

Abstract
Background
The aim is to investigate the risk of short-term maternal morbidity caused by the selective clinical use of episiotomy (rate < 0.02), and to compare the risk of severe perineal tears with the statewide risk.
Methods
In this retrospective cohort study, we investigated the effect of selective episiotomy on the risk of severe perineal tears and blood loss in singleton term deliveries, using propensity scores with inverse probability weighting.
Results
This study included 10992 women who delivered vaginally between 2008–2018. Episiotomy was performed in 171 patients (1.55%), three of whom (1.75%) experienced severe perineal tears compared to 156 (1.44%) in the control cohort. The adjusted odds ratio of severe perineal tears was 2.06 (95% confidence interval [CI]: 0.51, 8.19 with 0.3 p value). Multivariate linear regression showed that episiotomy increased blood loss by 96.3 ml (95% CI: 6.4, 186.2 with 0.03 p value). Episiotomy was performed in 23% (95% CI: 0.228, 0.23) of vaginal deliveries in the state of Hessen, with a risk of severe perineal tears of 0.0143 (95% CI: 0.0139, 0.0147) compared to 0.0145 (95% CI: 0.0123, 0.0168) in our entire cohort.
Conclusions
Selective use of episiotomy does not increase the risk of higher-grade perineal tears. However, it may be associated with maternal morbidity in terms of increased blood loss.
PLAIN LANGUAGE SUMMARY
An episiotomy is a cut between the vagina and the anus that may be performed by an obstetrician during childbirth and can result in increased blood loss or severe birth tears. In this study, we investigated the risks of both bleeding and severe tears caused by a highly selective local practice of episiotomies below 2% and compared the results with statewide data. The study included 10992 women who delivered between 2008–2018, 171 of whom underwent episiotomies according to the hospital’s protocols. Having an episiotomy did not increase the likelihood of severe birthing tears but was associated with an increase in estimated blood loss. Therefore, although highly selective use of episiotomy is unlikely to cause more severe tears, it has the potential to worsen the mother’s health by increasing blood loss.
Introduction
Episiotomy is a surgical procedure used to enlarge the vaginal orifice by incising the perineum during the second stage of labour (Carroli and Mignini Citation2009, Beyene et al. Citation2020). Episiotomies can be classified into three major types, including median, mediolateral, and lateral episiotomies (Räisänen et al. Citation2010, Stedenfeldt et al. Citation2012). Episiotomies are believed to be beneficial for the prevention of extensive perineal lacerations, allowing easy repair, and expediting delivery of the baby (Sagi-Dain and Sagi Citation2016, Sagi-Dain et al. Citation2018, Sangkomkamhang et al. Citation2020). Nevertheless, definitive evidence for defined episiotomy criteria or a clear benefit in reducing maternal and neonatal morbidities is lacking (Bansal et al. Citation1996). Episiotomies are also associated with severe bleeding, severe perineal tears, infection, haematoma, and wound dehiscence. However, long-term complications include scar tissue formation, dyspareunia, anorectal incontinence, and severe tears during childbirth (Gün et al. Citation2016).
The global episiotomy rate has been declining as a result of the predominant selective indication-based approach to episiotomy (rate below 0.1) following the World Health Organisation (WHO) recommendation to avoid routine episiotomies (World Health Organisation Citation1985, de la Santé Citation1997). Episiotomy rates have dropped in many countries, ranging from 0.037 in Denmark to 0.2 in France (Blondel et al. Citation2016, Goueslard et al. Citation2018). Nevertheless, healthcare providers in some regions, such as Cyprus, still perform routine episiotomies at a rate of 0.75, especially in nulliparous women (Blondel et al. Citation2016, Beyene et al. Citation2020).
Two Cochrane reviews reported lower rates of perineal trauma with selective use of episiotomies than with routine use, with similar short- and long-term adverse outcomes for both mothers and newborns (Carroli and Mignini Citation2009, Jiang et al. Citation2017). Therefore, the International Federation of Gynaecology and Obstetrics (FIGO) published a statement against routine episiotomies, emphasising that episiotomies should not be ‘withheld in all circumstances’ (Nassar et al. Citation2019). The National Institute of Health Care Excellence (NICE) recommends the use of episiotomy in vaginal operative deliveries, whereas the American College of Obstetricians and Gynaecologists (ACOG) advises against its use in routine practice (ACOG Citation2015, Nice Citation2023).
