
Abstract
Governments across the globe imposed behavioral restrictions to halt the spread of the COVID-19. These preventive behaviors became a moralized issue and engagement in those behaviors varied. In moral psychology, there are various theoretical frameworks with measures of individual differences that concern the way we form moral judgments. In a pre-registered longitudinal three-wave project started before the pandemic, we examined the predictive power of several moral measures on compliance with behavioral guidelines, moralization toward noncompliance, and intention to vaccinate and actual vaccine uptake. Mature integrative and deliberative moral thinking predicted moralization and compliance better than several measures of utilitarianism. These results hold when controlling for Fear of Covid-19 and sociodemographic factors.
Pandemic mitigation quickly became a moralized issue (Bor et al., Citation2023; Prosser et al., Citation2020) as the new suite of behaviors to prevent COVID-19 from spreading became a target of moral judgments (Francis & McNabb, Citation2020; Halpern, Citation2020; Stroebe et al., Citation2021). The moral environment quickly changed as norms of the pre-pandemic situation were not adequate to deal with the new challenges that the novel virus threw at everyone. Since the pandemic represents a set of unprecedented problems for moral cognition, it also provides a way of testing moral psychological research questions in a way that is arguably more ecologically valid than typical experimental methods. Thus, the COVID-19 pandemic effectively functioned as a real-life test of people’s moral attitudes and values. It is easy for humans to declare moral values before they are thrown into harsh reality, which challenges and tests their stated preferences. There is a long tradition in social psychology of investigating people’s stated and revealed preferences (De Corte et al., Citation2021) and COVID-19 offers a unique window into this topic, by comparing moral preferences before and during the pandemic.
Indeed, some longitudinal studies have already been conducted on the effects that the pandemic may have had on moral dispositions (Vartanova et al., Citation2021) and on changes in moral norms during the pandemic (Bor et al., Citation2023; Zhou et al., Citation2023). However, little literature exists about how individuals’ prior moral dispositions shaped their responses to pandemic mitigation—i.e., when the moral environment changed. The present study focuses on just this. That is, how well do moral psychological questionnaires, taken before the pandemic, predict self-reported behavior or moralization of others’ behavior during the pandemic? Further, do those relationships change when both are measured during the pandemic when the moral environment was similar?
To mitigate the spread of COVID-19, The World Health Organization (Citation2020) recommended, among other things, avoiding public places, wearing a mask, maintaining a physical distance from other people, and practicing good hand hygiene (i.e., preventive behaviors). Governments followed with restrictions, quarantines, recommendations, and mandates regarding public behavior (i.e., behavioral restrictions). When the first COVID-19 vaccines were developed, many campaigns were designed to encourage their uptake. While many people adopted preventive behaviors even before authorities recommended or mandated them, with many more following later (Haischer et al., Citation2020), a portion of the population continued to neglect them.
Countries also implemented these measures to different extents with their reception and societal impact—both intended and unintended—varied by the function of different political climates. In the present study, we focus on the UK and US, being the two majority countries in our sample. In the UK, the handling of the pandemic in the beginning was characterized by inaction with a focus on potential breaches of civil liberties (see Frowde et al., Citation2020). In the US, the pandemic response was politically polarized under the Trump administration, with misinformation about the virus often presented in mainstream media (Kerr et al., Citation2021; Motta et al., Citation2020). Perhaps unsurprisingly, this resulted in varying levels of trust in governments during this time; a factor that predicted compliance toward precautionary measures and prejudice toward immigrants (Frackowiak et al., Citation2023; Han et al., Citation2023; Shanka & Menebo, Citation2022; Vacchini et al., Citation2021).
Preventive behaviors during the pandemic soon became moralized, through a change of the moral environment. That is, following or not following preventative behaviors expressed a value in addition to being a personal preference (see Rozin, Citation1999). Bor et al. (Citation2023) showed that social distancing became a moralized issue in the early stages of the pandemic. In another study, images of mask-wearers were rated more trustworthy, albeit less likely to be healthy, compared to non-wearers (Olivera-La Rosa et al., Citation2020). Moral reactions have not always been supportive of prevention, with numerous demonstrations protesting against lockdowns, mask-policies, and other restrictions occurring globally (Gerbaudo, Citation2020). Moreover, a moral divide has been observed with vaccination as well (Rosenfeld & Tomiyama, Citation2022). Van Bavel et al. (Citation2022) found that in the US, higher national identification predicted greater engagement with the preventative behaviors, whereas in UK their association was very low. However, in the UK, community identification predicted adherence with restrictions (Stevenson et al., Citation2021).
Despite the existing literature on how affective processes—like trust and moral emotions—influenced people’s reactions toward the COVID-19 pandemic, individual differences are also likely to provide an explanation for the observed divides in moral reactions. It has been established that some morally-relevant individual differences, such as antisocial traits (O’Connell et al., Citation2021) and empathy (Pfattheicher et al., Citation2020), play a role in motivating (or inhibiting) preventive behaviors. The field of moral psychology has, from its various theoretical frameworks, uncovered numerous individual differences in what factors influence people’s moral thinking. These differences concern reasoning styles (affective and/or deliberative), what factors individuals take into account when evaluating whether something is right or wrong (e.g., the Moral Foundations model; Graham et al., Citation2011), and preferences for utilitarian or deontological ethics (Kahane et al., Citation2018; Laakasuo et al., Citation2017). Below we review several individual differences in moral cognition and examine the rationale for considering them relevant for COVID-19-related behaviors and moral judgments.
Utilitarian and deontological ethics
One tradeoff in COVID-19 prevention has been minimizing the risk and harm caused by the disease with the cost of restricted freedom. Utilitarian ethics demand actions that maximize the overall good while minimizing the overall harm. In contrast, deontological ethics dictate that certain acts are inherently wrong, regardless of situational factors or potential consequences. Kahane et al. (Citation2018) argued utilitarian ethics consists of two aspects: impartial beneficence, i.e., distributing good equally across people, and instrumental harm, i.e., accepting harm for the greater good.
Some behavioral restrictions clearly have utilitarian reasoning behind them. The stated rationale for individuals restricting their personal freedom is to protect others (instrumentality) in general, not just immediate friends or family (impartiality). Furthermore, people being willing to incur that penalty to themselves (i.e., limiting their own personal freedom) implies impartiality in regard to who has to make sacrifices. It would make sense for higher endorsement of utilitarianism to predict higher compliance with restrictions if those restrictions are believed to maximize welfare and/or minimize harm for the greatest number of people. However, it is less clear whether endorsements of instrumental harm or impartial beneficence specifically would be stronger predictors.
Moral orientations
A recent psychometric model (see Fleischmann et al., Citation2019) proposes four different styles of moral thinking, i.e., moral orientations. According to the model, people approach moral problems relying on either (1) a combination of affective and cognitive processes (Integration orientation), (2) pragmatic aspects (Deliberation orientation), (3) emotions (Sentiment orientation), or (4) established conventions (Rule orientation). Moral orientations are not mutually exclusive: an individual may score highly on more than one orientation. Each of the moral orientations potentially plays a role in preventive behaviors. Firstly, fear of infection as well as fear of punishment have been found to be self-centered motives for social distancing (Christner et al., Citation2020; corresponding to sentiment and rule orientations, respectively). Adopting preventive behaviors could also be seen as a pragmatic approach to the situation (corresponding to the deliberation orientation), and navigating among these different motivations as an instance of integration orientation. Fleischmann et al. (Citation2019) describe the Deliberation orientation and Integration orientation as “mature moral thinking.”
