Citation2015). A majority of curriculum time in the Year 1 (MS1) and Year 2 (MS2) years consists of small group sessions where students are responsible for creating their learning objectives for the week, doing independent research to learn these topics, and working in groups of 8–9 students to apply this knowledge to patient-based cases. Students also attend didactic sessions, participate in clinical learning and communication session, and have weekly rotations in clinical offices to support their learning.
These medical schools were deemed viable sites for co-study because they share similar curricular pedagogy, which asks students to engage in similar cognitive processes. Both School 1 and School 2 use fully integrated curricula, in which students learn basic, clinical, and social sciences woven together, and spiraled over time, rather than traditional basic science classes in the first two years of medical school. Both schools also have student-centered curricula, characterized by sessions that require students to: research learning objectives and figure out what they know and don’t know prior to attending class, identify and extract information from primary resources, engage in activities during class that scaffold complex reasoning, spend the majority of the week in self-directed learning by limiting class contact hours. At both schools, students spend much of their first year developing new learning strategies to support SRL in order to meet the demands of their respective curricula. These similarities allowed the researchers to explore trends in first-year students’ SRL strategy development in integrated, learner-centered curricula.
Student interviews
The interview questions were developed by the authors in an iterative process (see Supplemental Digital Appendix 1) and focused on learning strategies used just prior to starting medical school and at the end of the first year. In particular, students were asked 1) how they planned for an upcoming week; 2) what strategies they used while studying; 3) how they assessed or reflected on their learning; and 4) what ways they changed or adapted their learning process.
At each site, an email was sent out to all first-year medical students inviting them to participate in an interview as part of a research study to understand the learning strategies they used during their first year of medical school (convenience sampling). While convience sampling was used, the sample contained both gender and academic diversity. Slightly more than half the students interviewed identified as women, and students from all academic categories (higher, lower and average performance) were represented. The structured interviews were administered in person by a co-author at their respective site (School 1: BZ & AW; School 2: ES & AC). Interviews took place between April - May 2019 and lasted approximately 30 to 45 min. All interviews were audio recorded and transcribed verbatim. Transcriptions and codes were managed in Microsoft Excel® (Microsoft Corporation, Redmond, WA, USA).
School one conducted twelve interviews (out of 180 MS1 students), while school two conducted thirteen (out of 100 MS1 students). Students who participated in the interview were offered a monetary incentive in the form of a gift card. All students who participated in this study successfully completed their first year of medical school and went on to begin the second year of medical school on time. During the in-depth, semi-structured interviews students were asked to reflect on their learning strategies both retrospectively (at the start of medical school) and at the time of the interview (toward the end of the MS1 year) with the goal of understanding how students successfully enacted their learning strategies.
Data analysis
For qualitative analysis, we used prominent SRL theories as a conceptual framework from which to initially approach the coding of the data. Zimmerman (Citation2002) proposed three phases of SRL: forethought, performance, and self-reflection. The forethought stage usually involves goal setting and strategic planning. During the performance stage, a self-regulated learner implements selected strategies and self-monitors their own learning process. The self-reflection stage involves not only students self-assessing their performance, but also planning adjustments for future learning. Pintrich built on Zimmerman’s work and developed and validated the Motivated Strategies for Learning Questionnaire (Pintrich et al. Citation1991), which asked students about specific strategy use, to understand exactly which strategies college students were using under which circumstances.
Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) and Google Docs (Alphabet Inc., Mountain View, CA, USA) were used to manage the transcribed interviews and codes. Responses from each phase (forethought, reflection, and performance) were analyzed separately using both Zimmerman (Citation2002) and Pintrich’s (Pintrich et al. Citation1991) models as a conceptual framework for the coding. Researchers then chose codes from both models as warranted by the data to code the data deductively. The CHM research team (AW & BZ) generated the preliminary codebook. Codes for the forethought phase (e.g. goal setting and strategic planning) and the reflection phase (e.g. self-evaluation, course-evaluation, and co-reflection) were derived from Zimmerman’s SRL model (Zimmerman Citation1986; Citation2002) and the codes for the performance phase were derived from Pintrich’s MSLQ (Pintrich et al. Citation1991; e.g. rehearsal, elaborating, organizing, resource management, peer learning). Since one of the assumptions of the research is that first year medical students in an integrated, student-centered curriculum may enact SRL strategies differently than other students, we also left open the possibility that inductive codes might emerge. When codes outside of the frameworks were identified, the researchers documented and discussed them in depth before adding them to the codebook. Units of analysis were typically the length of a partial or complete sentence.
