

Abstract
Background
The trend of increasing caesarean section (CS) rates brings up questions related to subfertility. Research regarding the influence of CS on assisted reproduction techniques (ART) is conflicting. A potential mechanism behind CS-induced subfertility is intra uterine fluid resulting from a caesarean scar defect or niche. The vaginal microbiome has been repeatedly connected to negative ART outcomes, but it is unknown if the microbiome is changed in relation to a niche.
Methods
This systematic review describes literature investigating the effect of a niche on live birth rates after assisted reproduction. Furthermore, studies investigating a difference in microbial composition in subfertile persons with a niche compared to no niche are evaluated. Pubmed, Embase and Web of Science were searched on March 2023 for comparative studies on both study questions. Inclusion criteria were i.e., English language, human-only studies, availability of the full article and presence of comparative pregnancy data on a niche. The quality of the included studies and their risk of bias were assessed using the Newcastle-Ottawa scale for cohort studies. The results were graphically displayed in a forest plot.
Results
Six retrospective cohort studies could be included on fertility outcomes, with a total of 1083 persons with a niche and 3987 without a niche. The overall direction of effect shows a negative impact of a niche on the live birth rate (pooled aOR 0.58, 95% CI 0.48-0.69) with low-grade evidence. Three studies comparing the microbiome between persons with and without a CS could be identified.
Conclusion
There is low-grade evidence to conclude that the presence of a niche reduces live birth rates when compared to persons without a niche. The theory that a caesarean has a negative impact on pregnancy outcomes because of dysbiosis promoted by the niche is interesting, but there is no sufficient literature about this.
PLAIN LANGUAGE SUMMARY
The increasing number of caesarean deliveries has raised concerns about how it might affect a woman’s ability to get pregnant afterwards. Some studies suggest that having a caesarean section (CS) could make it harder to conceive, particularly through in vitro fertilisation (IVF). The reason could be the scar or niche from a previous caesarean. This niche can cause fluid inside the uterus. We also know that the mix of bacteria in the vagina, called the vaginal microbiome, can affect a woman’s chances of getting pregnant, especially with treatments like IVF. But we are not sure if having a caesarean affects the vaginal microbiome.
To understand this better, van den Tweel’s team looked at studies on whether having a niche from a caesarean affects a woman’s chance of having a baby through IVF. They also looked at studies comparing the bacteria in the vagina of women who have had a caesarean with those who have not. They found that having a caesarean niche makes it harder for a woman to have a baby through IVF. However, the evidence from these studies is not very strong. We still do not know enough about whether having a caesarean niche affects the bacteria in the vagina.
Introduction
The global average caesarean section (CS) rate increased by 19 percent from 1990 to 2018, with the WHO projecting continued growth up to 2030 (Betran et al. Citation2021).
The trend of increasing CS rates brings up questions related to its sequelae, amongst others, subfertility. Two systematic reviews, including meta-analysis, reported that persons post-CS take longer to achieve a subsequent pregnancy compared to vaginal delivery, with lower live birth rates (LBR), and are at a 14% increased risk of subfertility (O’Neill et al. Citation2013) (Gurol-Urganci et al. Citation2013). Both authors advise cautious interpretation of these results due to large heterogeneity in methodology and study quality, as well as unknown factors that play a role in the decision to perform a CS, such as couple’s personal views, expectations and experiences. These reviews, in tandem with an expected 28.5% share of CS in global births by 2030, indicate a concerning trend in reproductive health (Betran et al. Citation2021).