Moral foundations
Individual differences also exist in which properties of actions are considered morally relevant, and these could in turn influence whether adopting preventive behaviors is seen as morally worthwhile and neglecting them seen as condemnable. According to the Moral Foundations Theory (see, e.g., Graham et al., Citation2011), people have “moral taste buds” (Graham et al., Citation2013, p. 60) that are sensitive to certain properties of actions. The more an observed act “triggers” them, the more it is considered relevant. The exact number of these moral foundations is up to debate, but the most established five include sensitivity to: Care/Harm (e.g., cruelty, care-taking), Fairness/Cheating (inequality), Loyalty/Betrayal (violating ingroup norms), Authority/Subversion ([dis]obeying one’s boss, [dis]respecting one’s parents), and Purity/Degradation (violating taboos, disgusting acts, [dis]respecting sacred symbols).
Both the Care and Fairness foundations could motivate preventive behaviors because those behaviors protect others and failure to do so could be viewed as free-riding. Chan (Citation2021) showed that higher Care and Fairness foundations predicted increased staying home, mask-wearing, and social distancing, whereas the Purity foundation predicted the opposite—which is peculiar, considering that it has been linked with disgust sensitivity and avoidance of potentially sick individuals previously (Laakasuo et al., Citation2018). When preventive behaviors are established as widely recognized norms and officially recommended, they could also relate to loyalty and authority moral foundations. For example, supporting authorities were found to be the strongest predictor for complying with preventive measures during the pandemic (Murphy et al., Citation2020).
Morality as cooperation (MAC)
Pandemic mitigation is a large-scale cooperative effort, and individual differences in valuing different aspects of cooperation might influence their pandemic-related behaviors and moral judgments. The Morality as Cooperation Theory (MAC; Curry et al., Citation2019) bears similarities to the Moral Foundations Theory but claims that morality evolved specifically as a solution to problems of cooperation. Thus, people’s “moral taste buds” should be attuned to aspects related to cooperation. MAC postulates seven types of cooperation that people consider more or less central to their own morality: (1) Family, (2) Group loyalty, (3) Reciprocation, (4) Heroism, (5) Respect, (6) Fairness, and (7) Property rights.
Parts of MAC (group loyalty, respect, and fairness) are conceptually similar to Moral Foundations and are thus relevant to pandemic behavior for the same reasons. Moreover, protecting one’s family members could be a prime motivator for not visiting one’s elderly parents or grandparents. Further, Heroism could relate to the individuals who adopted preventive behaviors before official recommendations or mandates. On the other hand, Heroism could be associated with disobeying official mandates that one views as unnecessary or unjust.
The current research
In this longitudinal research project—for which data collection started in mid-2019, half a year before COVID-19 pandemic started—we investigated the relationships between the moral dispositions reviewed above and compliance with pandemic-related preventive behaviors, the moralization of not practicing them, as well as willingness to take the COVID-19 vaccine. We wanted to examine and compare the predictive power of different moral inclinations on these variables. Moreover, we wanted to see if these preferences have predictive power even if they were measured before the pandemic—if they would, this would be a relatively strong test of their predictive validity.
Naturally, such research could not have been planned: we had initially collected cross-sectional data for another project, including several moral measures as covariates, pre-pandemic. Once the pandemic had started, we decided to contact the participants again via the recruitment platform and collected pandemic-related variables as well as additional individual differences measures to expand the survey. Thus, we had no a priori hypotheses, and the measures included in the first wave of data collection were not selected with the idea of examining longitudinal trends in mind. For the present analyses, we had the following exploratory research questions:
RQ 1a: Which moral dispositions predict compliance with COVID-19 preventive behaviors from a prior time point?
RQ 1b: Which moral dispositions predict moralization of non-compliance with COVID-19 preventive behaviors from a prior time point?
RQ 1c: What is the magnitude difference of effect sizes between emotional variable (Fear of COVID-19) and the Moral Measures?
RQ 2: Do moral dispositions from a prior time point predict intentions to vaccinate, or vaccine uptake when vaccines become available?
Methods
We conducted three online surveys with an international sample, where we measured both moral dispositions as well as COVID-19-specific behaviors from the same individuals. The first wave was collected in July 2019 before the beginning of the pandemic (originally for other purposes reported elsewhere; Laakasuo et al., Citation2021) and included only moral variables, meaning these measurements were not influenced by the pandemic. During the pandemic, we re-contacted the participants to collect responses to many of the same measures as well as COVID-19-related questions. Because of the opportunistic nature of data-collection, the initial sample size was based on the needs of the original research question (20 observations per Likert item). The original study as well as subsequent data-collections were pre-registered (for original 2019 wave, see https://osf.io/2v3fj, for waves 2–3, see https://osf.io/63gtw). We pre-registered the general research question, the measures collected, and the exclusion criteria. For deviations from formal pre-registration, see the transparent changes document in the latter OSF repository. The data and the analysis code are available at https://osf.io/ghxvw. We report all manipulations, measures, and exclusions in this study.Footnote1
Participants
In the first wave of data-collection in July 2019, 1043 participants (453 female, 490 male, 6 non-binary, 4 who did not want to state their gender) enrolled into an online study (on Qualtrics XM) via Prolific. A person was eligible to participate if they spoke English as their first language, resided in either Australia, Canada, Ireland, NZ, UK, or US, and did not have any ongoing long-term physical or mental illnesses (the latter two criteria included both to ensure a healthy sample for a psychological study and due to the study touching on themes related to death and suicide). A large majority of the sample consisted of participants from the UK (N = 694, 66%) and from the US (N = 335, 32%).Footnote2 The mean age of participants during the first wave was 37.29 (SD = 13.32). We contacted the same participants via Prolific in December 2020 and April 2021 for waves 2 and 3. We excluded participants based on set criteria (see below) in between each data-collection and did not re-contact any participants who were excluded in any of the previous waves. 622 participants responded in wave 2, and 597 in wave 3. Since we did not plan the current study in 2019, the sample size was based on the needs of the original study.
Data exclusions
In each wave, we excluded participants based on the same set of three criteria. First, we excluded participants who incorrectly answered more than one of the attention checks (“It is important that you pay attention during the study, please answer 5”) in any wave. Second, as an inattentive responding check we included two “demographic” items: “I make my own shoes” and “I make my own clothes.” We excluded participants who responded positively to both items.Footnote3 Third, we excluded participants who engaged in “straight-lining,” i.e., picking the same response on a Likert scale to each question on a scale. We first checked which scales each participant had straight-lined, and then computed the proportion of straight-lined responses. We excluded participants who had straight-lined over 50% of the survey. For wave 1, we also excluded participants who completed the study very quickly as per the original pre-registration. In total, 52 people were excluded (mean age = 32.45, 12 female, 38 male, 23 from US, 27 from UK, 1 from Ireland), leaving us the final sample size of 991. After exclusions, we had 991 responses from wave 1, 612 from wave 2, and 574 from wave 3 (). The moral measures (see below) did not predict drop-out in logistic regression, but younger age did predict the likelihood of dropping out (wave 2: OR = 0.58; wave 3: OR = 0.61).
Table 1. Participants in each wave and joint-wave.
Measures
Cronbach’s alphas for all multi-item measures used in the current study are presented in Appendix A. See the descriptive statistics in Appendix B.
Moral Foundations Questionnaire (waves 2 and 3)
The Moral Foundations Questionnaire (MFQ; Graham et al., Citation2011) measures the five moral foundations of Moral Foundations Theory: Care, Fairness, Loyalty, Authority, and Purity. The scale has 6 items for each subscale, totaling 30 items. The first 15 items consist of properties of actions and ask how morally relevant a participant finds them—e.g., “Whether or not someone suffered emotionally” (Care). Responses are given on a scale from 1 (“Not at all relevant”) to 7 (“Extremely relevant”). The second half asks participants to indicate their agreement with statements about their attitudes—e.g., “Compassion for those who are suffering is the most crucial virtue” (Care). Responses are given on a scale from 1 (“Strongly disagree”) to 7 (“Strongly agree”). For each foundation, we averaged the items from the two halves of the questionnaire to create an overall score. Higher scores indicate a higher relevance of a foundation.