Researchers from both schools met through Zoom video conferencing (Zoom Video Communications, San Jose, CA, USA) to review the preliminary codebook. Once the initial codebook was agreed upon, one researcher from each school completed the coding for the transcripts from their institution (AW at CHM and DO at ZSOM) and one researcher coded all transcripts from both institutions (SG). Once the double coding was complete, the data were compiled and contrasted to determine if the codes and their application to the text were similar between coders. Then all three coders met through Zoom numerous times to discuss and reconcile the coded data. In cases where there was disagreement, the third coder reviewed the discrepancy which was discussed with all coders until reaching a negotiated agreement. Through extensive meetings, the coders reviewed the coded data and further refined and named sub-codes in the data using an inductive approach to make sense of the tasks and behaviors students were describing. These sub-codes were labeled as tasks and behaviors. through present these codes, tasks and behaviors.
Table 1. Explanation of how first-year medical students engage the FORETHOUGHT PHASE of SRL in an integrated, learner-centered curricula.
Table 3. Explanation of how first-year medical students engage the SELF-REFLECTION PHASE of SRL in an integrated, learner-centered curricula.
Findings
The goal of this research is to support students by providing a clear understanding of the strategies that first year medical students use during the three phases of SRL in an integrated, student-centered curriculum. Therefore, we present the findings largely in an easily digestible table format that will allow readers to quickly understand and apply the strategies. For each phase of SRL our table reports the codes we identified in the data. For each code we identified tasks, which define what the student is trying to accomplish, behaviors, which describe what the student actually does, and examples to illustrate the tasks and behaviors in action. , represents a broad overview of the findings in each phase.
Figure 1. Representation of the broad findings within each phase of SRL.
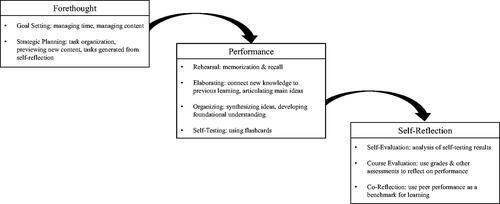
Forethought phase
Goal setting
Students engaged in two types of goal setting tasks: managing time and managing content. Behaviors focused on managing time included creating schedules and checklists to determine when to focus on specific content. Many medical students described elaborate systems for managing time including use of calendars, checklists, timers, etc. Students also described managing content by reviewing previous learning in order to understand what new learning needs to take place. They also organized where the content would go in their notes by integrating learning objectives and concepts to create a framework for learning for the week ahead.
Strategic planning
Students identified three types of strategic planning tasks: task organization, previewing new content, and tasks generated from self-reflection. When organizing tasks, students described breaking large tasks, which integrated multiple aspects of learning, into component parts. There, students described taking previously integrated learning objectives and dividing them into snapshots of material to be learned, before re-integration could occur. The second learning task under strategic planning is previewing content. Students described previewing content to develop background knowledge needed to learn foundational material. As students developed their background knowledge, they described actively building frameworks to support learning the new information. Finally, some students engaged in self-reflection by planning to target specific learning gaps or generating questions to ask in office hours.
Performance phase
Rehearsal
Students described rehearsal largely as a way to support direct memorization and recall, rather than to support student’s understanding of the material. Students reported using spaced repetition as part of their rehearsal strategies as well.
Elaboration
Students identified two types of elaboration tasks: connecting to prior knowledge and connecting to main ideas. Students reported creating diagrams and pictures to integrate content while learning or putting text into their own words in order to better understand the content.
Organization
Two kinds of organizing tasks were described by students: synthesizing ideas and developing foundational knowledge. These tasks were often done in tandem, where students would first work to understand the main ideas from a text, and then look across resources to add depth to their learning and connect to other ideas. They reported outlining materials or drawing diagrams or tables throughout this process.
Self-testing
Self-testing tasks were described as used for the purpose of developing recall. Students frequently used self-testing in conjunction with rehearsal to learn material that needed to be memorized.
Self-Reflection phase
Self-evaluation
Self-evaluation behaviors identified by students included using flashcards and other resources to self-test. Many students also described using board style question banks to assess their knowledge.
Course-evaluation
Students described using course grades and summative/formative evaluation to reflect on performance and make changes to study habits as needed.
