
ABSTRACT
Being able to empathise with others is a crucial ability in everyday life. However, this does not usually entail feeling the pain of others in our own bodies. For individuals with mirror-sensory synaesthesia (MSS), however, this form of empathic embodiment is a common feature. Our study investigates the empathic ability of adults who experience MSS using a video-based empathy task. We found that MSS participants did not differ from controls on emotion identification and affective empathy; however, they showed higher affect sharing (degree to which their affect matches what they attribute to others) than controls. This finding indicates difficulties with self-other distinction, which our data shows results in fewer signs of prosocial behaviour. Our findings are in line with the self-other control theory of MSS and highlight how the use of appropriate empathy measures can contribute to our understanding of this important socio-affective ability, both in typical and atypical populations.
Introduction
Is it possible to feel too much empathy? Although the ability to empathize with others is crucial for our everyday social interactions, for most of us, being empathic does not involve feeling the other person’s pain in our own bodies. This form of empathic embodiment, however, seems a common feature in individuals with mirror-sensory synaesthesia (e.g., Fitzgibbon et al., Citation2012; henceforth abbreviated to MSS). MSS encompasses experiences of mirror-touch synaesthesia (MTS)—the tactile experience in own body when observing another person being touched (Ward & Banissy, Citation2015) and mirror-pain synaesthesia (MPS)—the experience of noxious stimulation in the perceiver’s body when observing another person in pain (Giummarra & Bradshaw, Citation2009; Grice-Jackson et al., Citation2017). For individuals with MSS, the noxious or tactile synaesthetic experience appears to happen involuntarily. For example, Martin et al. (Citation2017, p. 220) quote the following from an interview excerpt with an MTS participant:
I feel an overall physical manifestation of the emotion of another person because I feel those physical manifestations. I feel there is an automatic backflow of that information that goes to my brain from the physical sensation that pulls up those emotions in me; it’s not so much a deliberate process as it is an automatic process … If I’m around someone whose emotional experience is very strong, and I’m around them for a sustained period of time, it gets to a point where I am unable to keep the volume down actively enough … (participant 3)
Consistent with this description, previous research has found that compared to controls, individuals with MTS report a higher level of affective empathy—the degree to which the affective state of another causes a matching state on self (Bird & Viding, Citation2014; Coll et al., Citation2017)—when responding to self-report questionnaires (e.g., Banissy & Ward, Citation2007; Ward et al., Citation2018). It has also been found that individuals with MTS show a greater ability to identify facial expressions of emotion (Banissy et al., Citation2011; Ward et al., Citation2018). Similarly, research with mirror-pain synaesthetes—often referred to as vicarious pain responders in the literature—also suggests enhanced empathy for these individuals. Botan et al. (Citation2018) used a Vicarious Pain Questionnaire—consisting of 16 brief videos showing people experiencing a range of physical pain such as sports injuries, falls and injections to classify pain responders into three groups: non-responders (participants who report no pain when seeing others experiencing pain), sensory-localized responders (those who report feeling localized pain using sensory descriptors), and affective-general responders (those who report a more generalized feeling of pain and use affective descriptors). Botan and colleagues found that both groups of pain responders report greater affective empathy and pro-social/helping attitudes than controls.
In addition to self-reported experiences, neuroimaging data show that when observing pain in others, individuals with MSS display brain activity not only in primary and secondary somatosensory cortices (SI, SII) but also in neural networks of empathy for pain, such as anterior cingulate cortex (ACC), anterior insula (AI) and supplementary motor areas (SMA)—e.g., Grice-Jackson et al. (Citation2017); Osborn and Derbyshire (Citation2010). These findings suggest that people with MSS experience both the sensory and affective components of pain when observing pain in others.
However, research findings on empathy in MSS do not always support the view that these individuals experience enhanced empathic abilities compared to controls. Baron-Cohen et al. (Citation2016) compared a self-report sample of individuals with MTS, a grapheme-colour (GC) synaesthesia group and a control group using a range of measures. They found no evidence of enhanced empathy in the MTS group compared to the other two groups. Furthermore, the researchers report that the only group difference in the Empathy Quotient questionnaire (EQ—Baron-Cohen & Wheelwright, Citation2004) was in the social skills sub-scale, in which the MTS group had lower scores than both, the GC synaesthetes and the neurotypical controls. The same study also showed that 30% of participants in the MTS group had an autism diagnosis and that scores on autistic traits—as measured by the autism quotient (AQ, Baron-Cohen et al., Citation2001)—were higher in this group than in both, the GC synaesthetes and the control group. The researchers highlight this finding as relevant because previous research has associated autism with empathy impairment (e.g., Baron-Cohen & Wheelwright, Citation2004; Decety & Moriguchi, Citation2007). Therefore, it follows that if autism can also be present in individuals who experience MSS, then this provides evidence against the view that MSS is related to enhanced empathy (Baron-Cohen et al., Citation2016). However, the researchers do acknowledge that the co-morbidity of autism and MTS could be due to the recruitment of participants from an autism database. Crucially, the assumption that autism is linked to a lack of empathic ability has been challenged by recent research (Santiesteban et al., Citation2021). Using a novel empathy task, see CARER description below, Santiesteban and colleagues found that compared to controls, autistic participants showed difficulties when required to retrospectively infer the affective state of others, but not when sharing such affective states. Further research also suggests that when psychometric measures of MSS are used—rather than relying on purely self-report of presence/absence of experience—then self-reported experiences of enhanced empathy are evident in MSS (Ward et al., Citation2018).
