
Abstract
Background: Family socioeconomic status (SES) is related to a child’s educational success. Intermediate pathways for this relationship, such as through pubertal timing and reserve capacity, occur in adolescence.
Aim: To study whether family SES affects a child’s adult education through a psychosocial and behavioural pathway (reserve capacity) and/or a biological pathway (pubertal timing) or only through school achievement in adolescence.
Subjects and methods: Finnish adolescents sampled in five cross-sectional surveys from 1985 to 1995 (n = 37,876) were followed through the Registry of Completed Education and Degrees until 2009, when they were 29–43 years old. Family SES data also came from this registry. Structural equation modelling adjusted for ages at baseline and follow-up was used.
Results: Low family SES increased the probability of low adult education, delayed pubertal timing (in boys), weak reserve capacity and low school achievement. Reserve capacity and school achievement directly affected adult education and mediated the relationship of family SES with the outcome. Delayed pubertal timing predicted low adult education, except when school achievement was added to the model.
Conclusions: The results show that family SES affects the child’s adult education level through psychosocial and biobehavioural pathways, but the biological pathway is mediated by school achievement.
Introduction
From a developmental perspective, adolescence has a unique position in the life course because it could either lessen or aggravate the impact of early childhood disadvantages on adult outcomes (Johnson et al. Citation2011). Rapid biological and social changes such as puberty and increasing autonomy from one’s family, as well as school, peer and other environmental influences, shape socio-emotional development and lead to formation and adoption of new behaviours (Viner et al. Citation2012), consequently affecting ‘successful’ transitions into adulthood (Johnson et al. Citation2011). Hence, intermediate pathways from childhood exposures to educational trajectories may be elucidated in adolescence.
In early life, the socioeconomic status (SES) of the family is an important exposure which has been strongly linked to various developmental outcomes of children and adolescents, particularly educational attainment (Conger et al. Citation2010; Merritt and Buboltz Citation2015; Acacio-Claro et al. Citation2018). Previous research focusing on SES as a predictor of child development explained that such links probably occur through family dynamics, parenting practices and investments for children (Martin et al. Citation2010). Accordingly, higher SES families tend to invest more in the health and education of their children than lower SES families do (Conger et al. Citation2010). Research has also shown that economic hardship affects relationships between parents and children, leading to poor parenting practices or poor communication in the family, which influence the cognitive, emotional and behavioural development of children (Kroenke Citation2008; Conger et al. Citation2010).
During adolescence, one salient marker of development with effects likely persisting until adulthood is puberty, and its timing has been extensively studied due to its complex familial and environmental causes (Parent et al. Citation2003; Euling et al. Citation2008; Golub et al. Citation2008; Johnson et al. Citation2011; Graber Citation2013). The physical, behavioural and hormonal effects of puberty, particularly when occurring earlier or later than in one’s age-mates, bring psychological and adjustment issues linked to elevated symptomatology and risks of psychopathology during adolescence and other disorders in adulthood (Golub et al. Citation2008; Graber Citation2013). Higher rates of depressive symptoms, especially in girls (Copeland et al. Citation2010; Keenan et al. Citation2014), risky health behaviours (Koivusilta and Rimpelä Citation2006; Golub et al. Citation2008; Downing and Bellis Citation2009; Graber Citation2013) and higher risks for developing cardiovascular disease (Golub et al. Citation2008; Jacobsen et al. Citation2009; Lakshman et al. Citation2009; Bleil et al. Citation2013), type 2 diabetes, breast and testicular cancers (Golub et al. Citation2008) were associated with early maturation. On the other hand, late maturation increased fracture risk (Zhu and Chan Citation2017) and psychopathology in boys in terms of higher rates of depressive symptoms and disruptive behaviours (Graber Citation2013; Zhu and Chan Citation2017). Aside from its health impact, recent evidence suggests that pubertal timing has cognitive effects which may be reflected in academic performance (Cavanagh et al. Citation2007; Martin and Steinbeck Citation2017) and educational outcomes (Koivusilta and Rimpelä Citation2004; Koerselman and Pekkarinen Citation2017), influencing socioeconomic conditions in adulthood (Johnson et al. Citation2011; Koerselman and Pekkarinen Citation2017).