Morality as Cooperation Questionnaire (waves 2 and 3)
The Morality as Cooperation Questionnaire (MAC-Q; Curry et al., Citation2019) measures the perceived moral relevance of seven different aspects of cooperation (as postulated by the scale developers). These are Family, Group, Reciprocity, Fairness, Property, Heroism and Deference. The scale has 6 items in each subscale, totaling 42 items. Like the MFQ, the questionnaire is split into two halves, the first assessing the relevance of different properties of actions to moral judgments (the evaluation facet), and the second assessing general attitudes corresponding to each aspect of cooperation (the judgment facet). All responses are given on a 7-point Likert scale: in the first half, 1 = “Not at all relevant” and 7 = “Extremely relevant”; in the second half 1 = “Strongly disagree” and 7 = “Strongly agree.” Example items for both halves from the Family subscale: “Whether or not someone acted to protect their family” and “You should always put the interests of your family first.” For each cooperation type, items from both halves were averaged. Higher scores indicate higher moral relevance of the aspect.
Moral Orientations Scale (waves 1–3)
The Moral Orientations Scale (MOS) measures four moral thinking styles: Integration, Deliberation, Sentiment, and Rule orientations. The validation information of this scale can be found in the supplemental material of Fleischmann et al. (Citation2019). The scale has a total of 28 items. Participants are asked to indicate their agreement on statements about their feelings and behaviors in ethically challenging situations on a 7-point Likert scale where 1 = “Strongly disagree” and 7 = “Strongly agree.” Example items from each subscale include: “When I think of people getting hurt it makes me upset” (Integration), “When thinking of ethical problems, I try to develop practical, workable alternatives” (Deliberation), “When making ethical decisions, I trust my heart to be my guide” (Sentiment), and “A person’s actions should be described in terms of being right or wrong” (Rule). Higher scores indicate a stronger orientation.
Oxford Utilitarianism Scale (waves 1–3)
The Oxford Utilitarianism Scale (OUS) was developed by Kahane et al. (Citation2018) to measure two aspects of utilitarianism. These are Impartial beneficence and Instrumental harm, which correspond to morally prescribing distributing good equally and altruistically, and morally prescribing harming people for the greater good, respectively. The scale has a total of 9 items for the subscales of instrumental harm and impartial beneficence. The scale asks participants to rate their agreement with statements about resolving several situations that involve saving another person’s life at a personal cost, on a 7-point Likert scale from 1 = “Strongly disagree” to 7 = “Strongly agree.” Example items include: “If the only way to save another person’s life during an emergency is to sacrifice one’s own leg, then one is morally required to make this sacrifice” (Impartial beneficence), and “It is morally right to harm an innocent person if harming them is a necessary means to helping several other innocent people” (Instrumental harm). Higher scores indicate higher endorsement of the belief measured by the subscale.
High-conflict moral dilemmas (waves 1–3)
The High-Conflict Moral Dilemmas (HCMDs) used in this study are a list of 12 dilemmas that pit utilitarian and deontological reasoning against each other from Koenigs et al. (Citation2007). HCMDs consistently form a unidimensional scale that is psychometrically valid (Laakasuo & Sundvall, Citation2016). In each dilemma, a participant is asked to imagine being in a scenario where they have to make a decision concerning other people’s lives. Each dilemma presents a participant with an option to sacrifice one person to save many others. Participants indicated how acceptable they would consider taking this course of action on a 7-point Likert scale where 1 = “Not acceptable at all” and 7 = “Totally acceptable.” Higher scores indicate higher preference for utilitarianism.
Fear of COVID-19 (waves 2 and 3)
The Fear of COVID-19 scale was developed to measure fear and anxiety toward the novel coronavirus (Ahorsu et al., Citation2022). The scale has 7 items, including, e.g., “When watching news and stories about the coronavirus on social media, I become nervous or anxious.” The questions are answered on a 5-point Likert scale from 1 = Strongly disagree to 5 = Strongly agree. Higher scores indicate greater fear toward COVID-19.
Dependent variable (DV): moralization of behavior during COVID-19 scale (waves 2 and 3)
This scale was adapted from a study by Francis and McNabb (Citation2020). The scale measures how morally wrong the respondent considers several violations of pandemic safety measures. Participants were presented with 16 brief scenarios with a target person engaging in such behaviors.Footnote4 Participants then indicated how wrong they considered the behavior on a 7-point Likert scale, where 1 = “Not wrong at all; a perfectly OK action” and 7 = “Very wrong; an extremely immoral action.” Example scenarios include “David is organizing and hosting a birthday meal at his local pub/bar” and “Ann throws a house party and invites many friends over.” Higher scores indicate higher moralization.
DV: measure of compliance (waves 2 and 3)
This set of questions was adapted from Francis and McNabb (Citation2020). This scale measures the extent the participants comply with behavioral guidelines to prevent the spread of COVID-19. The scale lists a set of preventive behaviors and asks participants which of the listed behaviors they were engaging in and how often. These behaviors include, e.g., proper hand-washing, avoiding crowded places, and using a mask in public places. The scale originally had 7 items, but we included an additional eighth item about mask use in both waves. Responses are given on a 5-point Likert scale, where 1 = “I never do this” and 5 = “I always do this.” Higher scores indicate higher (self-reported) compliance with behavioral recommendations.
DV: vaccination questions (waves 2 and 3)
In wave 2, participants rated their intention to take the COVID-19 vaccine when it becomes available to them using a 7-point Likert scale where 1 = “Extremely unlikely” and 7 = “Extremely likely.” In wave 3, participants were asked whether they have had access to the vaccine and whether they had taken it. We analyzed this DV only for the participants who indicated they have had access to the vaccine.
Data-analysis
We examined the predictive power of moral measures on compliance, moralization, and vaccination intention with multiple regressions, separately for each moral predictor. Moral predictors were always measured in the previous wave, and covariates from the current wave (same as the DV). For the dichotomous vaccine uptake question, we used logistic regression, using a subset of data in which participants had indicated that they had access to the vaccine (N = 303). We chose to analyze the predictors separately because this allowed us to compare the predictive power of the measures individually without the overlap between measures (see Appendix C) obscuring their relationships with the outcomes. Each of the moral measures was entered into the regression as a sole moral predictor along with the covariates outlined below to remove some potential confounds (see Appendix D for results with covariates only). We controlled for Fear of COVID-19, participants’ self-reported COVID-19 history, self-rated health, health problems and recent deaths in family, age, gender, nationality (UK/US/Other), employment status, income level, and political orientation on left/right and liberal/conservative axes. All numerical variables were standardized before the analyses, resulting in standardized regression coefficients.
Results
Standardized regression coefficients for moral predictors from their respective models are presented in . These represent the influence of each predictor on the dependent variable when control variables (see above) were included but other moral predictors were not. Our aim was to compare the predictive power of moral measures on COVID-19-related outcome variables.Footnote5
Table 2. Compliance and moralization results.
RQ 1a: Which moral dispositions predict compliance with COVID-19 preventive behaviors from a prior time point?
Wave 1 to wave 2
MOS Integration and Deliberation orientations predicted higher compliance (Integration: β = .11, Deliberation: β = .14; see ), which seems to imply that affective and moral reasoning and willingness to compromise in moral matters are related to compliance with behavioral restrictions.