A limitation worth noting in previous research on empathy in MSS is the reliance on self-report questionnaires such as the EQ and the Interpersonal Reactivity Index (IRI, Davis, Citation1980). This can be problematic due to the subjective nature of self-report. Furthermore, these measures of self-report focus on trait disposition, which is whether in general, one tends to consider the affective states of other (e.g., Martínez-Velázquez et al., Citation2020), rather than state empathy, which is the affective response elicited in specific situations (Van der Graaff et al., Citation2016). In fact, researchers have argued that more reliable measures of empathy should consider the individual’s ability to share what they perceived to be the affective state of others (Coll et al., Citation2017), hereafter referred to as affect sharing. Affect sharing is the extent to which identifying an emotion from a target, results in the empathizer experiencing the same emotion. According to Coll and colleagues, using a measure of affect sharing would allow researchers to consider individual differences. For example, in a hypothetical scenario in which a “Target” is upset and rates his affective state as 8 (out of 10), and there are two empathizers “A” and “B”. Empathizer “A” identifies the target’s emotion as 8 and their own affective state as 5; whereas Empathizer “B” identifies the target’s emotion as 6 but their own as 5. In this case, Empathizer “B” would show a higher degree of affect sharing (6–5 = 1) than empathizer “A” (8–5 = 3). Santiesteban et al. (Citation2021) measured affect sharing using a video-based empathy task (The Continuous Affective Rating and Empathic Response task, CARER). In addition to measuring affect sharing, this task also includes traditional measures of empathy such as emotion identification and affective empathy. Moreover, the CARER task also includes online and offline measures of these components of empathy. The online condition aims to resemble the dynamics of real-life social interaction as participants make judgements of their own and the Targets’ affective states using continuous ratings as they watch the Target describe an emotionally-charged real-life event. The offline measure requires reflective processing and is akin to empathy measures in previous studies in which participants are asked to make affective judgements after exposure to the affective stimuli. The offline rating of each video is required after the participant has provided continuous online ratings for the same video story.
In the current study, the CARER task is used to further explore the empathic abilities of individuals with MSS. Specifically, our study seeks to investigate if there are differences in emotion identification, affective empathy and affect sharing in MSS individuals compared to controls. Each of these three variables is derived from self and other affective ratings—see task description below. For emotion identification and affective empathy, the “other” rating is the Target’s own rating of their affective state. However, affect sharing is calculated by subtracting the participants’ ratings of the Target’s affective state (other) from their affective state (self) rating. Previous research suggests that atypical self-other processing could underly the mirror-sensory experiences, such that a blurring of self-other representations may facilitate enhanced empathy reporting of MSS individuals (Banissy & Ward, Citation2013). Data from the affect sharing measure in the CARER task would allow us to compare the difference between self-other ratings, thus enabling us to test the atypical self-other theory in MSS.
To the best of our knowledge, the comparison of online and offline measures of empathy has not been used before in studies of MSS. Therefore, data from these conditions could also contribute to our understanding of empathy processes in MSS. Specifically, the current experimental design enables us to determine: (i) whether the empathic abilities of those with MSS experiences differ from controls when making affective judgements in the online (resembling real-life interactions) and offline (requiring reflective processing) conditions; and (ii) whether atypical self-other processes play a role in the empathic abilities of MSS individuals. Based on the discussed findings, we expect MSS participants to show higher affective empathy, emotion identification and affect sharing than controls. However, lack of previous research prevents us from making predictions on the online vs. offline conditions. Furthermore, in line with the atypical self-other control theory, we predict that the difference in the ratings for self and other in the MSS group will be significantly smaller compared to controls.
Method
Participants
Fifty-four adults volunteered to take part in the study in exchange for a small monetary reimbursement. Participants first completed an online Vicarious Experiences Questionnaire (VEQ; Grice-Jackson et al., Citation2017; Ward et al., Citation2018) screening for MSS (both MTS and MPS)—see procedures below. To have a power of 0.8 to detect a medium effect size (0.5), with a significance level of .05, a total of 42 participants were required. The final sample satisfied these requirements. The first step of participant recruitment was via a general survey to all new volunteers who signed up to take part in psychology experiments at the Psychology department, University of Cambridge. As part of creating an account, volunteers were asked if they felt touch in their own body when observing someone else being touched. Those who responded positively were then invited to take part in our study. The VEQ allowed classifying our participants either as MSS (N = 20, 13 Females; age range: 18–55, Mean age = 29, SD = 11.11) or controls (N = 34, 19 Females, age range: 18–66, Mean age = 27, SD = 10.72). For the MTS classification, we used a cut-off score of 7/15 positive responses to the touch videos, this is a similar cut off to that recommended by Ward et al., Citation2018. Ward and colleagues used 14 videos depicting both pain and touch and recommend a cut-off of 7/14. In addition, for all responders of the VEQ, we used cluster analysis (see Botan et al., Citation2018; Bowling et al., Citation2019) to classify the qualitative responses to the touch and pain videos. For the pain videos, responders were classified as either sensory/localized or affective/general responders. Thus, in the MSS sample, N = 10 were classified as MTS, N = 6 as MPS sensory/localized, N = 2 as MTS + MPS sensory/localized and N = 2 as MTS + MPS affective/general.
The MSS and Control groups did not differ in terms of Age, (Mann–Whitney U = 270, p = .211, Mean Rank: MSS = 30.98, Controls = 25.46) or Gender, χ2 (1) = .43, p = .51. Due to the memory component of the empathy task—recalling a story during the offline rating condition—we measured immediate recall using the logical memory subscale of the Wechsler’s scale, fourth edition (WMS-IV, Wechsler, Citation2009). No group differences were found on this measure [t(52) = −.92, p = .36, d = .26; MSS: M = 27.75, SD = 5.92; Controls: M = 26.29, SD = 5.42]. Ethical approval was obtained from the Cambridge Psychological Research Ethics Committee. All participants provided written informed consent.
Materials and procedures
Before attending the lab for the experimental session, and after completion of the online VEQ, all participants were screened for symptoms of depression. This was because the CARER task required exposure to emotionally negative stimuli, aimed at eliciting an empathic response. Only those scoring below 30 (the cut-off for clinical depression) on the BDI were invited to take part in the experiment. Since the BDI measures depressive symptoms over a two-week timeframe, it was administered again at the beginning of the experimental session in the lab. No participants were excluded based on BDI scores. Following the BDI, we administered the Wechsler’s logical memory subscale before proceeding to the CARER task.
Vicarious Experiences Questionnaire (VEQ; Bowling et al., Citation2019). The VEQ consisted of short video clips depicting either touch or pain. In the pain videos, participants were exposed to 16 pain videos (e.g., Grice-Jackson et al., Citation2017), showing people experiencing mild to moderate pain—ranging from sports injuries to injections in various parts of the body. The touch videos consisted of 15 clips depicting touch to the left, right or both sides of a model’s face. There was a male and a female model. Other videos depicted touch to hands, left, right or both that were presented either from a first—or third-person perspective. Finally, there were three videos depicting touch to non-human stimuli. These clips showed two cups side by side and a finger touching either the cup on the right, the one on the left or both cups.