Secular changes observed regarding pubertal timing have been attributed mainly to improvements in nutrition and health, including an increase in body fat (de Muinich Keizer and Mul Citation2001; Parent et al. Citation2003). Pubertal timing is also influenced by certain gene regulators, gender, race/ethnicity (Obeidallah et al. Citation2000; Parent et al. Citation2003; Euling et al. Citation2008) and exposure to endocrine disrupting chemicals (Parent et al. Citation2003; Aksglaede et al. Citation2008). A stressful family environment characterised by family conflict (Bleil et al. Citation2013) and stressful life events (Sun et al. Citation2017), for example, father absenteeism, divorce and single parent families (Bellis et al. Citation2006) is likewise linked to altered pubertal timing. Notably, research has documented mixed findings of socioeconomic inequalities in timing of puberty (de Muinich Keizer and Mul Citation2001; Parent et al. Citation2003; Downing and Bellis Citation2009; James-Todd et al. Citation2010; Sun et al. Citation2017). On one hand, high SES or ‘privileged conditions’ were shown to have shifted pubertal timing towards earlier ages (de Muinich Keizer and Mul Citation2001; Parent et al. Citation2003), possibly due to improved childhood health status (de Muinich Keizer and Mul Citation2001; Bellis et al. Citation2006) and nutrition (Parent et al. Citation2003; Bellis et al. Citation2006; Kyweluk et al. Citation2018). On the other hand, low SES or childhood socioeconomic disadvantage was also found to accelerate pubertal onset (James-Todd et al. Citation2010; Sun et al. Citation2017) due to environmental stress, which hastens reproductive maturation (Obeidallah et al. Citation2000; James-Todd et al. Citation2010; Xu et al. Citation2018).
The mechanisms through which pubertal timing occurs and causes adverse health outcomes likely represent the interplay of socioeconomic, psychosocial and biobehavioural pathways in the life-course (Gallo et al. Citation2009; Matthews and Gallo, Citation2011). An integrative framework overarching this is the reserve capacity model proposed by Gallo and Matthews (Citation2003). This model posits that low SES increases one’s exposure to environmental stressors and depletes psychosocial resources such as self-efficacy, mastery and social support, triggering negative emotional and physiological responses, affecting health via altered biological and behavioural pathways (Gallo et al. Citation2009; Matthews et al. Citation2010; Matthews and Gallo Citation2011). Initially designed to understand how the psychosocial pathway links SES with physical health (Gallo and Matthews Citation2003), research which tested this model among adults produced inconclusive results about the hypothesised relationships (Matthews et al. Citation2010). However, studies conducted among children and adolescents yielded clearer directions on the connections of childhood SES and adult health outcomes through reserve capacity and biobehavioural pathways (Matthews et al. Citation2010). In addition, low SES and poor psychosocial functioning early in life placed children and adolescents at risk of lower educational outcomes compared to those with high SES and/or strong reserve capacity (Matthews et al. Citation2010).
We adopt this framework to assess whether pubertal timing and reserve capacity are such pathways through which SES influences educational trajectories. We added health-promoting behaviours, namely tooth brushing and physical activity, to the reserve capacity framework, as these underlie psychosocial resources such as perceived control and self-efficacy (Robbins et al. Citation2004; Cinar et al. Citation2009; Pakpour and Sniehotta Citation2012). Moreover, both behaviours were found to serve as pathways from childhood socioeconomic position to adult education level (Koivusilta et al. Citation2013), hence we included these variables in the present study. In this study, reserve capacity covers three dimensions, namely: perceived health, health-promoting behaviour and social support; with each dimension shown to independently predict adult education (Acacio-Claro et al. Citation2018). We also add another factor, school achievement, as several studies have shown this to be one of the strongest predictors of adult education (Slominski et al. Citation2011; Brekke Citation2015; Acacio-Claro et al. Citation2018). Further, we propose that the pathways occurring in adolescence might interact with each other to affect adult education ().