Research regarding the influence of CS on assisted reproduction techniques (ART) is conflicting. Two recent reviews investigate the impact of a CS in ART, yielding contradictory results on pregnancy rates (Riemma et al. Citation2021; Zhao et al. Citation2021) Several potential mechanisms behind a CS-induced reduction in fertility have been proposed. Principal amongst them is the presence of pelvic adhesions post-CS, disturbed foetal implantation, and the presence of a caesarean section defect or niche (Gurol-Urganci et al. Citation2013; Jolijn Vissers et al. Citation2020) The presence of a niche facilitates intra-uterine fluid and mucus accumulation, promotes local inflammation, disturbs physiological uterine contractions, and may hamper oocyte pick-up and embryo transfer during ART. The accumulation of blood in the niche could lead to degradation of haemoglobin and result in higher iron exposure, which could promote certain bacteria (Jolijn Vissers et al. Citation2020) A systematic review found the prevalence of a transvaginal ultrasound ascertained niche to be 24%-70% in persons with a history of CS (Bij de Vaate et al. Citation2014) Studies show that delivery via CS substantially raises the risk of a repeat CS (Sharma et al. Citation2020) With each consecutive CS the risk of incomplete scar healing and niche rises, up to 45-100% after a third CS (Bij de Vaate et al. Citation2014; Vikhareva Osser et al. Citation2009) Recently, a panel of experts defined the symptoms arising from a niche, an endometrial indentation at the site of a CS with a depth of at least 2 mm determined by ultrasound, as a Caesarean Scar Disorder (Jordans et al. Citation2019; Klein Meuleman et al. Citation2023).
The vaginal microbiome has been repeatedly connected to negative ART outcomes (Koedooder et al. Citation2019; Moreno et al. Citation2022; Skafte-holm et al. Citation2021) The sterile uterus hypothesis is now largely rejected but precise knowledge of what constitutes a physiologic uterine microbiome is lacking. Consensus has been achieved that the vaginal and endometrial microbiome form a continuum (Chen et al. Citation2017) Furthermore, there is early evidence that the presence of not only Lactobacillus in the vagina but also in the endometrium influences live birth rates (Koedooder et al. Citation2019; Moreno et al. Citation2022)
These studies raise the question if the reason for secondary subfertility after a CS is specifically caused by a niche. And if so, maybe the mucus accumulation in the niche could promote an abnormal microbiome. In this systematic review we evaluate the current studies about fertility outcomes during assisted reproduction techniques (ART) in the context of a niche, as well as the microbial composition following CS.
Methods
Data sources and main outcomes
This systematic review was conducted following the PRISMA Guidelines. This review was not registered upfront in a database, and had no protocol published. Ethical approval was not applicable. The PICO of the first study question was whether persons undergoing ART with a caesarean have different pregnancy outcomes compared to persons undergoing ART without a caesarean (or a niche). Pubmed, Embase and Web of Science were searched in November 2022 for articles using the keywords “caesarean” and “embryo transfer” to identify all relevant articles on the niche fertility search. Two authors (SvdS;MvdT) reviewed independently the title and abstract of each article for relevancy. In some cases, full text documents were also reviewed to make the final decision. In cases of a disagreement, a third person was responsible for making the final decision (KB). Inclusion criteria were English language, human-only studies, availability of the full article and presence of comparative pregnancy data on a niche. Exclusion criteria were conference abstracts, questionnaires, and reviews.
The main outcome for this review was live birth, secondary outcomes were clinical pregnancy, ectopic pregnancy, miscarriage, multiple pregnancy rate and ongoing pregnancy rate. Included articles were searched independently for data by two authors (SvdS; MvdT) on description of the niche, patient characteristics such as infertility duration, number of deliveries, intervention characteristics such as in vitro fertilisation (IVF) procedure, fresh/frozen embryo transfer, single or double embryo transfer (SET or DET) and statistical analysis.
The PICO of the second study question was whether subfertile persons with a caesarean have a different microbiome compared to subfertile persons without a caesarean (or niche). A second search using the keywords “bacteria”, “caesarean” and “fertility” was used to identify articles regarding microbial composition of a niche in March 2023. Further papers were identified via the snowballing method, using the reference lists of included papers as a starting point. Again two separate authors (SvdS;MvdT) reviewed independently the title and abstract of each article for relevancy. The authors were able to reach consensus in all cases. Inclusion criteria were English language, human-only studies, availability of the full article and presence of data on caesarean delivery. Exclusion criteria were conference abstracts and reviews.
Most important outcome for this part of the review was microbial composition. Secondary outcomes were pregnancy rates. Included articles were sought for a description of the niche, patient characteristics such as subfertility duration, number of deliveries, method of obtaining cervical or endometrial microbial samples and microbial analysis.