Empathy task (CARER). shows a trial sequence of the CARER task. The task consisted of short videos (30 seconds each) of individuals (Target) describing a situation where, (a) they carried out day-to-day tasks (neutral stories) or (b) a time when they experienced emotional distress (affective stories), based on real-life events—see Santiesteban et al. (Citation2021) for a detailed description of the task. There were two blocks of 16 trials each, with affective and neutral stories presented in a pseudorandomized order, such that no more than three trials of the same type were presented in succession. Participants were required the rate the intensity of the emotional experience, from extremely calm (0) to extremely upset (10). On each online trial, participants were asked to rate either how they felt while watching each video (Online self-rating) or how the person in the video (Target) was feeling while telling the story (Online other rating). The online rating trials for self or other were blocked and block order was counterbalanced across participants. Although each story was different, the content of the negative affect stories was mostly equivalent in each block. For the online measure participants provided continuous ratings. In contrast, the offline measure consisted of a single rating after the video was presented. For each trial, if the online rating was for self, then the offline rating was for the Target (Offline other rating) and vice versa (Offline self-rating). Each person in the video (Target) had previously provided their own rating of how they felt while telling the story. This allowed us to compute the variables of interest as follows, (1) Emotion identification (Target ratings of their own state—Empathizer rating of the Target’s state), with lower scores indicating more accurate emotion identification; (2) Affective empathy (Target’s state—Empathizer’s state), with lower scores indicating higher affective empathy and; (3) Affect sharing (Empathizer’s rating of the Target’s state—Empathizer’s state), with lower scores indicating higher affect sharing. Both online (continuous ratings) and offline (single rating) were obtained for each of the three measures. The CARER task was designed in MATLAB. The continuous rating was obtained by translating the screen coordinates for the location of each mouse click to the nearest decimal point in the scale, thus yielding scores with two decimal points within the range of 0–10.
Figure 1. Example of a trial sequence from the CARER task. There were two blocks. In one block the online (continuous) rating would be for self and the offline rating for other, then the order would be reversed for the other block.
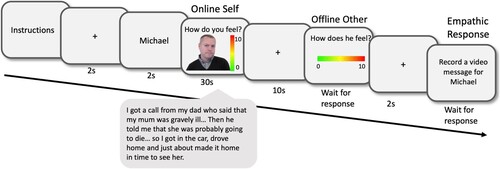
Following the offline ratings, participants were asked to record a brief video message to the Target based on the story they just watched. This part of the task was designed to elicit both verbal and non-verbal empathic responses. These video-recorded responses were scored independently by researchers blind to the experimental design and participant group. The researchers coded the following variables: frequency of empathic phrases (e.g., I’m sorry to hear … , that sounds awful, I feel for you, I can’t image … , etc.), frequency of verbal signs of personal distress (e.g., soft, breaking, slow, sadness), and frequency of non-verbal signs of distress (e.g., teary, sad facial expressions—turned down mouth eyebrows raised/knitted—, hand over mouth or chest). The task took approximately 35–40 minutes to complete.
Self-report measures. Participants also completed three self-report questionnaires: an empathy measure, the Interpersonal Reactivity Index (IRI; Davis, Citation1980) which consists of 4 subscales: empathic concern, fantasy, personal distress, and perspective taking. The IRI is a widely used empathy questionnaire, with acceptable internal consistency, (Cronbach’s alpha = .68—.79) and good test-retest reliability (0.61–0.81; Davis, Citation1980). Participants also completed the Autism Quotient (AQ; Baron-Cohen et al., Citation2001). The AQ is a 50-item scale designed to assess: social skills, attention switching, attention to detail, communication, and imagination. Cronbach’s alpha for the AQ has been found to be acceptable for non-autistic (.75) and good for autistic adults (.84)—see Broadbent et al. (Citation2013). Finally, the Toronto Alexithymia Scale (TAS-20; Bagby et al., Citation1994) was also administered. This 20-item scale includes 3 subscales: difficulty describing feelings, difficulty identifying feelings and externally oriented thinking. The TAS-20 has good internal consistency (Cronbach’s alpha = .81) and test-retest reliability (.77; Bagby et al., Citation1994). The entire experimental session lasted approximately 80–90 minutes.
Transparency and openness
We reported how we determined our sample size, all data exclusions, and all measures of the study. All data will be available at the UK Data Service repository [link to follow here]. Data were analysed using SPSS 28 (IBM SPSS Statistics, 2021). This study’s design and its analysis were not pre-registered.
Data analysis
A preliminary inspection of the CARER data revealed a consistent pattern across participants, whereby ratings were low in the first half of the videos—which contained the background to the emotional event—and higher in the latter stages of the story that contained the emotional climax. Thus, online rating data were split into two epochs (first and last 15s of each video, T1 and T2) and averaged within epoch. For offline analyses, participants provided a single score while Target ratings were continuous scores. Therefore, for the offline data, we subtracted the participants’ offline rating from the Target’s maximum rating. Thus, in total, 9 dependent variables were obtained: T1 and T2 online, plus offline versions of Emotion Identification, Affective Empathy and Affect Sharing scores.
Online data were analysed using ANCOVA with Story type (affective, control) and Time (T1, T2) as within-subject factors and Group (MSS, control) as a between-subjects factor. The alexithymia and autistic traits scores differed between the two groups—see below—therefore, to control for these differences, participants’ scores on the TAS-20 and the AQ were entered as a covariate in each of the analyses reported below. The analysis of the offline data included the same factors, except for Time. Greenhouse-Geisser corrected values are reported where sphericity assumptions were not met. Furthermore, we used Bonferroni corrections for all post-hoc multiple comparisons.
Results
Self-Report Measures. shows the descriptive statistics of the self-report measures. Due to technical difficulties one participant’s TAS-20 score, and a second participant’s IRI score were not recorded, both participants were from the control group. Analysis of the descriptive data for the BDI and AQ showed that they did not meet the parametric assumptions. Therefore, non-parametric analyses using Mann–Whitney U tests were conducted on these variables. No differences between the groups were found for depression scores on the BDI, U = 254.50, p = .12 (MSS Mean Rank = 31.78, controls Mean Rank = 24.99). However, the groups differed on autism traits, U = 226, p = .04, and MSS participants (Mean Rank = 33.20) scored higher in the AQ than those in the control group (Mean Rank = 24.15). Group differences were also found in the total alexithymia scores, t(51) = 2.84, p = .006, d = .80; overall, the MSS group (M = 56.7, SD = 10.45) scored higher than the control group (M = 49.12, SD = 8.75). However, no differences were found between the groups on any of the TAS subscales—see . Finally, there were no significant group differences on any of the IRI sub-scales—see .