Figure 1. Conceptual model for the relationship of family SES with adult education level through adolescent pathways (biological, reserve capacity and school achievement).
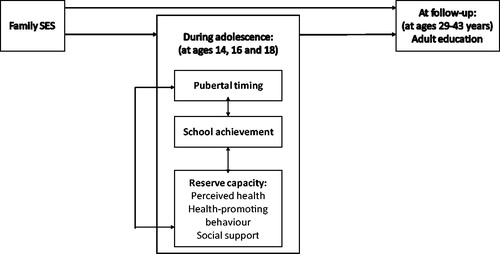
In general, we studied whether family SES affects a child’s adult education through a psychosocial and behavioural pathway (reserve capacity) and/or a biological pathway (timing of puberty) or only through school achievement in adolescence. Specifically, we want to test the following hypotheses: (1) family SES is related to pubertal timing, reserve capacity and school achievement; (2) pubertal timing and reserve capacity influence adult education level; and (3) family SES relates to adult education level directly and indirectly (i.e. mediated by any of the adolescent pathways). Understanding these mechanisms will help clarify the links among SES, adolescent pathways and adult education and point to new ways of supporting young people to achieve their full potential in learning—a recognised important life stage transition (Viner et al. Citation2012).
Subjects and methods
Study design and sample
A longitudinal study design was constructed using two data sources linked through unique national personal identification numbers. Baseline data were obtained from the Adolescent Health and Lifestyle Surveys (AHLS) of 1985, 1987, 1991, 1993 and 1995. The AHLS monitors the health and health-related lifestyle of adolescents in Finland. Nationally representative samples of 14-, 16- and 18-year-old Finns born on certain days in June, July and August between 1966 and 1980 were drawn for each study year from the Population Register Centre. Even though the AHLS has been conducted biennially since 1977, the variables suitable for measuring reserve capacity were included only in the above-mentioned years. A self-administered questionnaire, to be voluntarily answered, was sent by post in February, followed by two re-inquiries to non-respondents. The overall response rate was 79.1% (n = 37,876), with 71.9% (n = 17,531) for boys and 86.6% (n = 20,345) for girls, respectively.
Follow-up data on adult education, as well as socioeconomic information for the parents of AHLS participants, were obtained from the Registry of Completed Education and Degrees of Statistics Finland. The data from Statistics Finland covered censuses every fifth year from 1970 to 1995, and yearly registry data from 2000 until the end of 2009. At the end of 2009, the AHLS participants were aged 29–43 years.
Statistics Finland performed the data linkage according to a contract specifying the rights and duties of both parties. The Institutional Review Board of Statistics Finland and the Data Protection Ombudsman approved the study protocol. The Joint Commission on Ethics of the University of Turku and the Turku University Hospital also stated that no human rights were violated in the research protocol and approved it. Identification of the study participants was withheld from the investigators at all stages of the study.
Variables from Statistics Finland
Adult education level of the survey respondents
This is the main outcome of interest and based on the highest educational level attained by the adolescent. The exact degree codes according to the Finnish Standard Classification of Education were obtained (Statistics Finland Citation2018). We classified two groups according to years of schooling: low (≤ 9 years) to middle (10–12 years) and high education (> 12 years).
Family SES
Family SES was based on parents’ education and categorised in the same way as that of adolescents’ education. Data were obtained nearest to the year when the adolescent was aged 15 years and based on both mother’s and father’s education levels. If parents belonged to different categories, the highest was selected. If one parent had missing data, the available parent’s data were used. The minimum age of both parents was 30 years at the time their children participated in the surveys.