Full search strings of both searches are provided in Appendix 1.
Data collection and analysis
The quality of the included studies and their risk of bias were assessed using the Newcastle-Ottawa scale (NOS) for cohort studies. The NOS scores the studies on three categories: the selection and comparability of the exposed and non-exposed, and the ascertainment of outcome. With a maximum score of 9, one point can be awarded per subheading of the selection and outcome categories, with comparability being worth up to two points. Two authors scored the articles independently (SvdS; MvdT), when there was a disagreement, a third person determined the final score (KB).
The extraction forms were explicitly designed for this systematic review (see Appendix 4).
Odds ratios (OR) with 95% CI were extracted from the papers or calculated from the reported results in the papers. The results were graphically displayed in a forest plot. If heterogeneity between studies was low, odds ratios would be formally pooled in a random effect meta-analysis. Publication bias was assessed when a review contained more than 10 studies. R 4.3.1 was used to make the forest plot and meta-analysis.
Quality of obtained evidence is scored by Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system.
Results
General characteristics
A flowchart detailing the screening process of the two searches can be seen in . The niche fertility search identified 323 search results. Title and abstract screening identified 41 studies, and after screening the full article, six studies were included with complete (statistical) data about the niche and ART outcomes (Asoglu et al. Citation2021; Diao et al. Citation2021; Friedenthal et al. Citation2021; Huang et al. Citation2022; Wang et al. Citation2022; Zhang et al. Citation2022) The article by Vissers et al. which only mentioned an effect of a niche in their discussion, was excluded because of incomplete data (J Vissers et al. Citation2020) The study of Lawrenz et al. was excluded because of incomplete data and insufficient details in statistical analysis (only p-values of chi-square and t-test, no data on odds ratios) (Lawrenz et al. Citation2020) Of the included six papers, four were published after the most recent reviews by Riemma and Zhao et al. (Riemma et al. Citation2021; Zhao et al. Citation2021) All studies were retrospective cohort studies. In all six studies only the first cycle of an ART (IVF or intracytoplasmic sperm injection (ICSI)) regimen was analysed. All studies reported on live birth rates (LBR). In total 1083 patients with a niche were analysed.
Figure 1. Flow chart of included studies.
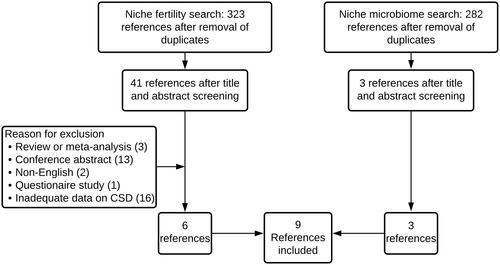
In the niche microbiome search, 282 papers were identified (). Three papers about the microbiome in the context of a niche were included after title and abstract screening (Hsu et al. Citation2022; Yang et al. Citation2022, Citation2021) Two studies were case-control studies that utilised cervical and endometrial 16s PCR sequencing (Yang et al. Citation2022, Citation2021) The other study was a prospective cohort study and utilised bacterial cultures of the niche and endocervix (Hsu et al. Citation2022) In total 138 participants with a niche were included.
Appendix 2 and 3 shows an overview of all articles screened.
Five studies received funding for their studies (Huang et al. Citation2022; Wang et al. Citation2022; Yang et al. Citation2022, Citation2021; Zhang et al. Citation2022) No study reported any conflict of interest. An overview of the included studies of both searches is shown in .
Table 1. Overview of included studies.
Overall quality assessment
Overall, the selected studies were heterogenous in their assessed susceptibility to bias. With exception of the study by Huang et al. (8 points) and Wang et al. (9 points), all the studies ranged from poor to medium in NOS scores. Wang et al. analysed only single embryo transfers (SET) and clearly described the methodology used, which resulted in the lowest assessed risk of bias of all studies (Wang et al. Citation2022) Because of the small number, the overall poor quality of the studies, and the heterogeneity in study population and niche evaluation, only a meta-analysis on the primary outcome of live birth was performed.