Table 1. Descriptive statistics and group comparisons of the self-report data.
CARER data
Emotion Identification Online. This analysis revealed that the covariate AQ scores significantly adjusted the dependent variable Story type (p = .004) and the Story Type × Time interaction (p = .02). The main effect of Story type was significant, F(1,49) = 8.37, p = .006, η2p = .15. Overall, after controlling for AQ scores, our participants’ judgements of the Target’s state were less accurate for affective (M = 2.01, SEM = .11, 95% CI [1.78, 2.24]) than for neutral stories (M = 1.19; SEM = .09, 95% CI [1.02, 1.36]). No other main effects or interactions reached significance, all ps ≥ .072—see Appendix A1 in supplementary material.
Emotion Identification Offline. No significant main effects or interactions were found, all ps ≥ .42.—see Appendix A2 in supplementary material.
Affective Empathy Online. This analysis also revealed that the covariate AQ scores significantly adjusted the dependent variables Story type (p = .04) and Group (p = .047). The main effect of Story type was significant, F(1,49) = 15.25, p < .001, η2p = .24. Overall, after controlling for AQ scores, participants’ self ratings were closer to the Target’s own ratings during neutral (M = .60, SEM = .09, 95% CI [.43, .78]) than during affective stories (M = 3.27, SEM = .14, 95% CI [.2.99, 3.54]). The main effect of time was also significant, F(1,49) = 7.04, p = .01, η2p = .13; showing that the difference between participants and target self ratings was larger for the second part of the story, T2 (M = 2.27, SEM = .10, 95% CI [2.04, 2.48]) than for the first part, T1 (M = 1.60, SEM = .06, 95% CI [1.49, 1.71]). After controlling for AQ scores, the main effect of Group (MSS M = 1.96, SEM = .12; controls M = 1.91, SEM = .09; p = .79) and the Group interactions failed to reach significance (all ps ≥ .16)—see Appendix A3 in supplementary material.
Affective Empathy Offline. None of the main effects or interactions reached significance in this analysis, (all ps ≥ .29)—see Appendix A4 in supplementary material.
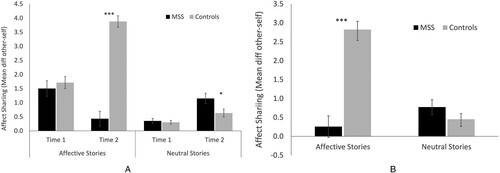
Affect Sharing Online. There was a significant main effect of Story type, F(1,49) = 9.97, p = .003, η2p = .17. Affect sharing was higher for neutral stories (M = .61, SEM = .07, 95% CI [.47, .74]) than for affective stories (M = 1.88, SEM = .12, 95% CI [.1.63, 2.13]) compared to. There was also a main effect of Group, F(1,49) = 20.19, p < .001, η2p = .29, higher affect sharing was found for the MSS (M = .86, SEM = .13, 95% CI [.60, 1.12]) than for the control group (M = 1.63, SEM = .10, 95% CI [1.43, 1.83]). However, the effect of Time was not significant, p = .09. In terms of interaction effects, the Group × Story Type interaction was significant, F(1,49) = 61.56, p < .001, η2p = .56. Post hoc analysis revealed that the MSS group showed significantly higher affect sharing compared to controls for affective stories (MSS M = .97, SEM = .21, 95% CI [.55, 1.38]; controls M = 2.80, SEM = .16, 95% CI [2.48, 3.11], p < .001, η2p = .48) but not for neutral stories (MSS M = .75, SEM = 11, 95% CI [.52, .98]; controls M = .47, SEM = .09, 95% CI [.29, .64], p = .06, η2p = .069)—. The Group × Time interaction was also significant, F(1,49) = 26.29, p < .001, η2p = .35. The post hoc analysis showed that only during the late part of the story (T2 which contains the climax of the affective story), the MSS group (M = .79, SEM = .18, 95% CI [.44, 1.14]) showed significantly higher affect sharing than controls (M = 2.26, SEM = .13, 95% CI [.1.99, 2.52], p < .001, η2p = .46). Finally, the 3-way interaction (Story Type × Time × Group) was also significant, F(1,49) = 58.77, p < .001, η2p = .55. Simple effects analysis showed that affect sharing for neutral stories in the last part of the story was higher in the control group (M = .63, SEM = .14, 95% CI [.35, .91]) than in the MSS group (M = 1.15, SEM = .18, 95% CI [.78, 1.52]; F(1,49) = 5.86, p = .04, η2p = . 09). However, for affective stories, the reverse pattern was observed, MSS participants’ affect sharing was higher at T2 (M = .43, SEM = .27, 95% CI [.10, .96]) than controls’ (M = 3.88, SEM = .20, 95% CI [3.47, 4.28]); F(1,49) = 98.95, p < .001, η2p = .67—see Appendix A5 in supplementary material.
Affect Sharing Offline. The covariate AQ scores significantly adjusted the Group variable (p = .023, η2p = .10). The main effect of Group was significant, F(1,49) = 24.78, p < .001, η2p = .34. Across both types of stories, after controlling for AQ scores, the MSS group showed higher affect sharing (M = .52, SEM = .17, 95% CI [.17, .86]) than the control group (M = 1.64, SEM = .13, 95% CI [1.37, 1.90]). Furthermore, the Story Type × Group interaction was also significant, F(1,49) = 40.59, p < .001, η2p = .45. Simple effects analysis showed that affect sharing for affective stories was higher for the MSS group (M = .26, SEM = .29, 95% CI [-.32, .83]) than for the control group (M = 2.82, SEM = .21, 95% CI [2.38, 3.26]); F(1.49) = 46.95, p < .001, η2p = .49)—see Appendix A6 in supplementary material.