Conflicting views on episiotomies highlight the need for more evidence to address whether they protect against severe perineal tears. In our study, selective episiotomy is defined as an episiotomy that is performed strictly because of an extremely abnormal foetal cardiac trace indicating hypoxia, in which the perineum is the sole hindrance to immediate delivery. In this study, we aimed to investigate the association between strict selective episiotomy and the risk of short-term maternal morbidity, including severe perineal tears and bleeding. We also aimed to compare the risk of severe perineal tears in this cohort with that in the population of the state of Hessen, Germany.
Methods
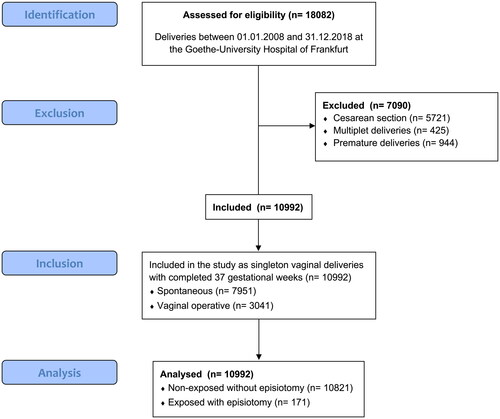
This retrospective cohort study included all-term vaginal singleton deliveries over more than a decade at the Obstetrical Unit of the Goethe-University Hospital of Frankfurt. The obstetrical medical records at this tertiary referral centre are routinely and prospectively documented in an electronic database (GeDoWin®, Saatmann GmbH, Worms). This database was utilised to identify eligible deliveries between January 1, 2008 and December 31, 2018. The inclusion criteria were singleton pregnancies completed at 37 gestational weeks, cephalic or breech presentation, and spontaneous and vaginal operative deliveries. Births with foetal abnormalities, small for gestational age, prior caesarean section, gestational diabetes, or other maternal comorbidities were intentionally included to increase generalisability. The exclusion criteria were multiplets and premature birth. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were followed in this study, and a study flowchart is shown in .
Figure 1. Flowchart of the study cohort.
The study cohort included two exposure groups: an exposed group with episiotomies (EPI) and a non-exposed group without episiotomies (NoEPI). All episiotomies were performed according to our selection policy: only when the foetal head was crowned, foetal bradycardia was present, and the perineum clearly hindered the delivery. Maternal and neonatal demographic variables, such as age, weight, height, body mass index (BMI), gravidity, parity, and gestational age, were recorded for both exposure groups. Further covariates included the presentation of the foetus, duration of labour stages, use of epidural analgesia, type of episiotomy, and induction of labour, and the database contained no missing information. For further comparative analysis, reference data from Hessian hospitals were obtained from the ‘Perinatalerhebung Hessen’ database (a standardised statewide database that collects perinatal outcome data).
We used two outcomes as surrogates for maternal morbidity; the primary outcome was the occurrence of severe perineal lacerations (third- and fourth-degree tears) as a binomial variable, and maternal blood loss was a secondary outcome of the continuous variables. A senior obstetrician confirmed all perineal tears to avoid misclassification or bias.
Vaginal operative deliveries in this cohort included forceps deliveries and vacuum extractions. Our team uses Kielland forceps to guide the foetal head when delivery fails or when there is a need to accelerate the second stage of labour (Patel and Murphy Citation2004, Vayssière et al. Citation2011, Nash et al. Citation2015). Vacuum extraction is normally used in term deliveries to avoid foetal distress and resolve failure to progress or when the preclusion of voluntary maternal expulsive efforts is advised (Vacca Citation1999, Putta and Spencer Citation2000). Manual assistance is limited to breech presentation, where it might support the rotation of the shoulders, delivery of the arms, or increase deflection of the foetal head (Jennewein et al. Citation2019).
Statistical analysis was conducted with Stata® (ver. 18, Texas, USA). Propensity scores with inverse probability weighting, univariate and multivariate logistic regression, and linear regression were used to address the confounding factors. Pearson’s chi-square test and two-sample t-test with a p value of 0.05 as a cut-off for statistical significance were used.