Figure 1. Partial regression plots for compliance main results. Note. X-axis values are the residuals when regressing all other predictors against the scores of the moral measure; y-axis values are residuals when predicting DV with all covariates, but not the moral measure.
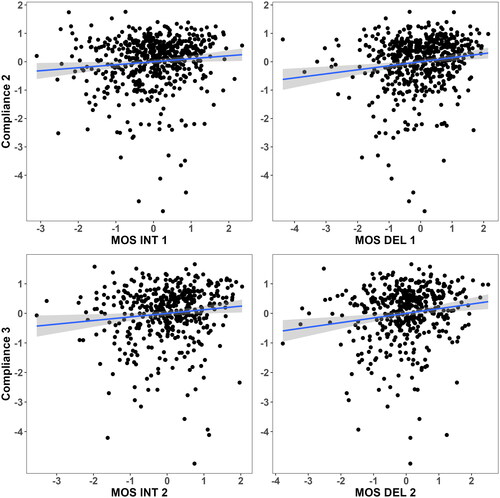
Wave 2 to wave 3
MOS Integration and Deliberation Orientations in wave 2 predicted compliance in wave 3 (Integration: β = .12; Deliberation: β = .16; see ) replicating the pattern above. Here, the Impartial Beneficence subscale of the OUS also predicted higher compliance (β = .11), suggesting a connection between pro-social moral reasoning and compliance—when the moral environment is held constant (i.e., there is an ongoing pandemic).
The MFQ and MAC-Q were first included in wave 2. Of the MFQ subscales, greater Care and Fairness foundations predicted higher Compliance (Care: β = .18; Fairness: β = .19), indicating that considerations of harm (avoidance) and equality are related to individuals more likely adopting these behaviors. The predictive power of the conservative “binding” foundations was very low for compliance (|βs| < .06); indicating that it is specifically these “individualizing” foundations that are associated with preventive behaviors. This is noteworthy because political orientation was controlled, implying that the effect of these moral values on compliance is not due to political divisions associated with moral foundations. Of the MAC-Q, the Family subscale had very low predictive power on compliance (β = .05) whereas all other subscales predicted it positively (all βs > .11). At face value, the results suggest that moral concerns about cooperation in general predicted compliance, but that concern for one’s kin was unrelated.
Measures of the instrumental harm aspect of utilitarianism (the HCMDs and OUS Instrumental Harm) did not predict compliance at any time point (|βs| < 0.01), suggesting that the “sacrificial” aspect of utilitarianism specifically does not promote preventive behaviors. The MOS Rule and Sentiment orientations also had low predictive power for compliance in all of the analyses (highest βs = .09), suggesting that neither a rigid rule-based approach nor a focus on empathy in moral reasoning were drivers of preventive behaviors.
RQ 1b: Which moral dispositions predict moralization of noncompliance with COVID-19 preventive behaviors from a prior time point?
Wave 1 to wave 2
Moralization toward noncompliance in wave 2 was predicted positively by OUS Impartial Beneficence (β = .11). This suggests that an altruistic and impartial concern for the well-being of everyone increased the moralization and condemnation of non-compliant actions. Utilitarian endorsements as measured using HCMDs (β = −.03) as well as utilitarian endorsements measured using OUS Instrumental Harm (β = −.07) had very low predictive power for moralization. Similarly to Compliance, MOS Integration and Deliberation orientations predicted greater moralization (Integration: β = .13; Deliberation: β = .09; see ). However, in contrast to the Compliance results, Moralization was also predicted positively by MOS Rule orientation (β = .13), implying that rule-based morality was associated with greater condemnation of noncompliance. Like with Compliance, MOS Sentiment orientation had a negligible effect on moralization (β = .06).
Figure 2. Partial regression plots for moralization main results. Note. X-axis values are the residuals when regressing all other predictors against the scores of the moral measures; y-axis values are residuals when predicting DV with all covariates, but not the moral measure.
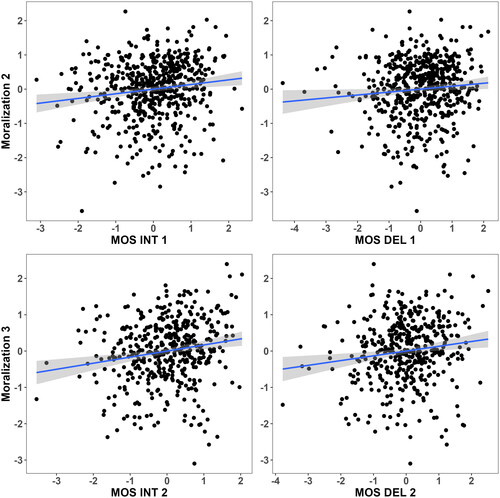
Wave 2 to wave 3
Neither of the instrumental harm measures (HCMDs and OUS Instrumental Harm) predicted Moralization well in wave 3 (HCMDs: β = .06; OUS IH: β = .06), but Impartial Beneficence aspect of utilitarianism was again associated with higher moralization (β = .22). Every MOS orientation predicted higher Moralization in wave 3 (βs > .11; see for Integration and Deliberation results), and the effects were slightly stronger than in wave 2. Of the MFQ, all of the subscales predicted higher Moralization, but the individualizing foundations (Care: β = .28; Fairness: β = .27) were stronger predictors than the binding foundations (Loyalty: β = .13; Authority: β = .14; Purity: β = .08. Given that individualizing foundations also predicted greater Compliance, they seem to be related to both action and the evaluation of others, while the binding foundations were more specific to evaluation. Additionally, all MAC-Q subscales predicted greater Moralization (βs > .15). Given that most MAC-Q subscales had high correlations with each other (see Appendix C), this could indicate that instead of different moral concerns for aspects of cooperation having specific effects, it could be that the subscales share a general aspect of “concern for cooperation” that would then be associated with the moralization of any given act.
RQ 2: Do moral dispositions from a prior time point predict intentions to vaccinate, or vaccine update when vaccines become available?
Vaccination intention
The only notable predictors of Vaccination intention were MOS Rule orientation (β = −.19) and MOS Sentiment orientation (β = −.09), which both predicted lower intention to vaccinate. Thus, approaches to moral thinking emphasizing established rules and approaches relying on emotions seem to be associated with a lower likelihood to consider vaccination.
Vaccine uptake
MOS Deliberation was the strongest predictor of vaccine uptake when controlling for covariates (OR = 1.58). This measure was also a positive predictor of Compliance in both waves 2 and 3. It is indirectly associated with utilitarianism, which fits with it predicting an arguably utilitarian action. However, pre-pandemic utilitarianism did not predict self-reported behaviors before the moral context changed. The majority of other predictors had an OR close to 1, with the most notable exceptions being the both OUS utilitarian scales, the Fairness aspects of both MFQ and MAC, and MOS Rule orientation (negative predictor) ().
Table 3. Vaccination results.
Covariates (RQ 1c)
The majority of our covariates had no effect on any dependent variable or had inconsistent effects across time points. The one notable exception to this was the Fear of COVID-19 measure, which was positively associated with each dependent variable on all time-points (see Appendix D). In a majority of the models, it had a larger effect size than the main predictor of the model. Due to the politically divisive nature of the DVs, we also ran exploratory moderation analyses where we included an interaction between the moral predictors and left-right political orientation. The results are presented in Appendix F.
Discussion
The COVID-19 pandemic provided a context in which to test how significant changes in people’s moral environments are associated with their moral convictions and preferences as well as actual behaviors that have moral relevance. Overall, we found that several measures modestly predicted COVID-19 related behaviors on the subsequent time-point. Surprisingly it was MOS Integration and Deliberation that were predictive of Moralization and Compliance across different timepoints, whether the moral environment had just changed or remained constant. Both of these measures are measures of mature and nuanced thinking that focus on capacity to balance and take into consideration multiple viewpoints. We will discuss these in more detail below.