Additional Analysis: to explore the moderator effect of AQ in the analyses reported above, a sub-sample of control participants (N = 20) were selected to match the MSS sample (N = 20) on AQ scores. Each of the analyses in which the covariate AQ significantly adjusted the dependent variables was repeated. The findings of this sub-sequent analyses replicated those from the initially reported ANCOVAs. Since they do not add valuable insights to the initial analyses, these results have been added to the Supplementary Materials—see Appendix B.
To address the atypical self-other processes in MSS theory, we further explored this interaction by looking at the raw ratings for self and other in both groups using paired samples t-test—see .
Figure 2. Mean Affect Sharing per group and condition. Panel A illustrates the 3-way interaction in the Online condition: Group × Story type × Time. Panel B shows the Group × Story type interaction in the offline condition. Error bars represent the SEM. **p < 0.01; *p < 0.05.
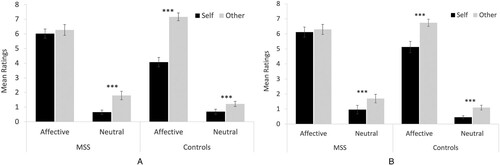
Self-Other Online. This analysis revealed that for neutral stories, the difference between ratings for self and other were significant in both groups (MSS: t(19) = −5.62, p < .001, d = 1.26; controls: t(33) = −3.87, p < .001, d = .66). However, the pattern of results was different for affective stories; while in the control Group the ratings for self were significantly different to ratings for other, t(33) = −10.83, p < .001, d = 1.86, in the MSS Group, the difference between self and other ratings failed to reach significance, t(19) = −1.60, p = .13, d = .36.
Self-Other Offline. The pattern of results for offline trials was similar to the online ones. For neutral stories, the difference between self and other ratings was significant in both the MSS [t(19) = −2.91, p = .009, d = .65] and control group [t(33) = −4.93, p < .001, d = .85]; whereas for affective trials, there was a significant difference on self and other ratings in the control group [t(33) = −5.17, p < .001, d = .88], but not in the MSS group [t(19) = −1.06, p = .30, d = .24].
Taken together, the findings from the self-other analysis indicates that unlike controls, individuals with MSS judged their own affective state to be significantly closer to that of the Target in the video, but only after exposure to emotionally-charged stories ().
Figure 3. Mean ratings for self and other per participant group during each story type. Panel A shows ratings for self and other in Online trials and Panel B shows the offline trials. Error bars represent SEM. **p < 0.01.
Video Responses. The participants’ video responses (a video message to each Target) were coded by two researchers who were blind to the experimental design. One researcher coded all video responses (32 videos per participant) from the whole sample, to ensure reliability of these ratings, a second researcher scored the responses of 25 randomly selected participants. We tested inter-rater reliability with intraclass correlation coefficients (ICC) estimates and their 95% confidence intervals, which were calculated based on a median rating (k = 2), absolute agreement, 2-way mixed effects model. A high degree of ICC reliability was found for the three measures, frequency of empathic phrases, ICC = .97, 95% CI = .94 to .98, F(44,44) = 32.13, p < .001; frequency of verbal signs of personal distress, ICC = .98, 95% CI = .96 to .99, F(44,44) = 54.81, p < .001; frequency of physical signs of distress ICC = .91, 95% CI = .83 to .95, F(44,44) = 10.92, p < .001. The data from video responses did not meet parametric assumptions, therefore non-parametric analyses were carried out.
Mann–Whitney tests on the video response variables indicated group differences during affective trials for frequency of empathic phrases, U = 507, p = .002, the MSS group (Mean Rank = 19.15) used fewer empathic phrases than controls (Mean Rank = 32.41). Group differences, in the same direction, were also found in the frequency of verbal signs of personal distress U = 484, p < .005 (Mean Rank MSS = 20.30, controls = 31.74). However, no group differences were found in the frequency of physical signs of distress, U = 411, p = .17 (Mean Rank MSS = 23.95, controls = 29.59).
Correlations. shows the Spearman’s rho correlation coefficients of the key dependent variables across all participants. This analysis was conducted to determine the association between the self-reported measures and the variables from the CARER task. Although, our sample size is small for these analyses and the magnitude of a correlation is unstable in small samples (Schönbrodt & Perugini, Citation2013), reporting these correlations could motivate future research. However, these results should be considered indicative, rather than robust findings.
Table 2. Correlations between key variables from the CARER task and self-reported questionnaires.
We found a significant positive correlation between autism traits (AQ scores) and alexithymia scores (TAS-20), rs (53) = .36, p = .009. This finding is consistent with previous research showing a link between autism and alexithymia (e.g., Bird & Cook, Citation2013). The Personal Distress subscale of the IRI was significantly correlated to AQ scores [rs (53) = .394, p = .004]. In addition, the analysis showed a significant correlation between the Empathic Concern subscale of the IRI and the CARER online measure for affective empathy, rs (53) = −.28, p = .043. Thus, indicating that higher scores in the empathic concern subscale were associated with higher affective empathy scores in CARER. There was also a significant correlation between offline affect sharing and AQ scores, rs (54) = −.41, p = .002 (noting that the negative correlation implies high AQ is linked to high affect sharing). The online measure of affect sharing also correlated with alexithymia scores: rs (53) = −.42, p = .002, thus, indicating that those participants who scored higher in the alexithymia scale, showed higher affect sharing.
Discussion
The current study aimed to explore the empathic abilities of individuals with MSS compared to a group of non-synaesthete participants using the CARER task, an empathy measure that comprises three variables: emotion identification, affective empathy and affect sharing. In addition, the experimental design allowed us to contrast empathic responses online—during exposure to affective stimuli, resembling real-life social interactions—and offline—after exposure to the video stimuli, in line with traditional empathy measures.
Our results show no significant differences between the two groups on emotion identification and affective empathy. However, we did find group differences in the affect-sharing measure. The MSS group showed higher affect sharing ability than controls. These findings indicate that MSS individuals rate the intensity of the emotional experience similarly for both self and others. In contrast, the intensity ratings by the control group were higher for the person in the video compared to self-ratings. The implication of these findings in relation to previous research on empathy in mirror-sensory synaesthesia is discussed in the section below.