All three microbiome studies were scored as having poor quality (2 points for the studies of Yang and 4 points for the study of Hsu). The complete score table on the NOS is included in the Appendix 5. None of the microbiome studies provided any pregnancy outcomes after initial microbiome analysis was performed. Publication bias for both subjects was not assessed because of the low number of articles found.
Niche and pregnancy outcomes
Study population
All selected six studies included secondary infertile participants and analysed fertility outcomes during ART. Treatment strategies of ART were different between the studies. Two studies performed only SET (Friedenthal et al. Citation2021; Wang et al. Citation2022) Two studies had much higher proportions of double embryo transfer (DET) compared to others and did not provide reasons as to how SET or DET were assigned (Diao et al. Citation2021; Zhang et al. Citation2022) In the study of Diao et al. there was also a high percentage of selective reduction of twin pregnancies (Diao et al. Citation2021) One study only analysed fresh cycles (Diao et al. Citation2021) Two studies performed no fresh embryo transfer if any endometrial cavity fluid was seen (Friedenthal et al. Citation2021; Huang et al. Citation2022) Two studies only performed frozen embryo transfers (Friedenthal et al. Citation2021; Zhang et al. Citation2022) An overview of details of the studies is shown in . Furthermore, some studies only included pre-implantation genetic tested embryos for aneuploidy (Friedenthal et al. Citation2021), some had both PGTa and non PGTa (Asoglu et al. Citation2021), and some excluded those (Huang et al. Citation2022; Wang et al. Citation2022).
Niche evaluation
Three studies differed in their definition of a niche from that of the European niche taskforce (>2mm indentation) and two of them used subjective criteria (Asoglu et al. Citation2021; Diao et al. Citation2021; Friedenthal et al. Citation2021) All studies determined retrospectively whether there was a niche, using various methods to ascertain its presence. One study checked ultrasound pictures made during the day of oocyte retrieval (Huang et al. Citation2022), three studies checked multiple ultrasound pictures by two separate researchers (Friedenthal et al. Citation2021; Wang et al. Citation2022; Zhang et al. Citation2022).
Sample sizes
Three studies performed a power analysis before starting the study (Asoglu et al. Citation2021; Diao et al. Citation2021; Friedenthal et al. Citation2021). The other three studies had a high number of participants, with more than 120 having a niche, included (Huang et al. Citation2022; Wang et al. Citation2022; Zhang et al. Citation2022) Two out of six studies reached the number of included participants calculated in their power analysis (Asoglu et al. Citation2021; Friedenthal et al. Citation2021).
Comparability between studies
Three studies compared vaginal delivery with caesarean delivery as the main study question and conducted a subanalysis on participants with a niche (Diao et al. Citation2021; Friedenthal et al. Citation2021; Zhang et al. Citation2022) Two studies included persons with more than one delivery (Asoglu et al. Citation2021; Wang et al. Citation2022) Three studies had, as their main study question, the comparison between a niche and without a niche following a caesarean delivery (Asoglu et al. Citation2021; Huang et al. Citation2022; Wang et al. Citation2022) Baseline characteristics were in some studies significantly different (Diao et al. Citation2021; Friedenthal et al. Citation2021; Zhang et al. Citation2022), but these studies adjusted for the baseline differences in the final analysis. Asoglu et al. had an age-matched cohort but did not describe how these controls were chosen (Asoglu et al. Citation2021).
Multiple pregnancy rates differed in the studies, with the highest rates in the study of Diao et al. and Zhang et al. (23% and 28% in delivery control group). Diao et al. did not report any multiple pregnancies in the niche group. However, in two cases in the niche group, a selective embryo reduction was performed, compared to ten cases in the vaginal delivery control group.
Live birth
All six studies reported on live births and had adequate follow-up until birth. A forest plot for the odds ratios (OR) on the live birth rates (LBR) in those with and without a niche of all six studies is shown in and . All six studies found a negative effect on LBR, for 5 of the 6 studies the effect was statistically significant. One study observed no significant effect (Asoglu et al. Citation2021) The pooled adjusted OR was 0.58 (95% confidence interval: 0.48-0.69) (heterogeneity p = 0.61, I2 = 0%).