Co-reflection
Students described two learning tasks for co-reflection: peer preparation benchmarking and peer reflection. Some students described using peers not as a benchmark but as an aid in self-assessment, by creating study groups or other circumstances where students could quiz each other and talk through ideas. Others engaged in benchmarking behaviors such as listening to peers during classes or office hours to see if their knowledge was on par.
Insight
Zimmerman and Pintrich provided the foundational framework for SRL utilized in this study. However, an important limitation of their work is that it does not offer direct instruction on the tasks and behaviors needed to enact the construct. The results of the current study build upon existing knowledge by providing a more detailed understanding of the specific strategies, tasks, and behaviors medical students use to support SRL as they engage in integrated, student-centered curricula during their first year of medical school.
Forethought phase
Overall, students described shifting their forethought behaviors to better plan for the integration of material, and to develop connections to existing learning and frameworks. These findings align with prior research about learning which states that learning complex, integrated material must involve building frameworks that incorporate learners’ prior schema, and then adding details to those frameworks (Brown et al. Citation2014; Ambrose et al. Citation2010). However, traditionally, according to SRL theory, the forethought phase is associated primarily with skills involving time management and resource management (Schunk Citation2005; West and Sadoski Citation2011). The present study expands this finding by showing that these first-year students utilized forethought not simply to decide what work to accomplish at a given time, but also to plan for integration. Students engaged in the behaviors of consolidating new information with old, integrating multiple learning objectives, identifying the scope and boundaries of a task, and breaking a task into its components. Each of these behaviors set students up to build frameworks and explore the boundaries of ideas, in other words, to integrate.
Performance phase
Students used performance phase strategies, especially elaborating and organizing, to either support integration of their existing content knowledge, or develop the foundational knowledge needed for future integration. Bloom’s revised taxonomy (Krathwohl Citation2002) holds that learning happens in a progression, and before complex processes like integration can occur, students must build up their initial knowledge base. This study supports that assumption by demonstrating the ways students fluidly move between initial content learning and more complex integration. For example, during the performance phase students engaged in low level Bloom’s behaviors such as paraphrasing, outlining and rehearsal to strategies that promote more complex learning like generative notetaking, and clustering of ideas (see for examples).
Table 2. Explanation of how first-year medical students engage the PERFORMANCE PHASE of SRL in an integrated, learner-centered curricula.
Interestingly, a few strategies traditionally associated with the performance phase (Zimmerman Citation1986) were used instead during other phases of SRL. These included resource management, peer learning and identifying knowledge gaps. Students described resource management during the forethought rather than performance phase. As students engaged in defining what they needed to learn, they decided which resources would help them with that learning. In the context of an integrated student-centered curriculum this makes sense, because students are not always assigned resources, and instead must work from a list of suggested resources and decide which to use. Students in our contexts needed to do that work as part of forethought, to prepare for the learning that would happen in the performance phase. Peer learning and identifying knowledge gaps, however, tended to occur not as a way to learn material as it often occurs in secondary education, but instead in the reflection phase. We suggest that this shift may be in part due to students engaging in peer learning and identifying knowledge gaps in conjunction with assessment. For example, as shown in , students often quiz themselves or work with a peer to quiz each other to determine what they need to know next. They rarely described utilizing this type of quizzing behavior as they read a text or watched a video.
Self-reflection phase
While students in an integrated, student-centered curriculum used their forethought and goal-setting strategies in ways that highlighted new and different learning goals based on their context, students in this study tended to use strategies during the self-reflection phase in ways traditionally associated with the self-reflection phase of SRL. Self-reflection is typically used to help students decide what they already know and what they need to learn next. In this study, while the purpose of reflection remained the same, we noticed that students engaged in this process using three specific forms of reflection - self-reflection, course evaluation and co-reflection.
Implications for strategy use
Our data provides a roadmap for students, faculty, learning specialists, and staff to use to support students as they become self-regulated learners. The specific strategies, tasks, and behaviors described provide a bridge between theory and the specific steps students take to engage in SRL. Although students may hear about the phases of SRL in medical school, they often have difficulty translating each phase into actionable steps as first year medical students. The specific information provided by this study can aid in diagnosing gaps in learners’ existing processes or serve as concrete suggestions for new strategies, tasks, and behaviors to try when coaching first year medical students. Additionally, as faculty orient students to the new learning environment, they can be deliberate in describing the phases of SRL and providing specific examples of strategies, tasks, and behaviors students should consider emphasizing in an integrated, student-centered curriculum.