Emotion identification and affective empathy
Taken at face value, the failure to find significant differences in emotion identification and affective empathy does not support previous work showing enhanced empathy and emotion recognition in individuals who experience mirror-sensory synaesthesia (e.g., Banissy et al., Citation2011; Banissy & Ward, Citation2007; Ward et al., Citation2018). However, there are important methodological differences between the measures used in previous studies and those derived from the CARER task. Previous empathy studies using self-report questionnaires to measure affective empathy require participants to reflect on hypothetical scenarios based on their own life experiences, for example, “I am good at predicting how someone will feel” is an item from the Empathy Quotient (EQ; Baron-Cohen & Wheelwright, Citation2004). Responding to such a statement, (a) requires introspection about general feelings in hypothetical scenarios, and (b) lacks the spontaneity of responses that are required in everyday social interactions. In contrast, the CARER task involves watching a video clip of someone describing a specific sad event in their lives and asks participants to react to that story by rating how it makes them feel as they watch the video clip. Although introspection is also needed in these trials, participants have a specific point of reference—the story they just listened to—when rating how they feel at different points of the story. The continuous affect rating resembles the spontaneous—internal—responses that are experienced in real-life interactions. Furthermore, another crucial difference between a questionnaire and the affective empathy measure of the CARER task, is that it includes the actual rating of the Target (person in the video), which arguably provides a “more objective” measure of affective empathy. Participants’ own ratings are subtracted from the Target’s affective rating. The resulting score provides an index of empathic accuracy (e.g., Ickes, Citation2001), that is how closely the participant’s affective state matches that of the Target. Similarly, the measure of emotion identification from the CARER task differs from the traditional empathy measures that require participants to label emotions of static facial stimuli (e.g., Dziobek et al., Citation2008). The dynamic nature of video clips and the advantage of comparing the affective rating scores between the Target and participants in the CARER task provides a more ecologically valid measure of emotion identification than previous measures.
The lack of differences between MSS and controls on emotion identification and affective empathy also appears to be consistent with reports of no empathy advantage of MSS compared to controls (Baron-Cohen et al., Citation2016). However, the inclusion of a third dependent variable, affect sharing, in our experimental paradigm allows us to explore empathy from the participant’s own experience and provides contrasting evidence to such previous findings. Our results show that the MSS group demonstrated higher affect sharing than controls, both on the online and offline measures.
Affect sharing comprises the participant’s perception of the affective state of the other, compared to their own affective state—following exposure to the emotional stimuli. It has been suggested that affect sharing is a more reliable measure of empathy because it considers individual differences (Coll et al., Citation2017). This argument is supported by the findings from this study that those individuals who experience MSS show higher affect sharing than neurotypicals. Although there is an abundance of empathy definitions in the field, it is generally accepted that this psychological construct refers to the affective state originated by the directly perceived, imagined or inferred affective state of another being (Batson, Citation2009; Singer & Lamm, Citation2009). A key element of this definition is that although an other-oriented response, empathy is experienced at an individual level. Therefore, the intensity of the empathic response would be determined by the extent to which the perceived affective state of the other matches the affective state of the self. The analysis of self and other ratings of affective stories in the current study shows that they were significantly more closely matched in the MSS group than in the control group. However, this finding requires further consideration and ponders the question of to what extent feeling the same intensity of affect as what we perceive in another being is the desired, more effective and prosocial outcome. A crucial aspect of empathy is self-other distinction, that is, the awareness that the source of the experienced affective state originates from the other, not within ourselves (e.g., De Vignemont & Singer, Citation2006; Decety & Jackson, Citation2004; Singer & Lamm, Citation2009). Not being able to distinguish between self and other representations could potentially lead to personal distress or the inability to provide an affective response (Singer & Lamm, Citation2009). To put this argument into context, when a patient is in pain and is seen by a healthcare professional, the latter must be aware that it is the patient who is in pain, not them, to provide the appropriate care. The lack of self-other distinction here could have negative consequences for the patient who might not receive the care and attention they need.
The closely matched ratings for self and others observed in the MSS participants in this study could therefore be considered atypical. This is in line with the atypical self-other processing theory of MSS proposed by Banissy and Ward (Citation2013), also referred to as Self-Other Control Theory, Ward and Banissy (Citation2015). Further support for this theory, and consistent with our findings, comes from the results of a recent fMRI study by Li, Racey, Bouyagoub, Critchley & Ward, (under review). Li and colleagues asked vicarious pain responders and a control group to rate the intensity of pain for self and other. Pain was delivered via an electric shock to either the participant or the experimenter’s hand or foot. They found that the control group rated pain intensity to be higher for self than other; however, the vicarious pain responders showed similar ratings for both themselves and the experimenter. Furthermore, multivariate analysis revealed less self-other distinction for pain intensity ratings in the vicarious pain responders in brain regions associated with physical pain, known as the “pain matrix”, which includes somatosensory cortex, mid-cingulate cortex and insula.
Previous empirical evidence supporting the atypical self-other theory comes from studies in the socio-cognitive domain. For example, Maister et al. (Citation2013) used a self-face recognition task using morphed images containing various proportions of their face and of an unfamiliar face before and after exposure to videos showing tactile stimulation to the unfamiliar face. They found that after exposure to the touch videos, individuals with mirror-touch synaesthesia were more likely to identify images that were previously rated as containing equal quantities of self and other as images of themselves. This suggests that the induced MSS experience led to blurring mental representations of self and other. Consistent with these findings, a study by Santiesteban et al. (Citation2015) found that participants with mirror-touch synaesthesia showed impaired ability to inhibit imitation of a motor action—which required the ability to distinguish competing representations from self and others. Thus, the current study’s results showing that, compared to neurotypical controls, individuals with MSS rate self-affective states as close to the state of others after exposure to emotional stimuli, provide further evidence of atypical self-other processing in MSS, this time in the affective domain.
Affect sharing & prosocial behaviour in MSS
Our findings also show that higher affect sharing in MSS does not translate to better prosocial behaviour than controls. The analysis of the video messages that participants were asked to record for the Target in the videos shows group differences, but these differences were in the opposite direction. Those with MSS used fewer empathic phrases and fewer verbal signs of personal distress than the neurotypical group. Although it appears contradictory that higher affect sharing does not necessarily lead to more prosocial behaviour, this finding can be interpreted in relation to atypical self-other distinction, which, in this case, resulted in a lack of engagement in prosocial behaviour. Martin et al. (Citation2017) found some anecdotal evidence from MSS individuals that relates to these findings. The authors refer to it as a “double-edge sword”, although those with MSS show enhanced ability when relating to others, almost as if they share the same feelings, their need to regulate the intensity of the MSS experience can lead to avoidance behaviour that appears to be less prosocial and socially withdrawn.