Figure 2. Live birth rate with a niche compared to no defect.
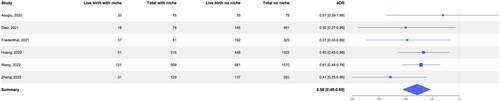
Table 2. Pregnancy outcomes for included studies.
Zhang et al. performed a separate analysis for the SET and DET group with an aOR of 0.59 (0.24-1.43) in the SET subgroup and aOR 0.39 (0.21-0.72) in the DET subgroup. Wang et al. found that the size of the niche had an effect on pregnancy outcomes: the larger the niche, the more pronounced the effect, leading to a greater odds ratio. Huang et al. found no significant effect in frozen cycles (aOR 0.69, 0.45-1.08), but a significant effect in fresh embryo transfers (aOR 0.5, 0.29- 0.87).
Intra cavitary fluid
Two studies performed a separate analysis to see if intracavitary fluid (ICF) was influencing pregnancy outcomes. In the study of Diao et al. the presence of ICF (n = 25) in relation to a niche did not significantly alter pregnancy outcomes (Diao et al. Citation2021) However, Huang et al. performed a comparison in the niche and frozen-thawed ET arm of the study between uterine cavity with (n = 35) and without ICF (n = 90) and showed a significantly lower LBR in the presence of ICF (aOR 0.27, 95% CI 0.08-0.94) (Huang et al. Citation2022).
Early pregnancy
Five studies reported clinical pregnancy rates. Odds ratios were in line with those of LBR (, ). Friedenthal et al. did not report clinical pregnancy rates, it was the only study reporting ongoing pregnancy rate, which was the same as LBR (Friedenthal et al. Citation2021) Four studies reported ectopic pregnancy rate, with in total 7 ectopic pregnancies in the niche group and 20 in the control group (Asoglu et al. Citation2021; Diao et al. Citation2021; Wang et al. Citation2022; Zhang et al. Citation2022).
Figure 3. Clinical pregnancy rate with a niche compared to no defect.

Five studies reported miscarriage rates. Only Wang et al. found a just significant higher miscarriage rate in persons with a niche, other studies did not find a significant difference. Numbers in all studies were small, in which Wang et al. had the largest numbers (, ).
Figure 4. Miscarriage rate with a niche compared to no defect.

Niche and microbiome
Two studies examined the microbiome in secondary infertile persons with a niche to those with vaginal delivery (Yang et al. Citation2022, Citation2021) One study analysed microbial composition in secondary infertile participants with a niche compared to participants with a caesarean without a niche (Hsu et al. Citation2022) No follow up was performed to see if participants conceived, hence no data about fertility rates could be extracted. None of the three studies performed any power analysis or sample size calculation.
Two out of three microbiome studies originated from the same research group, with both studies having different inclusion periods. Both studies lacked relevant data on the participants, such as infertility duration, socio-economic status, smoking, and comorbidities. No clear explanation was given how the control group was determined. In both studies there is no definition of a niche given (only described as seen at hysteroscopy). Samples were collected during hysteroscopy for cases with a niche and controls, and they were subsequently analysed using 16s rDNA sequencing. They found a decrease of Lactobacillus abundance in the cervix of CS participants, and an increase in the abundance of certain other bacteria (Proteobacteria, Neisseriaceae, Staphylococcaceae, Sphingomonas, Sediminbacterium, and Ralstonia) (Yang et al. Citation2022, Citation2021)
Hsu et al. had a more clearly defined prospective cohort (>1 year infertile) and definition of a niche (> 2,5mm indentation). However, this study also lacked relevant population-level data (such as socio-economic status, smoking, comorbidities etc.). Cultures were used to assess microbial composition. Samples were taken with ultrasound guidance during gynaecological examination with a speculum. More bacterial colonies (more Gram-positive cocci, Gram-negative rods (such as Pseudomonas)) were found in participants with a niche compared to those without a niche.
Discussion
There is low-grade evidence to conclude that the presence of a niche reduces the live birth rates during ART when compared to persons without a niche (). In the two studies with lowest risk of bias (Wang et al. and Huang et al.), the live birth rate was significantly lower in the niche group. There is insufficient literature on the topic of dysbiosis or intracavitary fluid promoted by the niche influencing ART outcomes.