Limitations and future directions
This study is not without limitations. We used convenience sampling to recruit participants, which may result in a biased sample, however as a qualitative study the goal is to understand the experiences of these students in this context, with the hope that the results will resonate with others in similar contexts. Future studies could utilize purposive sampling, with the goal of building a more quantitive understanding of student experiences.
Because this study used self-report data, students may have internalized certain strategies and not thought of them as strategies to report. Thus, further studies could use event measures of SRL such as think-aloud or real-time observation of student learning (Moos and Bonde Citation2016; Gandomkar et al. Citation2016) to more accurately capture students’ adoption of SRL strategies. It would also be beneficial to query students at the beginning and end of the first year of medical school to more accurately capture frequency of use, and when and how the behaviors are applied, rather than rely only on student recall during interviews. Finally, future studies could examine links between strategy use and achievement, as well as how students respond to interventions that support use of these strategies.
Conclusion
Our study provides new insights into which strategies medical students utilize to support SRL in an integrated, student-centered curriculum. Additionally, this study provides a detailed understanding of the tasks and behaviors students engage in to employ these strategies. The results of this study are a tangible resource that educators can utilize to support students during the first year medical school.
Disclaimer
The opinions and assertions expressed herein are those of the authors and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences or the Department of Defense.
Supplemental Material
Download MS Word (15.6 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Amy Greenberg
Amy Greenberg, MEd, is the Interim Director of Clinical Experiences at Michigan State University. Greenberg’s work in medical education is focused on the nexus of teaching and learning. She explores how preceptors, curriculum, and cultural forces promote metacognition and learning in students. In addition to engage in medical education research, she works directly with faculty on teaching and learning projects that focus on teacher effectiveness.
Doreen M. Olvet
Judith Brenner, MD, is an associate professor and the Senior Associate Dean for Medical Education at the New York University Long Island School of Medicine. Dr. Brenner’s research interests have been focused on assessment in undergraduate medical education, specifically use of open-ended questions for assessment of medical knowledge, and use of the medical student performance evaluation. In addition, Dr. Brenner works with faculty, staff and trainees across the undergraduate/graduate medical education continuum to promote trainee growth and success.
Judith Brenner
Doreen M. Olvet, PhD, is an Associate Professor of Science Education and the Director of Science Education Scholarship at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell. Dr. Olvet has published on the use of open-ended questions in medical school assessment as well as the use of near-peers as teachers. Her role is to coach faculty on medical education scholarly projects and teach medical students clinical epidemiology and biostatistics.
Binbin Zheng
Elisabeth F. M. Schlegel, PhD, MSc, MBA, MS (HPPL), is Professor, Microbiology and Immunology, in the Department of Medical Education at the Western Atlantic University School of Medicine. Drawing from backgrounds of science, business, and pedagogy, her interest includes developing, assessing, and disseminating learner-centered, collaborative teaching and learning frameworks and methodologies in the foundational sciences as well as in health professions education.
Amber Chess
Amber Chess, is the Deputy Director of the Office of Student Disability Services at the University of Chicago. Prior to her current role, she worked as a Medical Education Learning Specialist for nearly a decade, where she assisted students in optimizing the use of metacognitive strategies during their medical education experience. Her Interests include support of students underrepresented in higher education.
Elisabeth F. M. Schlegel
Samara B. Ginzburg, MD, is the Vice Dean and Dean for Education at the Zucker School of Medicine. Dr. Ginzburg’s research interests focus on innovations in medical education in learner-centered curricula. Her team received the NEGEA Innovation in Medical Education Award for developing a longitudinal, integrated approach to leadership training in medical education as part of a problem/case-based learning program and she is currently PI on two education innovation grants-AMA Accelerating Change in Medical Education-Coaching the Master Adaptive Learner and an AAMC/CDC Health Professions Education Curricular Innovations Grant: Kickstarting Strategies for Addressing Health Misinformation.
Samara B. Ginzburg
Binbin Zheng, PhD, is an associate professor in the Center for Health Professions Education (CHPE) at the Uniformed Services University of the Health Sciences (USUHS). She brings her background in educational technology and educational psychology into the field of health professions education. Her current research focuses on using technologies to support teaching and learning, knowledge construction and group dynamics in collaborative learning environments, self-regulation and co-regulation, and interprofessional education.
References
- Ambrose SA, Bridges MW, DiPietro M, Lovett MC, Norman MK. 2010. How learning works: seven research-based principles for smart teaching. San Francisco (CA): Jossey-Bass (John Wiley & Sons).