The study was approved by the local Ethics Committee (reference number 20-840) and patient consent was not required.
Results
Between 2008 and 2018, 10992 vaginal deliveries met the inclusion criteria. Practitioners performed episiotomy in 171 deliveries (1.55%). Overall, 7951 (72.3%) spontaneous vaginal deliveries, 2163 (19.6%) forceps deliveries, 19 (0.17%) vacuum extractions, and 859 (7.8%) manually assisted deliveries were performed. Median, mediolateral, and lateral episiotomies accounted for 60.23%, 37.42%, and 2.34% of cases, respectively. summarises the descriptive statistics of the two groups.
Table 1. Demographic characteristics of the two exposure study cohorts as well as the distribution of the main two outcomes of severe perineal tears and blood loss with crude descriptive statistical analyses.
The EPI and NoEPI cohorts showed no significant difference in maternal age (32 ± 4.6 vs. 31.9 ± 5.0 years), gestational age (280 vs. 279 days), birth weight (3391 ± 452 vs. 3410 ± 446 g), or induction of labour (17.5% vs. 14.9%). The BMI was lower in the EPI compared to the NoEPI group (22.2 ± 3.4 vs. 23.7 ± 4.8) and the total duration of labour (first and second stage) was significantly longer in the EPI group (364 vs. 270 min). Furthermore, patients who underwent episiotomy were more likely to be nulliparous and to receive epidural analgesia.
Cephalic presentation was the most common foetal position in both cohorts; however, more regular cephalic presentations were observed in the NoEPI group than in the EPI group (88.8% vs. 78.5%). Irregular cephalic presentations were almost twice as likely in the EPI group than in the NoEPI group (5.3% vs. 3%). Similarly, breech presentation was approximately twice as likely in the EPI group as in the NoEPI group (15.8% vs. 8.3%). These results indicate that episiotomy is positively associated with an irregular presentation and position.
Episiotomy was performed in 0.89% of all spontaneous deliveries and 3.28% of operative vaginal deliveries. In the EPI group, 58.5% of births ended with a vaginal operative delivery, which was significantly higher than that in the non-EPI group (27.2%).
The NoEPI cohort included 156 (1.44%) patients with severe perineal tears, whereas the EPI cohort included three (1.45%) patients with severe perineal tears. The unadjusted odds ratio (OR) of the primary outcome of severe perineal tears in the EPI compared to the NoEPI cohort was not significant at 1.22 (95% confidence interval [CI]: 0.39, 3.87 with 0.73 p value), whereas the ß-coefficient for blood loss was significant at 75.9 ml (95% CI: 46.7, 105 with < 0.001 p value) according to univariate regression. The findings in show that several characteristics and potential confounders were unbalanced, with statistical significance between the exposure groups; therefore, we can assume that the crude effect of episiotomy on severe perineal tears and blood loss outcomes was confounded by indication.
Multivariate logistic regression was used to build a model for predicting exposure assignment (undergoing an episiotomy), and propensity scores were calculated. The covariates of the model with corresponding coefficients and CIs are shown in . The resulting propensity score distributions for the two groups are shown in and demonstrate a wide common support region.
Figure 2. Distribution of the propensity score density based on the exposure to an episiotomy.
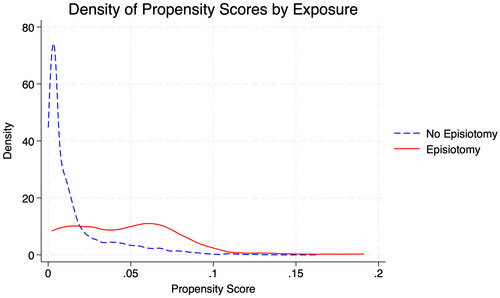
Table 2. Multivariate logistic regression model to create the propensity scores predicting the probability of performing an episiotomy as a function of potential confounders (age, gestational age, birth weight, BMI, nulliparity, induction of labour, duration of labour, epidural analgesia, mode of vaginal delivery, foetal presentation).
Subsequently, inverse probability weighting was used to weigh the data and develop a new pseudo-population with 2,605.1 exposed and 2,776.9 non-exposed observations. The standardised differences and ratios of variance for all confounders are summarised in , which shows a suboptimal balance of confounders between the two cohorts, with some weighted differences above 0.1, but with a weighted ratio of variance between 0.5 and 2.