Table 3. Concluding evidence of searches.
The previous general review by Riemma et al. did not reveal a lower live birth rate after a CS, possibly because the included studies did not account for the presence of a niche. Since then, more research has come to light reserving a role for the niche in fertility outcomes. One strength of this review is its focus on investigating the impact of the uterine niche, addressing the question of which individuals may experience difficulties conceiving after a caesarean section. We also broadened our scope to include intrauterine fluid and microbiome of individuals with a uterine niche. Additional prospective research is needed to investigate the effects of a niche to determine which persons with a CS may experience lower fertility rates, with a particular focus on intracavitary fluid.
A limitation of our review is the quality of evidence. The heterogeneity among the included studies was high. All studies on fertility outcomes were retrospective cohort studies, which may introduce bias. Preferably, results should be compared between participants with a niche and those with a CS without a niche, rather than comparing participants with a niche to vaginal delivery. The definition of a niche varied among studies, and this is important for comparing results. The definition of >2 mm indentation should be adhered to in future prospective studies. To reduce confounding, focus should also be on single embryo transfers (SET). Studies with a high proportion of DET resulted in a significant number of embryo reductions, which affects the live birth rates. A more complete description of patient characteristics is also essential for adjusting for confounding factors, such as smoking, socio-economic status, ethnicity, body mass index etcetera.
In addition to the heterogeneity of the studies, another limitation could be that the majority of the included studies were conducted in Asian countries. The microbiome is influenced, amongst other factors, by ethnicity, which makes extrapolating the results to another population difficult. Furthermore, the CS rate in China is high, at 35% (Li et al. Citation2020)This can also introduce bias when comparing our results to other countries with lower CS rates.
In future studies, the description of intracavitary fluid (ICF) should be included, as this could be the primary reason for a lower pregnancy rate. Several studies investigating ICF after CS have suggested that ICF might be the cause of low implantation rates, which is also suggested by the included study by Huang et al. It has been proposed that during frozen cycles, there is less ICF (Cai et al. Citation2022; Huang et al. Citation2022; Kathuria et al. Citation2024; Lawrenz et al. Citation2020) However, the smaller included study by Diao et al. did not find an impaired pregnancy rate in the presence of ICF (Diao et al. Citation2021) The findings so far are too heterogeneous to provide a clear answer regarding the separate impact of a niche compared to ICF.
Microbiome studies in the IVF population have shown a negative impact of the microbiome on fertility rates (Koedooder et al. Citation2019; Moreno et al. Citation2022) If a dysbiotic microbiome is more often encountered in persons with a niche, it could be the reason for lower fertility rates. This review demonstrates a similar association between bacterial counts, specifically lower Lactobacilli and an increase in other bacteria such as Pseudomonas and Streptococcus, as observed in studies about fertility and the microbiome. Therefore, this could be an important factor in understanding lower fertility rates after a CS (with a niche). The changed microbiome could also possibly be linked to the immune system, as the study by Nobuta et al. describes more chronic endometritis in persons with caesarean scar syndrome (Tsuji et al. Citation2022) Another theory could be that a dysbiotic microbiome (or the microbiome as a proxy for a certain lifestyle) influences the mode of delivery and the wound healing after a CS, increasing the risk of a niche. Future studies should be performed with high-quality design and preferably with objective testing methods for the vaginal or cervical microbiome, such as qPCR or 16s RNA sequencing. None of the included niche microbiome investigating studies reported fertility outcomes. However, this information is key for understanding the potential effects of the microbial environment on fertility and pregnancy outcomes.
Many questions will remain unanswered until further research is conducted. If the issue lies in the niche and the accumulated fluid, a niche repair (either laparoscopically or hysteroscopically) could potentially be beneficial (Abdou and Ammar, Citation2018) If the problem is related to an abnormal microbiome, antibiotics, probiotics or lifestyle interventions might prove successful. An interesting hypothesis is that flushing the niche or uterine cavity during hysterosalpingogram or hysteroscopy could lead to improved outcomes (Ghasemi et al. Citation2022) All treatments should only be offered within the context of a clinical trial to bring us closer to treating subfertility.