It is worth mentioning that in our sample, differences were found between the groups on autism traits and alexithymia scores. The MSS group scored higher in autism traits than controls. This finding is consistent with Baron-Cohen et al.’s (Citation2016) which showed that 30% of their MSS participants reported having an autism diagnosis. The link between MSS and autism deserves to be explored further. In this study, the group differences in autism trait scores were controlled for by including AQ as a covariate in our statistical analysis. Our results showed that AQ was a significant moderator of the failure to reach significance between the groups in affective empathy. Furthermore, in the affect sharing analysis, even after controlling for AQ, the MSS group showed higher affect sharing. A follow-up analysis with a subset of matched controls on AQ replicated the original findings from the ANCOVAs.
Our MSS participants also scored higher on the alexithymia scale, although no group differences were found in any of the subscales. In one of our previous studies (Bowling et al., Citation2019), MSS—specifically, mirror-pain synaesthesia—was associated with lower alexithymia scores overall and on the externally-oriented thinking subscale compared to non-responders to vicarious pain. One possible explanation for the discrepancy between our current study and Bowling et al.’s (Citation2019) could be the higher scores on autistic traits found in the present study, which was not reported in Bowling et al.’s study as autistic traits were not measured. It is possible that this difference between the two samples could account for the relationship between MSS and alexithymia scores. Nevertheless, the Bowling et al study also showed higher self-reported depersonalization and interoceptive sensibility. Overall, this pattern of results suggests altered self-body awareness in vicarious pain responders. A direct comparison of these findings with our current results is not possible as this study did not include measures of depersonalization or interoception.
Limitations to the current study include the use of self-report measures, which could introduce response bias, such as social desirability bias. Our awareness of this limitation is what led us to introduce the CARER task, which although based on self-report, the inclusion of the Target’s own rating to calculate emotion identification and affective empathy provides some degree of objectivity. For both dependent variables, participants’ own ratings are subtracted from the Target’s ratings to provide an index of these measures. Another limitation is the in our design, we use negative and neutral affect stimuli but did not include positive affect. Although, this is not uncommon in empathy research, the interpretation of our findings are limited to affect sharing in the context of negative emotional experiences and reduced empathic responses/ prosocial behaviour in individuals who experience MSS. Future studies using the CARER task could include positive-valanced stimuli to investigate the extent to which affect sharing in MSS differs from control when happy experiences are shared. Furthermore, future studies could also use the CARER task in combination with physiological measures such as skin conductance or heart rate to measure affective arousal and personal distress more objectively.
Conclusions
The findings from the current study provide further evidence of the complexities of empathy as a psychological construct. Our research highlights the importance of improving current measures to enhance our understanding of socio-affective abilities, both in typical and atypical populations. Using the CARER task to test the empathic abilities of MSS individuals and neurotypical controls, we found that those with mirror-sensory experiences show enhanced affect sharing compared to controls and that this could be related to atypical self-other representations in this population. However, our results also show that such enhanced affect sharing does not translate into better prosocial behaviour, suggesting that to regulate the mirror-sensory experience, these individuals are likely to display social withdrawal, which could potentially lead to erroneous attribution of inappropriate social abilities.
SupMat_MSS_CARER_R2.docx
Download MS Word (97.3 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Bagby, R. M., Parker, J. D., & Taylor, G. J. (1994). The twenty-item Toronto Alexithymia Scale—I. Item selection and cross-validation of the factor structure. Journal of Psychosomatic Research, 38(1), 23–32. https://doi.org/10.1016/0022-3999(94)90005-1
- Banissy, M. J., Garrido, L., Kusnir, F., Duchaine, B., Walsh, V., & Ward, J. (2011). Superior facial expression, but not identity recognition, in mirror-touch synesthesia. The Journal of Neuroscience, 31(5), 1820–1824. https://doi.org/10.1523/JNEUROSCI.5759-09.2011
- Banissy, M. J., & Ward, J. (2007). Mirror-touch synesthesia is linked with empathy. Nature Neuroscience, 10(7), 815–816. https://doi.org/10.1038/nn1926
- Banissy, M. J., & Ward, J. (2013). Mechanisms of self-other representations and vicarious experiences of touch in mirror-touch synesthesia. Frontiers in Human Neuroscience, 7, 112.
- Baron-Cohen, S., Robson, E., Lai, M. C., & Allison, C. (2016). Mirror-touch synaesthesia is not associated with heightened empathy, and can occur with autism. PLoS One, 11(8), e0160543. https://doi.org/10.1371/journal.pone.0160543
- Baron-Cohen, S., & Wheelwright, S. (2004). The empathy quotient: An investigation of adults with Asperger syndrome or high functioning autism, and normal sex differences. Journal of Autism and Developmental Disorders, 34(2), 163–175. https://doi.org/10.1023/B:JADD.0000022607.19833.00
- Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J., & Clubley, E. (2001). The autism-spectrum quotient (AQ): Evidence from asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. Journal of Autism and Developmental Disorders, 31(1), 5–17. https://doi.org/10.1023/A:1005653411471
- Batson, C. D. (2009). These things called empathy: Eight related but distinct phenomena. In J. Decety, & W. Ickes (Eds.), The social neuroscience of empathy (pp. 3–15). Review.
- Bird, G., & Cook, R. (2013). Mixed emotions: the contribution of alexithymia to the emotional symptoms of autism. Translational Psychiatry, 3(7), e285–e285. https://doi.org/10.1038/tp.2013.61
- Bird, G., & Viding, E. (2014). The self to other model of empathy: Providing a new framework for understanding empathy impairments in psychopathy, autism, and alexithymia. Neuroscience & Biobehavioral Reviews, 47, 520–532. https://doi.org/10.1016/j.neubiorev.2014.09.021
- Botan, V., Bowling, N. C., Banissy, M. J., Critchley, H., & Ward, J. (2018). Individual differences in vicarious pain perception linked to heightened socially elicited emotional states. Frontiers in Psychology, 9, 2355. https://doi.org/10.3389/fpsyg.2018.02355
- Bowling, N. C., Botan, V., Santiesteban, I., Ward, J., & Banissy, M. J. (2019). Atypical bodily self-awareness in vicarious pain responders. Philosophical Transactions of the Royal Society B: Biological Sciences, 374(1787), 20180361. https://doi.org/10.1098/rstb.2018.0361
- Broadbent, J., Galic, I., & Stokes, M. (2013). Validation of autism spectrum quotient adult version in an Australian sample. Autism Research and Treatment, 2013.