Moral orientations
As stated above, the most consistent predictors in our models were the moral orientations of Integration and Deliberation, which predicted both compliance and moralization—these measures were predictive of behaviors across changing moral environments of prior-to-during COVID-19 pandemic. Integration orientation is described as a characteristic of “mature” moral thinking with affective and cognitive factors (see Fleischmann et al., Citation2019). Since Integration orientation predicts empathic concern as well as charitable behavior (Fleischmann et al., Citation2019), it seems logical that it predicts prosocial behavior and the moralization of actions that fail to protect others. The fact that a moral psychological measure can function consistently and reliably in changing moral environments is a strength of the measure and should perhaps influence future researchers’ decision-making when selecting instruments for their studies.
Deliberation orientation also predicted compliance and moralization in both waves after controlling for all covariates and was the strongest (positive) predictor of vaccine uptake. Deliberation orientation has been shown to predict utilitarian but not deontological decision-making and a focus on outcomes but not empathic concern (Fleischmann et al., Citation2019). Considering the implicit or explicit utilitarian rationale behind behavioral restrictions, it seems reasonable that an orientation that aligns well with utilitarian thinking would predict compliance with the restrictions, as well as actual vaccine uptake. However, other measures of results-focused and non-empathic utilitarian thinking—the High-Conflict Moral Dilemmas or the Instrumental harm subfactor of the OUS—did not predict compliance at any point in our analyses (see below). Thus, Deliberation orientation may predict both results-focused thinking (Fleischmann et al., Citation2019) and compliance, but the association from Deliberation orientation to Compliance is not necessarily driven by results-focused thinking only. But again, the fact that the Deliberation orientation actually measures a stable disposition of values that sensibly predict human behavior in a changing moral environment is something to recognize and should matter for future research.
Rule orientation was only consistently associated with Moralization and was a negative predictor of Vaccine intentions and to some extent a negative predictor of Vaccine uptake. High rule orientation indicates cognitive rigidity and dogmatic aversion to moral rule breaking and rejection of outcome maximization (Fleischmann et al., Citation2019). Our study implies that Rule orientation is more strongly associated with condemning others for breaking rules, even novel ones, than oneself following them. It could be that the aversion toward results-maximization associated with rule orientation would explain some of these results. However, both Rule and Deliberation orientations were positive predictors of moralization at wave 3, but have opposite associations with results-oriented thinking. Thus, it is unclear whether preferences about results-maximization explain one or the other result, but logically, they cannot explain both. Nonetheless, the fact that Rule orientation, too, systematically predicts at least the need to watch and enforce rules on others, despite the changes in a changing moral environment, is an encouraging finding. This finding also fits with existing evolutionary psychology models of moral cognition, which suggest that people strategically use moral norms and rules to influence others and to gain power and control over others by forming alliances (e.g., Kurzban, Citation2010).
Finally, Sentiment orientation was a positive predictor of Moralization in wave 3 as well as negative predictor of Vaccination intention in wave 2. Fleischmann et al. (Citation2019) describe Sentiment orientation as an approach to moral decision-making characterized by an “uncritical reliance” on affect over deliberation. Sentiment orientation is positively associated with empathic concern but negatively associated with utilitarian preferences. It seems sensible that an empathy-focused way of moral thinking would predict the Moralization of noncompliance with behaviors that are designed to protect other people. However, it is less obvious why this association is not found across time points. It is possible that some moral orientations are more dynamic in their nature; when the moral environment changes, their functioning changes. Given that emotions are highly context dependent, it makes sense that sentiment orientation would function more reactively than the other moral orientations. That is, Sentiment orientation measured before the pandemic may have not predicted Moralization and Compliance because people had not yet had enough time to have emotional experiences concerning COVID-19. The negative association between Sentiment orientation and Vaccine intention could, similarly, reflect an initial negative reaction to vaccination that was reduced later on, since Sentiment only modestly negatively predicted vaccine uptake.
Utilitarian preferences
Impartial Beneficence predicted Moralization positively across changing moral environments (W1 vs. W2) and even when the moral environment was constant (W2 vs. W3). It also predicted Compliance with behavioral recommendations but in wave 3 only. Put in the context of the pandemic, this measure of concern for people outside one’s own group positively predicted following guidelines. This suggests that moral judgments might be more influenced by a broader concern for well-being rather than a “calculative” utilitarian approach. To corroborate this finding, future research could incorporate additional measures like Dark Tetraed (Međedović & Petrović, Citation2015) or Dark Triad (Jones & Paulhus, Citation2014).
Critically, Impartial Beneficence was the only utilitarian metric that predicted our dependent variables. We found that neither following COVID-19 restrictions nor judging those who break them were linked to a utilitarian view that justifies harm for a greater good (Instrumental harm; Francis & McNabb, Citation2020; Kneer & Hannikainen, Citation2022), aligning with previous research on utilitarianism and the pandemic. One reason for this discrepancy could be that our measures, like the Instrumental harm subscale of the OUS and High-Conflict Moral Dilemmas, are not designed to predict real-world actions but rather to understand moral cognition (Christensen & Gomila, Citation2012; Francis & McNabb, Citation2020).
A common criticism of these measures is that they may not be reliable or they could be sensitive to the presence or lack of affective states (Bartels & Pizarro, Citation2011; Patil et al., Citation2014; though see Paruzel-Czachura & Farny, Citation2023). People might score high for different reasons: some could be making careful ethical calculations and others might simply be less emotional about causing harm. Therefore, these measures might not be reliable for understanding moral attitudes in real-world pandemic situations.
Moral foundations and types of cooperation
With respect to Moral Foundations Questionnaire (MFQ) and Morality as Cooperation Questionnaire (MAC-Q), which were only measured when the moral environment stayed relatively constant, we found that all of them predicted COVID-19 related moralization (RQ1B). With respect to Compliance (RQ1A), we found that MFQ Care and Fairness were relevant as well as all of the MAC-Q scales.
Moral Foundations Questionnaire and Morality as Cooperation Scales were included in our data collection efforts only from Wave 2 onwards and thus, they are only informative of behaviors, when the moral environment stays constant. Nonetheless, each moral foundation was a positive predictor of Moralization (RQ1B), though effect sizes were the largest for Care and Fairness. These two were also the MFQ foundations that emerged as the strongest positive predictors of Compliance (RQ1A). Thus, it seems that the individualizing (Care, Fairness) foundations predicted both self-reported behavior and moral judgment of others, while the binding (Loyalty and Authority) foundations only predicted the latter. Fairness considerations are associated with reciprocal altruism, while the Care foundation is associated with virtues of kindness and aversion to the pain of others (Graham et al., Citation2011). Thus, it seems logical that a higher emphasis on Fairness would predict both altruistic behavior and condemnation of those who refuse to behave altruistically, and that a higher emphasis on Care would predict both the avoidance of behavior that could harm others as well as the condemnation of such behavior.
Indeed, the justifications of the mandates and recommendations were often utilitarian, with the stated outcomes of preventive behaviors being aggregate welfare—protecting oneself and others from a disease and its associated risks. Thus, the rationale behind preventive behaviors matched conceptually with the Fairness and Care foundations: everyone must do their part to prevent harm. Meanwhile, the correspondence with the other foundations was less direct. The Loyalty foundation is concerned with loyalty to one’s ingroup, while the behaviors we measured were explicitly about protecting people regardless of their group affiliation. Further, the Authority foundation is concerned with deference to legitimate authority and traditions, leaving room for individual differences in the current context: people’s compliance with recommended behaviors could be dependent on whether they agree with the authorities’ moral rationale to begin with.