However, it is essential to bear in mind that if the first CS could be prevented through effective pre-labour counselling, subsequent pregnancies have fewer complications and lower maternal morbidity. Reducing the caesarean section rate may also contribute to preventing subfertility issues.
Conclusion
There is low-grade evidence to conclude that the presence of a niche reduces the live birth rates when compared to persons without a niche (). The overall direction of effect in all studies indicates a negative impact of a niche on the live birth rate (pooled aOR 0.58, 0.48-0.69). The theory that this could be attributed to dysbiosis or the intracavitary fluid promoted by the niche is interesting, but there is insufficient literature on this topic.
Author contributions
Authors roles: MvdT: conception and design of the study, acquisition, analysis and interpretation of data, review writing. SvdS: acquisition, analysis of the data, review writing SlC: interpretation of data, review editing KB: conception and design of the study, interpretation of data, review editing. All authors approved the version to be published and agreed to be accountable for all aspects of the work.
Supplemental Material
Download Zip (164.1 KB)Acknowledgements
We thank Prof. J.M.M. van Lith for critical appraisal of this review.
Disclosure statement
No funding was received for this review. The authors have stated explicitly that they have no conflict of interest in connection with this article.
Data availability statement
The dataset(s) supporting the conclusions of this article is(are) included within the article (and its additional file(s)).
Additional information
Funding
References
- Abdou, A.M. and Ammar, I.M.M., 2018. Middle East. Middle East Fertility Society Journal , 23 (4), 1–10.
- Asoglu, M.R., et al., 2021. Impact of Isthmocele on Assisted Reproductive Treatment Outcomes: An Age-matched Retrospective Study. Journal of Minimally Invasive Gynecology, 28 (5), 1113–1120.
- Betran, A.P., et al., 2021. Trends and projections of caesarean section rates: global and regional estimates. BMJ Global Health, 6 (6), e005671.
- Bij de Vaate, A.J.M., et al., 2014. Prevalence, potential risk factors for development and symptoms related to the presence of uterine niches following Cesarean section: systematic review. Ultrasound in Obstetrics & Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 43 (4), 372–382.
- Cai, M., et al., 2022. Intra-cavitary fluid resulted from caesarean section but not isthmocele compromised clinical pregnancy after IVF/ICSI treatment. Archives of Gynecology and Obstetrics, 306 (1), 229–237.
- Chen, C., et al., 2017. The microbiota continuum along the female reproductive tract and its relation to uterine-related diseases. Nature Communications, 8 (1), 875.
- Diao, J., et al., 2021. Caesarean section defects may affect pregnancy outcomes after in vitro fertilization-embryo transfer: a retrospective study. BMC Pregnancy and Childbirth, 21 (1), 487.
- Friedenthal, J., et al., 2021. The association between prior cesarean delivery and subsequent in vitro fertilization outcomes in women undergoing autologous, frozen-thawed single euploid embryo transfer, in: American Journal of Obstetrics and Gynecology. American Journal of Obstetrics and Gynecology, 225 (3), 287.e1-287–e8.
- Ghasemi, M., et al., 2022. Uterine Cavity Irrigation With Office Hysteroscopy During Ovarian Stimulation for IVF: A Randomized Controlled Trial. Frontiers in Endocrinology, 13, 778988.
- Gurol-Urganci, I., et al., 2013. Impact of Caesarean section on subsequent fertility: a systematic review and meta-analysis. Human Reproduction (Oxford, England), 28 (7), 1943–1952.
- Hsu, I., et al., 2022. Bacterial colonization at caesarean section defects in women of secondary infertility: an observational study. BMC Pregnancy and Childbirth, 22 (1), 135.
- Huang, L., et al., 2022. Reduced pregnancy and live birth rates after in vitro fertilization in women with cesarean section scar diverticulum: A retrospective cohort study. The Journal of Obstetrics and Gynaecology Research, 48 (1), 146–154.