Table 3. Covariate balance and standardised differences between the episiotomy exposed (EPI) and the non-exposed (NoEPI) cohorts in the new dataset after the inverse probability weighting propensity score model.
Double robust multivariate logistic and linear regression using inverse probability weights and controlling for induction of labour, duration of labour, nulliparity, epidural analgesia, and mode of vaginal delivery showed that episiotomy was not significantly associated with severe perineal tears (OR: 2.06; 95% CI: 0.51, 8.19 with 0.3 p value), but was significantly associated with blood loss, with a ß-coefficient of 96.3 ml (95% CI: 6.4, 186.2 with 0.03 p value).
During the study period, 373.250 vaginal births were documented in the state of Hessen. An average of 23% (95% CI: 0.228–0.23) of the patients underwent an episiotomy while giving birth, which was significantly higher than the 1.5% (95% CI: 0.0128, 0.0175) of patients at our centre. Regarding the primary outcome of interest, the average rate of severe perineal tears was 0.0143 (95% CI: 0.0139, 0.0147) in Hessen and 0.0145 (95% CI: 0.0123, 0.0168) in our centre.
Discussion
The benefit of episiotomies in preventing higher-grade perineal lacerations is controversial (Thacker and Banta Citation1983, Sangkomkamhang et al. Citation2020). Cochrane analyses of different practices involving routine versus selective episiotomy have been published and have shown that performing fewer episiotomies during spontaneous vaginal delivery reduces the risk of higher-degree perineal trauma by 30% (Hartmann et al. Citation2005, Jiang et al. Citation2017), which contradicts several current recommendations that highlight the protective role of episiotomy against higher-grade tears (De Leeuw et al. Citation2008, Nice Citation2023). Additionally, the findings of the Cochrane analyses suggest that a further reduction in severe perineal trauma can be achieved when episiotomies are entirely avoided, with a few exceptions. The likelihood of episiotomy in our study was 1.55% and episiotomy did not significantly affect the risk of severe perineal tears. Nevertheless, they were associated with a trend towards a higher risk of high-degree perineal tears (0.0175) than the NoEPI group (0.0144), albeit the difference was not significant. This finding is consistent with nationwide data from 2014, where the percentage of episiotomy (22.7%) among 469258 vaginal births increased the risk of higher-grade perineal tears from 0.0104 to 0.0253. Therefore, our study shows that episiotomies do not protect mothers from higher-degree perineal tears, and consequently, do not improve maternal morbidity. In contrast, they may also be a cause of increased morbidity, even if not statistically significant. Therefore, this finding should be interpreted with caution. Recent trends show that while the incidence of severe tears decreases with a reduction in the voluntary episiotomy rate, the rate of severe tears associated with instrumental delivery increases (Leclercq et al. Citation2024).
The episiotomy rate was higher (3.28%) during operative vaginal delivery than during spontaneous delivery (0.89%). Operative delivery increases the likelihood of practitioners’ non-adherence to the selective episiotomy approach, likely due to the NICE/RCOG guidelines (Pai Citation2013, Nice Citation2023). However, it is unclear whether episiotomies during vaginal operative delivery truly protect against severe perineal tears. De Leeuw et al. showed a higher risk of third-degree perineal tears during vaginal operative deliveries and subsequently recommended the use of mediolateral episiotomy to reduce this risk (De Leeuw et al. Citation2001). In contrast, Dandolu et al. showed a significantly higher risk of perineal laceration during vaginal operative deliveries when an episiotomy was performed (Dandolu et al. Citation2005). Similarly, Kudish et al. demonstrated an increased risk of anal sphincter injuries with the use of episiotomies during operative vaginal deliveries and recommended avoiding this combination (Kudish et al. Citation2006). Ecker et al. examined the effect of reducing the use of routine episiotomy for vaginal operative deliveries on the risk of high-grade perineal tears and demonstrated an unchanged risk of third-degree lacerations with a decreased risk of fourth-degree lacerations (Ecker et al. Citation1997). In our department, forceps are removed before the foetal head passes the perineum as standard protocol to prevent perineal tears, and the current belief is that operative delivery could be a modifier for the association between episiotomies and severe perineal tears (Muraca et al. Citation2024).