Each MAC-Q subscale predicted moralization positively, and each subscale also predicted compliance positively (RQ1AB), though, for the Family subscale, this predictive power was very low. The Fairness subscale was the strongest MAC-Q predictor for both of our dependent variables, similar to the Fairness foundation of the MFQ. While the MAC-Q results match with the MFQ results in terms of Fairness being the strongest predictor, it seems that the MAC-Q overall predicted compliance better than the MFQ, implying that the scope of MFQ is wider. As the MAC-Q is intended to measure how much people emphasize different aspects of cooperation in their moral judgments, it could be that each subscale also measures aspects of cooperativeness. Given the rationale of preventive behaviors as a collaborative effort to prevent harm, it makes sense that even an indirect measure of cooperativeness would predict those behaviors.
Main results in comparison to affective processes
The Fear of COVID-19 covariate was also a consistent strong predictor of compliance, moralization, and both Vaccine intention and uptake, which aligns well with findings by Russell et al. (Citation2023), who found affective states (including fear) to predict compliance with restrictions. Our results show that moral measures, collected before the change in the moral environment, can predict pandemic-related behavior, but their effect sizes are modest in contrast to acute affective states (RQ1C).
Summary
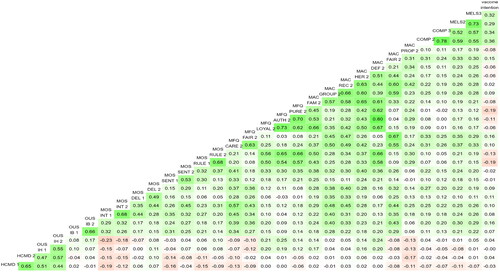
The measures that predicted higher Compliance and Moralization at the change of the moral environment—and when the change in the moral environment persisted—were MOS Integration and Deliberation. In addition, Impartial Beneficence predicted Moralization, when the moral environment changed—and when the change persisted. As is evident from our correlation matrix (Appendix C) these measures are relatively independent of each other; which means that there is no single moral psychological mechanism or factor that would explain all of these phenomena in an economic way. It seems safe to assume that all of these moral judgment mechanisms add up to different moral behaviors. Indeed, moral judgments and moral actions are more complicated than just emotional reactions, since the results persist even after controlling for Fear of COVID-19.
When the moral environment stays constant (W2 vs. W3) there were unifying themes: fairness (MFQ Fairness foundation; MAC-Q Fairness subscale) and concern for the well-being of others (MFQ Care foundation), and cooperation (MAC-Q in general) had the strongest associations with compliance and moralization, respectively. The measures that did not predict compliance, or predicted it much less, were also varied, but can be roughly categorized as opposing the use of other people as means to an end (HCMDs and OUS Instrumental Harm), favoring the in-group (MFQ Loyalty foundation; MAC-Q Family subscale), conservative moral values (MFQ Authority and Purity foundations), and moral thought characterized by avoiding deliberation (MOS Rule and Sentiment orientations).
In general, there were more predictors of moralization than of compliance. Additionally, very few moral measures had good predictive power for intentions to vaccinate or vaccine uptake. The results suggest that moral measures more reliably predict an individual’s attitudes toward the behavior of others in a novel context than the individual’s own behavior; which is in alignment with Descioli-Kurzban’s model of morality as in-group coordination to protect one’s inclusive fitness (DeScioli & Kurzban, Citation2013, Citation2018).
Limitations
Like many longitudinal studies, our study had notable attrition, with 48% of the participants providing data for all of the waves, although the data still remain sizable. While the sample was international, we must note that participants were all from English-speaking WEIRD (Henrich et al., Citation2010) countries, limiting the generalizability. Also, due to the opportunistic nature of the data collection, the initial materials were not planned for investigating COVID-19 related topics. For example, we decided to include MFQ and MAC starting from wave 2 and were unable to examine how their pre-pandemic levels are associated with pandemic behavior—with these measures we can only estimate their functioning in a situation where the moral environment stays constant. Perhaps, once the pandemic times are completely over, their effectiveness in a changed moral environment can be evaluated. Naturally, since there are several predictive variables, it is likely that some associations could be spurious correlations. However, this concern is mitigated by the fact that many of our variables behave in a logical manner across timepoints.
Conclusions
In a two-year longitudinal study—unique in the sense that data collection was started before the COVID-19 pandemic—we found several moral dispositions to prospectively predict Compliance with behavioral restrictions during the COVID-19 pandemic or moralization of noncompliance with those restrictions. This is a unique study that offers a window into examining the relative strengths of the most common moral psychological measures in a situation where the moral environment changes and allows us to compare their effect sizes with a more acute emotional measure of fear. It seems that the moral orientations of Integration and Deliberation, characterized as mature moral thinking, deserve more attention from the scientific community than they have thus far garnered. Moreover, some moral dispositions predicted the intention to vaccinate and vaccine uptake. Moral measures related to pro-sociality, impartiality, and compromise-seeking were the most consistent predictors of compliance, while moralization of noncompliance was associated with a wider range of moral measures. The results in general seem to point to the predictive power as well as to societal and political relevance of moral psychological measures when people face real-world moral problems.
Ethical approval
The study was approved by Research Ethics Committee in the Humanities and Social and Behavioral Sciences of University of Helsinki (statement 28/2019).
Author contributions
Anton Kunnari: conceptualization, investigation, formal analysis, data curation, writing–original draft, writing–review and editing; Kathryn Francis: conceptualization, methodology, resources, writing–review and editing; funding acquisition; Jukka Sundvall: conceptualization, investigation, formal analysis, writing–original draft, writing–review and editing; Michael Laakasuo: conceptualization, formal analysis, investigation, resources, project administration, writing–original, writing–review and editing, supervision, funding acquisition.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data and analysis scripts are available in an OSF repository: https://osf.io/ghxvw.
Additional information
Funding
Notes
1 Because we use a subset of a larger project data that concern the research questions of the current paper, listing all of the collected variables would be unfeasible, and thus we refer the reader to the OSF materials for the measures that fall outside the scope of this paper.
2 Australia: N = 7 (<1%), Ireland: N = 14 (<1%), Other countries: N = 3 (<1%). Participants were contacted and their data were used in the analyses regardless of their nationality, though the participants from countries other than UK and US were collapsed into an “Other” category in the nationality covariate.
3 This exclusion criterion is based on the reasoning that a participant who claims to both make their own shoes and their own clothes is more likely to be a participant clicking on the first option for each item as quickly as possible rather than a skilled professional or amateur tailor and shoemaker.
4 We dropped four scenarios included in the original battery of Francis and McNabb (Citation2020) from the analysis because we wanted to focus on moralization toward non-compliance, whereas these items concerned other kinds of non-altruistic behavior.
5 We also ran models where we included all moral predictors at once along with the covariates to see the relative unique contributions of the predictors. These models are presented in Appendix E.