- Coll, M. P., Viding, E., Rütgen, M., Silani, G., Lamm, C., Catmur, C., & Bird, G. (2017). Are we really measuring empathy? Proposal for a new measurement framework. Neuroscience & Biobehavioral Reviews, 83, 132–139. https://doi.org/10.1016/j.neubiorev.2017.10.009
- Davis, M. H. (1980). A multidimensional approach to individual differences in empathy. JSAS Catalogue of Selected Documents in Psychology, 10, 85. https://doi.org/10.1037/t01093-000.
- Decety, J., & Jackson, P. L. (2004). The functional architecture of human empathy. Behavioral and Cognitive Neuroscience Reviews, 3(2), 71–100. https://doi.org/10.1177/1534582304267187
- Decety, J., & Moriguchi, Y. (2007). The empathic brain and its dysfunction in psychiatric populations: Implications for intervention across different clinical conditions. BioPsychoSocial Medicine, 1(1), 22–21. https://doi.org/10.1186/1751-0759-1-22
- De Vignemont, F., & Singer, T. (2006). The empathic brain: How, when and why? Trends in Cognitive Sciences, 10(10), 435–441. https://doi.org/10.1016/j.tics.2006.08.008
- Dziobek, I., Rogers, K., Fleck, S., Bahnemann, M., Heekeren, H. R., Wolf, O. T., & Convit, A. (2008). Dissociation of cognitive and emotional empathy in adults with Asperger syndrome using the Multifaceted Empathy Test (MET). Journal of Autism and Developmental Disorders, 38(3), 464–473. https://doi.org/10.1007/s10803-007-0486-x
- Fitzgibbon, B. M., Enticott, P. G., Rich, A. N., Giummarra, M. J., Georgiou-Karistianis, N., & Bradshaw, J. L. (2012). Mirror-sensory synaesthesia: exploring “shared” sensory experiences as synaesthesia. Neuroscience & Biobehavioral Reviews, 36(1), 645–657. https://doi.org/10.1016/j.neubiorev.2011.09.006
- Giummarra, M. J., & Bradshaw, J. L. (2009). Synaesthesia for pain: Feeling pain with another. In A. Pineda (Ed.), The role of mirroring processes in social cognition (Contemporary neuroscience series) (pp. 287–307). Humana Press.
- Grice-Jackson, T., Critchley, H. D., Banissy, M. J., & Ward, J. (2017). Common and distinct neural mechanisms associated with the conscious experience of vicarious pain. Cortex, 94, 152–163. https://doi.org/10.1016/j.cortex.2017.06.015
- Ickes, W. (2001). Measuring empathic accuracy. Interpersonal Sensitivity: Theory and Measurement, 1, 219–241.
- Maister, L., Banissy, M. J., & Tsakiris, M. (2013). Mirror-touch synaesthesia changes representations of self-identity. Neuropsychologia, 51(5), 802–808. https://doi.org/10.1016/j.neuropsychologia.2013.01.020
- Martin, D., Cleghorn, E., & Ward, J. (2017). The lived experience of mirror-touch synaesthesia: A qualitative investigation of empathy and social life. Journal of Consciousness Studies, 24(1–2), 214–227.
- Martínez-Velázquez, E. S., Ahuatzin González, A. L., Chamorro, Y., & Sequeira, H. (2020). The influence of empathy trait and gender on empathic responses. A study with dynamic emotional stimulus and eye movement recordings. Frontiers in Psychology, 11, 23. https://doi.org/10.3389/fpsyg.2020.00023
- Osborn, J., & Derbyshire, S. W. (2010). Pain sensation evoked by observing injury in others. Pain, 148(2), 268–274. https://doi.org/10.1016/j.pain.2009.11.007
- Santiesteban, I., Bird, G., Tew, O., Cioffi, M. C., & Banissy, M. J. (2015). Mirror-touch synaesthesia: Difficulties inhibiting the other. Cortex, 71, 116–121. https://doi.org/10.1016/j.cortex.2015.06.019
- Santiesteban, I., Gibbard, C., Drucks, H., Clayton, N., Banissy, M. J., & Bird, G. (2021). Individuals with autism share others’ emotions: Evidence from the continuous affective rating and empathic responses (CARER) task. Journal of Autism and Developmental Disorders, 51(2), 391–404. https://doi.org/10.1007/s10803-020-04535-y
- Schönbrodt, F. D., & Perugini, M. (2013). At what sample size do correlations stabilize? Journal of Research in Personality, 47(5), 609–612. https://doi.org/10.1016/j.jrp.2013.05.009
- Singer, T., & Lamm, C. (2009). The social neuroscience of empathy. Annals of the New York Academy of Sciences, 1156(1), 81–96. https://doi.org/10.1111/j.1749-6632.2009.04418.x
- Van der Graaff, J., Meeus, W., de Wied, M., van Boxtel, A., van Lier, P. A., Koot, H. M., & Branje, S. (2016). Motor, affective and cognitive empathy in adolescence: Interrelations between facial electromyography and self-reported trait and state measures. Cognition and Emotion, 30(4), 745–761. https://doi.org/10.1080/02699931.2015.1027665
- Ward, J., & Banissy, M. J. (2015). Explaining mirror-touch synesthesia. Cognitive Neuroscience, 6(2–3), 118–133. https://doi.org/10.1080/17588928.2015.1042444
- Ward, J., Schnakenberg, P., & Banissy, M. J. (2018). The relationship between mirror-touch synaesthesia and empathy: New evidence and a new screening tool. Cognitive Neuropsychology, 35(5–6), 314–332. https://doi.org/10.1080/02643294.2018.1457017
- Wechsler, D. (2009). Wechsler memory scale (4th ed.). Pearson.