Most previous studies have compared two clinical practice protocols for the primary outcomes of advanced perineal tears. Numerous studies have compared routine episiotomy to selective episiotomy or to a cohort in which episiotomies are almost completely avoided. Two randomised controlled trials focused on the implementation of a ‘non-episiotomy’ protocol compared to ‘selective episiotomy’ practice, with the aim to limit the number of episiotomies performed in clinical practice to an absolute minimum (M Amorim et al. Citation2017, Sagi-Dain et al. Citation2018). Although our study shares the same core idea as these trials, the episiotomy rate of both randomised trials was much higher than that reported in the current study (approximately 20%), which was justified by the non-compliance of practitioners to the non-episiotomy practice (Sagi-Dain et al. Citation2018). Although these studies showed limited success towards their main goal, in our study, although not a randomised controlled trial, we compared our selective episiotomy protocol (1.55%) to another protocol (23%), followed by the rest of the statewide hospitals. Therefore, the present study was particularly successful in comparing cohorts with functionally different episiotomy rates.
Regarding the primary outcome of interest, the rate of severe perineal lacerations did not significantly increase in our patients, indicating that the selective policy did not endanger women by increasing short-term morbidity. An important limitation of our study was the lack of long-term follow-up to assess additional morbidity. Turmo et al. showed that 12.8% of women develop chronic pain after episiotomies (Turmo et al. Citation2015), whereas other studies have shown that a woman’s sex life could be negatively affected by higher rates of dyspareunia and insufficient lubrication (Ejegård et al. Citation2008). Moreover, women who undergo episiotomy are more susceptible to anxiety-related symptoms and display a greater negative body perception even a year after delivery than women with severe lacerations, which emphasises the importance of long-term outcomes (Molyneux et al. Citation2024). In this study, episiotomy increased blood loss by approximately 96 ml even after adjusting for all available confounders, which is in line with the results of previous studies (Baksu et al. Citation2008). However, this significant increase is not necessarily clinically significant, and may not have increased maternal morbidity.
In conclusion, this study showed that short-term maternal morbidity did not increase when episiotomies were performed in a selective clinical approach. Regardless, the risk of severe perineal lacerations is low, and we do not support the assumption that episiotomies prevent severe tears, although they should be considered in forceps deliveries. These findings provide evidence for the adoption of a selective clinical approach for episiotomies and highlight the need to re-evaluate episiotomy indications in obstetrical centres with the goal to reduce perineal trauma. This approach protects women by reducing short- and long-term morbidities. Our study has several limitations, including the fact that the EPI group mainly contained primigravids, which is not surprising as nulliparous women are six times more likely to undergo episiotomy (Beyene et al. Citation2020). Additionally, we were unable to include psychometric measures in our definition of short-term morbidity because of the retrospective study design, and episiotomies are known to significantly affect women’s birth satisfaction (D’Sa et al. Citation2024). Another shortcoming is that our data did not allow investigation of the effect of episiotomy type on perineal tears, and studies have reported that the outcomes of lateral and mediolateral episiotomies differ (Sagi-Dain and Sagi Citation2015, Rusavy et al. Citation2016). Moreover, there is evidence of the value of computational modelling of the pelvic floor anatomy to simulate biochemical processes and study parturition. Such studies could investigate the effect of episiotomy type on perineal tears. One previous study showed that mediolateral episiotomies have a protective effect on the pelvic floor musculature (Oliveira et al. Citation2016). Finally, this was a retrospective cohort study, and information bias and confounders remain a concern despite the fact that we tried to minimise them with propensity scores and double robust regression analyses.
In addition to innovative statistical methods that strengthened the study design, the properties of the study centre as a specialised delivery unit for breech presentation and the use of forceps amplify the novelty of this cohort and the presented data. Future randomised controlled trials with strict adherence to selective episiotomy are necessary to further investigate maternal morbidity. Although our findings indicate the potential of episiotomies to increase maternal morbidity, we wish to emphasise that episiotomy is a meaningful obstetrical measure, the indications of which should be critically considered and weighed against the possible drawbacks for the mother and foetus.
Acknowledgements
We thank all of our patients and colleagues who made this project possible. This study is part of the doctoral thesis of the first author.