- Brauer DG, Ferguson KJ. 2015. The integrated curriculum in medical education: AMEE Guide No. 96. Med Teach. 37(4):312–322.
- Brown PC, Roediger HL, McDaniel MA. 2014. Make it stick. London (UK): Belknap Press (Harvard University Press).
- Cho KK, Marjadi B, Langendyk V, Hu W. 2017. The self-regulated learning of medical students in the clinical environment – a scoping review. BMC Med Educ. 17(1):17.
- Cooke M, Irby DM, Sullivan W, Ludmerer KM. 2006. American Medical Education 100 Years after the Flexner Report. Cox M, Irby DM, eds. N Engl J Med. 355(13):1339–1344.
- Gandomkar R, Mirzazadeh A, Jalili M, Yazdani K, Fata L, Sandars J. 2016. Self-regulated learning processes of medical students during an academic learning task. Med Educ. 50(10):1065–1074.
- Ginzburg S, Brenner J, Willey J. 2015. Integration: a Strategy for Turning Knowledge into Action. MedSciEduc. 25(4):533–543.
- Ginzburg SB, Willey JM, Bates C, Santen SA, Battinelli D, Smith L. 2019. Applying the Hedgehog Concept to Transform Undergraduate Medical Education. Acad Med. 94(4):477–481.
- Kaufman DM, Mann KV. 2010. Teaching and learning in medical education: how theory can inform practice. In Understanding medical education: evidence, theory and practice. Hoboken (NJ): Wiley-Blackwell; p. 7–30.
- Krathwohl DR. 2002. A revision of Bloom’s taxonomy: an overview. Theory Prac. 41(4):212–218.
- Moos DC, Bonde C. 2016. Flipping the Classroom: embedding Self-Regulated Learning Prompts in Videos. Tech Know Learn. 21(2):225–242.
- Nijhuis JFH, Segers MSR, Gijselaers WH. 2005. Influence of Redesigning a Learning Environment on Student Perceptions and Learning Strategies. Learning Environ Res. 8(1):67–93.
- Pintrich PR, Smith DA, Garcia T, McKeachie WJ. 1991. A Manual for the Use of the Motivated Strategies for Learning Questionnaire (MSLQ). National center for research to improve postsecondary teaching and learning.
- Pizzimenti MA., Axelson RD. 2015. Assessing student engagement and self‐regulated learning in a medical gross anatomy course. Anat Sci Educ. 8:104–110.
- Schunk DH. 2005. Self-Regulated Learning: the Educational Legacy of Paul R. Pintrich. Educ Psycholog. 40(2):85–94.
- Scouller K. 1998. The influence of assessment method on students’ learning approaches: multiple choice question examination versus assignment essay. Higher Educ. 35(4):453–472.
- van Houten‐Schat MA, Berkhout JJ, Van Dijk N, Endedijk MD, Jaarsma ADC, Diemers AD. 2018. Self‐regulated learning in the clinical context: a systematic review. Med Educ. 52(10):1008–1015.
- West C, Sadoski M. 2011. Do study strategies predict academic performance in medical school? Med Educ. 45(7):696–703.
- White CB. 2007. Smoothing Out Transitions: how Pedagogy Influences Medical Students’ Achievement of Self-regulated Learning Goals. Adv Health Sci Educ Theory Pract. 12(3):279–297.
- White CB, Gruppen LD, Fantone JC. 2013. Self-regulated learning in medical education. In: Tim S, editor. Understanding medical education. John Wiley & Sons, Ltd; p. 201–211.
- Zheng B, Ward A, Stanulis R. 2020. Self-regulated learning in a competency-based and flipped learning environment: learning strategies across achievement levels and years. Med Educ Online. 25(1):1686949.
- Zheng B, Zhang Y. 2020. Self-regulated learning: the effect on medical student learning outcomes in a flipped classroom environment. BMC Med Educ. 20(1):100.
- Zimmerman BJ. 2008. Investigating Self-Regulation and Motivation: historical Background, Methodological Developments, and Future Prospects. Am Educ Res J. 45(1):166–183.
- Zimmerman BJ. 1986. Becoming a self-regulated learner: which are the key subprocesses? Contemp Educ Psychol. 11(4):307–313.
- Zimmerman BJ. 2002. Becoming a Self-Regulated Learner: An Overview. Theory Prac. 41(2):64–70.