- Jordans, I.P.M., et al., 2019. Sonographic examination of uterine niche in non-pregnant women: a modified Delphi procedure. Ultrasound in Obstetrics & Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 53 (1), 107–115.
- Kathuria, P., et al., 2024. Systematic review analyzing significance of endometrial cavity fluid during assisted reproductive techniques. Archives of Gynecology and Obstetrics, 309, 413–425.
- Klein Meuleman, S.J.M., et al., 2023. Definition and Criteria for Diagnosing Cesarean Scar Disorder. JAMA Network Open, 6 (3), e235321.
- Koedooder, R., et al., 2019. The vaginal microbiome as a predictor for outcome of in vitro fertilization with or without intracytoplasmic sperm injection: a prospective study. Human Reproduction (Oxford, England), 34 (6), 1042–1054.
- Lawrenz, B., et al., 2020. Isthmocele and ovarian stimulation for IVF: considerations for a reproductive medicine specialist. Human Reproduction (Oxford, England), 35 (1), 89–99.
- Li, H., et al., 2020. Trends in Cesarean Delivery Rates in China, 2008-2018. Jama, 323 (1), 89–91.
- Moreno, I., et al., 2022. Endometrial microbiota composition is associated with reproductive outcome in infertile patients. Microbiome, 10 (1), 1–17.
- O’Neill, S. M., et al., 2013. Caesarean Delivery and Subsequent Pregnancy Interval: A systematic review and meta-analysis. BMC Pregnancy Childbirth, 13, 165.
- Riemma, G., et al., 2021. Reproductive and pregnancy outcomes following embryo transfer in women with previous cesarean section: A systematic review and meta-analysis. Acta Obstetricia Et Gynecologica Scandinavica, 100 (11), 1949–1960.
- Sharma, J., et al., 2020. Prevalence of Repeat Cesarean Section in a Tertiary Care Hospital. Journal of Nepal Medical Association, 58 (229), 650–653.
- Skafte-holm, A., et al., 2021. The Association between Vaginal Dysbiosis and Reproductive Outcomes in Sub-Fertile Women Undergoing IVF-Treatment: A Systematic PRISMA Review and Meta-Analysis. Pathogens (Basel, Switzerland), 10 (3), 295.
- Tsuji, S., et al., 2022. Decreased Fertility in Women with Cesarean Scar Syndrome Is Associated with Chronic Inflammation in the Uterine Cavity. The Tohoku Journal of Experimental Medicine, 258 (3), 237–242.
- Vikhareva Osser, O., Jokubkiene, L. and Valentin, L., 2009. High prevalence of defects in Cesarean section scars at transvaginal ultrasound examination. Ultrasound in Obstetrics & Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 34 (1), 90–97.
- Vissers, J., et al., 2020. Post-Caesarean section niche-related impaired fertility: hypothetical mechanisms. Human Reproduction (Oxford, England), 35 (7), 1484–1494.
- Vissers, J., et al., 2020. Reduced pregnancy and live birth rates after in vitro fertilization in women with previous Caesarean section: a retrospective cohort study. Human Reproduction (Oxford, England), 35 (3), 595–604.
- Wang, L., et al., 2022. Pregnancy and Perinatal Outcomes of Patients With Prior Cesarean Section After a Single Embryo Transfer in IVF/ICSI: A Retrospective Cohort Study. Frontiers in Endocrinology, 13, 851213.
- Yang, X., et al., 2021. Front Med (Lausanne) 8.
- Yang, X., et al., 2022. Interaction between Cervical Microbiota and Host Gene Regulation in Caesarean Section Scar Diverticulum. Microbiology Spectrum, 10 (4), e0167622.
- Zhang, Y., et al., 2022. Previous caesarean delivery and the presence of caesarean scar defects could affect pregnancy outcomes after in vitro fertilization frozen-thawed embryo transfer: a retrospective cohort study. BMC Pregnancy and Childbirth, 22 (1), 769.
- Zhao, J., et al., 2021. Impact of previous Caesarean section on reproductive outcomes after assisted reproductive technology: systematic review and meta-analyses. Reproductive Biomedicine Online, 43 (2), 197–204.