References
- Ahorsu, D. K., Lin, C. Y., Imani, V., Saffari, M., Griffiths, M. D., & Pakpour, A. H. (2022). The Fear of COVID-19 scale: Development and initial validation. International Journal of Mental Health and Addiction, 20(3), 1537–1545. https://doi.org/10.1007/s11469-020-00270-8
- Bartels, D. M., & Pizarro, D. A. (2011). The mismeasure of morals: Antisocial personality traits predict utilitarian responses to moral dilemmas. Cognition, 121(1), 154–161. https://doi.org/10.1016/j.cognition.2011.05.010
- Bor, A., Jørgensen, F., Lindholt, M. F., & Petersen, M. B. (2023). Moralizing the COVID-19 pandemic: Self-interest predicts moral condemnation of other’s compliance, distancing, and vaccination. Political Psychology, 44, 257–279. https://doi.org/10.1111/pops.12835
- Chan, E. Y. (2021). Moral foundations underlying behavioral compliance during the COVID-19 pandemic. Personality and Individual Differences, 171, 110463. https://doi.org/10.1016/j.paid.2020.110463
- Christensen, J. F., & Gomila, A. (2012). Moral dilemmas in cognitive neuroscience of moral decision-making: A principled review. Neuroscience and Biobehavioral Reviews, 36(4), 1249–1264. https://doi.org/10.1016/j.neubiorev.2012.02.008
- Christner, N., Sticker, R. M., Söldner, L., Mammen, M., & Paulus, M. (2020). Prevention for oneself or others? Psychological and social factors that explain social distancing during the COVID-19 pandemic. Journal of Health Psychology, 27(6), 1342–1353. https://doi.org/10.1177/1359105320980793
- Curry, O. S., Jones Chesters, M., & Van Lissa, C. J. (2019). Mapping morality with a compass: Testing the theory of ‘morality-as-cooperation’ with a new questionnaire. Journal of Research in Personality, 78, 106–124. https://doi.org/10.1016/j.jrp.2018.10.008
- De Corte, K., Cairns, J., & Grieve, R. (2021). Stated versus revealed preferences: An approach to reduce bias. Health Economics, 30(5), 1095–1123. https://doi.org/10.1002/hec.4246
- DeScioli, P., & Kurzban, R. (2013). A solution to the mysteries of morality. Psychological Bulletin, 139(2), 477–496. https://doi.org/10.1037/a0029065
- DeScioli, P., & Kurzban, R. (2018). Morality is for choosing sides. In K. Gray & J. Graham (Eds.), Atlas of moral psychology (pp. 177–185). Guildford Press.
- Fleischmann, A., Lammers, J., Conway, P., & Galinsky, A. D. (2019). Paradoxical effects of power on moral thinking: Why power both increases and decreases deontological and utilitarian moral decisions. Social Psychological and Personality Science, 10(1), 110–120. https://doi.org/10.1177/1948550617744022
- Frackowiak, M., Russell, P. S., Rusconi, P., Fasoli, F., & Cohen-Chen, S. (2023). Political orientation, trust and discriminatory beliefs during the COVID-19 pandemic: Longitudinal evidence from the United Kingdom. The British Journal of Social Psychology, 62(4), 1897–1924. https://doi.org/10.1111/bjso.12662
- Francis, K., & McNabb, C. B. (2020). Moral decision-making during COVID-19: Moral judgments, moralisation, and everyday behaviour [Preprint]. Open Science Framework. https://doi.org/10.31219/osf.io/jvfds
- Frowde, R., Dove, E. S., & Laurie, G. T. (2020). Fail to prepare and you prepare to fail: The human rights consequences of the UK government’s inaction during the COVID-19 pandemic. Asian Bioethics Review, 12(4), 459–480. https://doi.org/10.1007/s41649-020-00151-1
- Gerbaudo, P. (2020). The pandemic crowd. Journal of International Affairs, 73(2), 61–76.
- Graham, J., Haidt, J., Koleva, S., Motyl, M., Iyer, R., Wojcik, S. P., & Ditto, P. H. (2013). Chapter two – Moral foundations theory: The pragmatic validity of moral pluralism. In P. Devine & A. Plant (Eds.), Advances in experimental social psychology (Vol. 47, pp. 55–130). Academic Press. https://doi.org/10.1016/B978-0-12-407236-7.00002-4
- Graham, J., Nosek, B. A., Haidt, J., Iyer, R., Koleva, S., & Ditto, P. H. (2011). Mapping the moral domain. Journal of Personality and Social Psychology, 101(2), 366–385. https://doi.org/10.1037/a0021847
- Haischer, M. H., Beilfuss, R., Hart, M. R., Opielinski, L., Wrucke, D., Zirgaitis, G., Uhrich, T. D., & Hunter, S. K. (2020). Who is wearing a mask? Gender-, age-, and location-related differences during the COVID-19 pandemic. PLOS One, 15(10), e0240785. https://doi.org/10.1371/journal.pone.0240785
- Halpern, L. W. (2020). The politicization of COVID-19. The American Journal of Nursing, 120(11), 19–20. https://doi.org/10.1097/01.NAJ.0000721912.74581.d7
- Han, Q., Zheng, B., Cristea, M., Agostini, M., Bélanger, J. J., Gützkow, B., Kreienkamp, J., Leander, N. P., & PsyCorona Collaboration (2023). Trust in government regarding COVID-19 and its associations with preventive health behaviour and prosocial behaviour during the pandemic: A cross-sectional and longitudinal study. Psychological Medicine, 53(1), 149–159. https://doi.org/10.1017/S0033291721001306
- Henrich, J., Heine, S., & Norenzayan, A. (2010). The weirdest people in the world? The Behavioral and Brain Sciences, 33(2–3), 61–83. https://doi.org/10.1017/S0140525X0999152X
- Jones, D. N., & Paulhus, D. L. (2014). Introducing the Short Dark Triad (SD3): A brief measure of dark personality traits. Assessment, 21(1), 28–41. https://doi.org/10.1177/1073191113514105
- Kahane, G., Everett, J. A. C., Earp, B. D., Caviola, L., Faber, N. S., Crockett, M. J., & Savulescu, J. (2018). Beyond sacrificial harm: A two-dimensional model of utilitarian psychology. Psychological Review, 125(2), 131–164. https://doi.org/10.1037/rev0000093
- Kerr, J., Panagopoulos, C., & van der Linden, S. (2021). Political polarization on COVID-19 pandemic response in the United States. Personality and Individual Differences, 179, 110892. https://doi.org/10.1016/j.paid.2021.110892
- Kneer, M., & Hannikainen, I. R. (2022). Trolleys, triage and Covid-19: The role of psychological realism in sacrificial dilemmas. Cognition & Emotion, 36(1), 137–153. https://doi.org/10.1080/02699931.2021.1964940
- Koenigs, M., Young, L., Adolphs, R., Tranel, D., Cushman, F., Hauser, M., & Damasio, A. (2007). Damage to the prefrontal cortex increases utilitarian moral judgements. Nature, 446(7138), 908–911. https://doi.org/10.1038/nature05631
- Kurzban, R. (2010). Why everyone (else) is a hypocrite: Evolution and the modular mind. Princeton University Press.