Disclosure statement
The authors declare that they have no conflicts of interest.
Data availability statement
Anonymised unidentifiable raw data from this project are available for at least 5 years after publication upon request.
Additional information
Funding
References
- ACOG, 2015. ACOG practice bulletin number 154. ACOG practice bulletin no. 154: operative vaginal delivery. Obstetrics & Gynecology, 126 (5), 1–8.
- Baksu, B., et al., 2008. Effect of timing of episiotomy repair on peripartum blood loss. Gynecologic and Obstetric Investigation, 65 (3), 169–173.
- Bansal, R.K., et al., 1996. Is there a benefit to episiotomy at spontaneous vaginal delivery? A natural experiment. American Journal of Obstetrics and Gynecology, 175 (4 Pt 1), 897–901.
- Beyene, F., et al., 2020. Factors associated with episiotomy practices in Bahirdar City, Ethiopia: a cross-sectional study. Risk Management and Healthcare Policy, 13, 2281–2289.
- Blondel, B., et al., 2016. Variations in rates of severe perineal tears and episiotomies in 20 European countries: a study based on routine national data in Euro-Peristat Project. Acta Obstetricia Et Gynecologica Scandinavica, 95 (7), 746–754.
- Carroli, G. and Mignini, L., 2009. Episiotomy for vaginal birth. Cochrane Database of Systematic Reviews, (1), CD000081.
- D’Sa, J.L., et al., 2024. Psychometric properties of a Saudi Arabian version of the Birth Satisfaction Scale-Revised (BSS-R). Belitung Nursing Journal, 10 (1), 105–113.
- Dandolu, V., et al., 2005. Risk factors for obstetrical anal sphincter lacerations. International Urogynecology Journal and Pelvic Floor Dysfunction, 16 (4), 304–307.
- De Leeuw, J.W., et al., 2001. Risk factors for third degree perineal ruptures during delivery. BJOG: An International Journal of Obstetrics and Gynaecology, 108 (4), 383–387.
- De Leeuw, J.W., et al., 2008. Mediolateral episiotomy reduces the risk for anal sphincter injury during operative vaginal delivery. BJOG: An International Journal of Obstetrics and Gynaecology, 115 (1), 104–108.
- de la Santé, O.M., 1997. Les soins liés à un accouchement normal: guide pratique. Genève: Rapport d’un groupe de travail technique.
- Ecker, J.L., et al., 1997. Is there a benefit to episiotomy at operative vaginal delivery? Observations over ten years in a stable population. American Journal of Obstetrics and Gynecology, 176 (2), 411–414.
- Ejegård, H., Ryding, E.L. and Sjogren, B., 2008. Sexuality after delivery with episiotomy: a long-term follow-up. Gynecologic and Obstetric Investigation, 66 (1), 1–7.
- Goueslard, K., et al., 2018. How did episiotomy rates change from 2007 to 2014? Population-based study in France. BMC Pregnancy and Childbirth, 18 (1), 208.
- Gün, İ., Doğan, B. and Özdamar, Ö., 2016. Long- and short-term complications of episiotomy. Turkish Journal of Obstetrics and Gynecology, 13 (3), 144–148.
- Hartmann, K., et al., 2005. Outcomes of routine episiotomy: a systematic review. JAMA, 293 (17), 2141–2148.
- Jennewein, L., et al., 2019. The influence of the fetal leg position on the outcome in vaginally intended deliveries out of breech presentation at term – a FRABAT prospective cohort study. PLOS One, 14 (12), e0225546.
- Jiang, H., et al., 2017. Selective versus routine use of episiotomy for vaginal birth. The Cochrane Database of Systematic Reviews, 2 (2), CD000081.
- Kudish, B., et al., 2006. Operative vaginal delivery and midline episiotomy: a bad combination for the perineum. American Journal of Obstetrics and Gynecology, 195 (3), 749–754.
- Leclercq, C., Braund, S. and Verspyck, E., 2024. Évolution du taux d’épisiotomies et des lésions obstétricales du sphincter de l’anus depuis les recommandations de 2018. Gynecologie, Obstetrique, Fertilite & Senologie, 52 (2), 95–101.