- Laakasuo, M., Repo, M., Drosinou, M., Berg, A., Kunnari, A., Koverola, M., & Sundvall, J. (2021). The dark path to eternal life: Machiavellianism predicts approval of mind upload technology. Personality and Individual Differences, 177, 110731. https://doi.org/10.1016/j.paid.2021.110731
- Laakasuo, M., & Sundvall, J. (2016). Are utilitarian/deontological preferences unidimensional? Frontiers in Psychology, 7, 1228. https://doi.org/10.3389/fpsyg.2016.01228
- Laakasuo, M., Köbis, N., Palomäki, J., & Jokela, M. (2018). Money for microbes—Pathogen avoidance and out‐group helping behaviour. International Journal of Psychology, 53(S1), 1–10. https://doi.org/10.1002/ijop.12416
- Laakasuo, M., Sundvall, J., & Drosinou, M. (2017). Individual differences in moral disgust do not predict utilitarian judgments, sexual and pathogen disgust do. Scientific Reports, 7(1), 45526. https://doi.org/10.1038/srep45526
- Međedović, J., & Petrović, B. (2015). The dark tetrad. Journal of Individual Differences, 36(4), 228–236. https://doi.org/10.1027/1614-0001/a000179
- Motta, M., Stecula, D., & Farhart, C. (2020). How right-leaning media coverage of COVID-19 facilitated the spread of misinformation in the early stages of the pandemic in the U.S. Canadian Journal of Political Science, 53(2), 335–342. https://doi.org/10.1017/S0008423920000396
- Murphy, K., Williamson, H., Sargeant, E., & McCarthy, M. (2020). Why people comply with COVID-19 social distancing restrictions: Self-interest or duty? Australian & New Zealand Journal of Criminology, 53(4), 477–496. https://doi.org/10.1177/0004865820954484
- O’Connell, K., Berluti, K., Rhoads, S. A., & Marsh, A. A. (2021). Reduced social distancing early in the COVID-19 pandemic is associated with antisocial behaviors in an online United States sample. PLOS One, 16(1), e0244974. https://doi.org/10.1371/journal.pone.0244974
- Olivera-La Rosa, A., Chuquichambi, E. G., & Ingram, G. P. D. (2020). Keep your (social) distance: Pathogen concerns and social perception in the time of COVID-19. Personality and Individual Differences, 166, 110200. https://doi.org/10.1016/j.paid.2020.110200
- Paruzel-Czachura, M., & Farny, Z. (2023). Psychopathic traits and utilitarian moral judgment revisited. Personality & Social Psychology Bulletin, 1461672231169105. https://doi.org/10.1177/01461672231169105
- Patil, I., Cogoni, C., Zangrando, N., Chittaro, L., & Silani, G. (2014). Affective basis of judgment-behavior discrepancy in virtual experiences of moral dilemmas. Social Neuroscience, 9(1), 94–107. https://doi.org/10.1080/17470919.2013.870091
- Pfattheicher, S., Nockur, L., Böhm, R., Sassenrath, C., & Petersen, M. B. (2020). The emotional path to action: Empathy promotes physical distancing and wearing of face masks during the COVID-19 pandemic [Preprint]. PsyArXiv. https://doi.org/10.31234/osf.io/y2cg5
- Prosser, A. M. B., Judge, M., Bolderdijk, J. W., Blackwood, L., & Kurz, T. (2020). Distancers’ and ‘non‐distancers’? The potential social psychological impact of moralizing COVID‐19 mitigating practices on sustained behaviour change. The British Journal of Social Psychology, 59(3), 653–662. https://doi.org/10.1111/bjso.1239
- Rosenfeld, D. L., & Tomiyama, A. J. (2022). Jab my arm, not my morality: Perceived moral reproach as a barrier to COVID-19 vaccine uptake. Social Science & Medicine, 294, 114699. https://doi.org/10.1016/j.socscimed.2022.114699
- Rozin, P. (1999). The process of moralization. Psychological Science, 10(3), 218–221. https://doi.org/10.1111/1467-9280.00139
- Russell, P. S., Frackowiak, M., Cohen-Chen, S., Rusconi, P., & Fasoli, F. (2023). Induced gratitude and hope, and experienced fear, but not experienced disgust, facilitate COVID-19 prevention. Cognition & Emotion, 37(2), 196–219. https://doi.org/10.1080/02699931.2022.2157377
- Shanka, M. S., & Menebo, M. M. (2022). When and how trust in government leads to compliance with COVID-19 precautionary measures. Journal of Business Research, 139, 1275–1283. https://doi.org/10.1016/j.jbusres.2021.10.036
- Stevenson, C., Wakefield, J. R. H., Felsner, I., Drury, J., & Costa, S. (2021). Collectively coping with coronavirus: Local community identification predicts giving support and lockdown adherence during the COVID-19 pandemic. The British Journal of Social Psychology, 60(4), 1403–1418. https://doi.org/10.1111/bjso.12457
- Stroebe, W., vanDellen, M. R., Abakoumkin, G., Lemay, E. P., Schiavone, W. M., Agostini, M., Bélanger, J. J., Gützkow, B., Kreienkamp, J., Reitsema, A. M., Abdul Khaiyom, J. H., Ahmedi, V., Akkas, H., Almenara, C. A., Atta, M., Bagci, S. C., Basel, S., Berisha Kida, E., Bernardo, A. B. I., … Leander, N. P. (2021). Politicization of COVID-19 health-protective behaviors in the United States: Longitudinal and cross-national evidence. PLOS One, 16(10), e0256740. https://doi.org/10.1371/journal.pone.0256740
- Vacchini, S., Fasoli, F., & Volpato, C. (2021). “You cannot get into my taxi!” Perceptions of a COVID-19-based rejection episode reported in the newspapers. Journal of Language and Social Psychology, 40(5–6), 677–689. https://doi.org/10.1177/0261927X211043096
- Van Bavel, J. J., Cichocka, A., Capraro, V., Sjåstad, H., Nezlek, J. B., Pavlović, T., Alfano, M., Gelfand, M. J., Azevedo, F., Birtel, M. D., Cislak, A., Lockwood, P. L., Ross, R. M., Abts, K., Agadullina, E., Aruta, J. J. B., Besharati, S. N., Bor, A., Choma, B. L., … Boggio, P. S. (2022). National identity predicts public health support during a global pandemic. Nature Communications, 13(1), 517. https://doi.org/10.1038/s41467-021-27668-9
- Vartanova, I., Eriksson, K., Kirgil, Z. M., & Strimling, P. (2021). The advent of the COVID-19 epidemic did not affect Americans’ endorsement of moral foundations. Frontiers in Psychology, 12, 647858. https://doi.org/10.3389/fpsyg.2021.647858
- World Health Organization (2020). Advice for the public: Coronavirus disease (COVID-19). https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public
- Zhou, H., Cárdenas, D., & Reynolds, K. J. (2023). Norms and COVID‐19 health behaviours: A longitudinal investigation of group factors. European Journal of Social Psychology, 53(4), 720–731. https://doi.org/10.1002/ejsp.2932
Appendix A.
Reliabilities of the measures used.
Table A1. Cronbach’s alphas.
Appendix B.
Descriptive statistics of the measures used.
Table B1. Means and SDs of the main variables.
Appendix C.
Correlations between variables.
Figure C1. Correlation matrix of the main variables.
Appendix D.
Multiple regression results for covariates only.
Table D1. Multiple regression results.
Appendix E.
Models including all moral predictors simultaneously.
For each DV, we entered all moral variables as predictors simultaneously along with covariates to check their unique contributions. MOS Deliberation was the only (positive) predictor for Compliance in wave 2, partially aligning with the main results. Wave 3 compliance was predicted negatively by MFQ Authority and Purity foundations, and positively by MAC deference. Moralization was not predicted by any moral measure in wave 2, but in wave 3 was predicted positively by OUS impartial beneficence and MFQ Care and Fairness foundations. Vaccine intention was predicted positively by MOS Deliberation orientation and negatively by Rule orientation, and actual vaccine uptake negatively by MOS rule orientation and positively by MAC deference.
Table E1. Full models with all moral predictors.
Appendix F.
Exploratory moderation analyses.
We conducted exploratory moderation analyses to examine whether political orientation influenced the predictive power of the moral measures. The analyses were otherwise similar to the main analyses, with separate models for all moral predictors, but an interaction term between the predictor and left-right political orientation (standardized) was added. In wave 2, political orientation moderated instrumental harm aspect of utilitarianism for both compliance and moralization, with stronger effect for more right-wing participants. Likewise, MOS sentiment orientation was more strongly associated with vaccination intention the more right-wing the participant was. The only effect political orientation moderated in wave 3 was between MOS sentiment and compliance, with stronger positive effects of compliance the more
Table F1. Moderation of political orientation (left-right) with moral predictors.