- M Amorim, M., et al., 2017. Selective episiotomy vs. implementation of a non-episiotomy protocol: a randomized clinical trial. Reproductive Health, 14 (1), 55.
- Molyneux, R., Fowler, G. and Slade, P., 2024. The postnatal effects of perineal trauma on maternal psychological and emotional wellbeing: a longitudinal study. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 294, 238–244.
- Muraca, G.M., et al., 2024. Variation in episiotomy use among nulliparous individuals by maternity care provider and associated rates of obstetric anal sphincter injury. Journal of Obstetrics and Gynaecology Canada: JOGC = Journal D’obstetrique Et Gynecologie Du Canada: JOGC, 46 (5), 102415.
- Nash, Z., Nathan, B. and Mascarenhas, L., 2015. Kielland’s forceps. From controversy to consensus? Acta Obstetricia Et Gynecologica Scandinavica, 94 (1), 8–12.
- Nassar, A.H., et al., 2019. FIGO statement: restrictive use rather than routine use of episiotomy. International Journal of Gynaecology and Obstetrics: The Official Organ of the International Federation of Gynaecology and Obstetrics, 146 (1), 17–19.
- Nice, G.C., 2023. Intrapartum care for healthy women and babies.
- Oliveira, D.A., et al., 2016. A biomechanical analysis on the impact of episiotomy during childbirth. Biomechanics and Modeling in Mechanobiology, 15 (6), 1523–1534.
- Pai, H.D., 2013. Manual on vaginal surgery: workshop manual. New Delhi: Jaypee Brothers Medical Publishers.
- Patel, R.R. and Murphy, D.J., 2004. Forceps delivery in modern obstetric practice. BMJ (Clinical Research Ed.), 328 (7451), 1302–1305.
- Putta, L.V. and Spencer, J.P., 2000. Assisted vaginal delivery using the vacuum extractor. American Family Physician, 62 (6), 1316–1320.
- Räisänen, S., Vehviläinen-Julkunen, K. and Heinonen, S., 2010. Need for and consequences of episiotomy in vaginal birth: a critical approach. Midwifery, 26 (3), 348–356.
- Rusavy, Z., Karbanova, J. and Kalis, V., 2016. Timing of episiotomy and outcome of a non-instrumental vaginal delivery. Acta Obstetricia Et Gynecologica Scandinavica, 95 (2), 190–196.
- Sagi-Dain, L. and Sagi, S., 2015. The correct episiotomy: does it exist? A cross-sectional survey of four public Israeli hospitals and review of the literature. International Urogynecology Journal, 26 (8), 1213–1219.
- Sagi-Dain, L. and Sagi, S., 2016. Indications for episiotomy performance – a cross-sectional survey and review of the literature. Journal of Obstetrics and Gynaecology: The Journal of the Institute of Obstetrics and Gynaecology, 36 (3), 361–365.
- Sagi-Dain, L., et al., 2018. No episiotomy versus selective lateral/mediolateral episiotomy (EPITRIAL): an interim analysis. International Urogynecology Journal, 29 (3), 415–423.
- Sangkomkamhang, U., et al., 2020. Restrictive versus routine episiotomy among Southeast Asian term pregnancies: a multicentre randomised controlled trial. BJOG: An International Journal of Obstetrics and Gynaecology, 127 (3), 397–403.
- Stedenfeldt, M., et al., 2012. Episiotomy characteristics and risks for obstetric anal sphincter injuries: a case-control study. BJOG: An International Journal of Obstetrics and Gynaecology, 119 (6), 724–730.
- Thacker, S.B. and Banta, H.D., 1983. Benefits and risks of episiotomy: an interpretative review of the English language literature, 1860–1980. Obstetrical & Gynecological Survey, 38 (6), 322–338.
- Turmo, M., et al., 2015. Development of chronic pain after episiotomy. Revista Espanola De Anestesiologia y Reanimacion, 62 (8), 436–442.
- Vacca, A., 1999. The trouble with vacuum extraction. Current Obstetrics & Gynaecology, 9 (1), 41–45.
- Vayssière, C., et al., 2011. Instrumental delivery: clinical practice guidelines from the French College of Gynaecologists and Obstetricians. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 159 (1), 43–48.
- World Health Organisation, 1985. Appropriate technology for birth. Lancet (London, England), 2 (8452), 436–437.