Variables from the surveys
Pubertal timing
To obtain an indicator of pubertal timing (biological pathway), boys were asked about their age at first ejaculation, while girls were asked about their age at menarche. Classification of pubertal timing as early, average and late followed the groupings used by Koivusilta and Rimpelä (Citation2004). In boys, the categories were chosen to be at age 12 or earlier (early), at 13 or 14 (average), and at 15 or later or if not occurred by the time of enquiry (late). In girls, the categories were at age 11 or earlier (early), at 12 or 13 (average), and at 14 or later or if not occurred by the time of enquiry (late).
Reserve capacity
Reserve capacity, spanning an underlying strong or weak construct, referred to a latent variable measured by nine observed variables in three distinct dimensions:
Perceived health dimension included three items: reported chronic disease, injury or disability that restricts daily activities (no/yes); a summary index of weekly perceived stress symptoms (stomach aches, tension or nervousness, irritability or outbursts of anger, trouble falling asleep or waking at night, headache, trembling of hands, feeling tired or weak, feeling dizzy) categorised as no symptoms, one symptom/week, 2–3/week, 4–8/week; and, self-rated health categorised as very good, average/good or poor.
Health-promoting behaviour dimension included frequency of tooth brushing (several times a day, once a day, 1–5 times/week or less) and efficiency of physical activity. Efficiency of physical activity was measured by combining information from two variables: frequency of physical activity in leisure time and intensity of exercise (shortness of breath/sweating). This combination used the following categories: does not exercise; exercises with low/occasional efficiency; active efficient exerciser; very active efficient exerciser.
Social support dimension was measured using four items: nuclear family (living with both parents or not); ease of talking about troubling issues to father; to mother; and to friends (easy, difficult or very difficult). Those who did not have a father (5.2%), mother (1%) or friends (0.5%) were included in the ‘very difficult’ category.
School achievement
For school achievement, adolescents were categorised based on self-assessment of their school performance as having: highest, 2nd highest, 2nd lowest or lowest academic achievement. The 14-year-old respondents (in comprehensive schools) were asked to assess whether their end-of-term school report was much better (highest), slightly better (2nd highest), average (2nd lowest), slightly poorer or much poorer (lowest) than the class average. For 16–18-year-olds, in addition to their self-assessment, school status (academic upper secondary school/vocational school/not attending school) was also used. Their achievement was classified as follows: highest (in academic upper secondary school with better performance); 2nd highest (in vocational school with better performance or academic upper secondary school with average performance); 2nd lowest (in vocational school with poor to average performance or high school with poor performance); and lowest (not at school).
Statistical analysis
We used confirmatory factor analysis (CFA) to estimate the underlying construct of ‘reserve capacity’ and create a general, continuous latent variable from the nine measured variables: presence of chronic disease; perceived stress symptoms; self-rated health; physical activity; regular tooth brushing; nuclear family; talking to father; talking to mother; and talking to friends. We included covariances among variables within each dimension. We also fixed the value of the variance of the latent variable at one to freely estimate the factor loadings for all the variables.
To analyse the mechanisms by which SES, puberty, reserve capacity and school achievement influence adult education level, we used structural equation modelling (SEM). This enabled the inclusion of latent effects and testing of multiple pathways simultaneously (Grace and Bollen Citation2005). SEM is composed of both a measurement model and a structural model. The measurement model is given by CFA, which shows how observed or measured variables relate to latent variables. The structural model describes the relationships among the variables, including the latent variables, through a set of regression equations (Muthén and Muthén Citation2012). In our study, the resulting estimates were probit coefficients, which are effects on a cumulative normal function of the probabilities that the response variable equals one (Muthén and Muthén Citation2012). We assigned a value of one to an outcome of low-to-middle adult education; thus, we predict this probability given a low family SES, delayed pubertal timing, weak reserve capacity and low school achievement.
Models were fitted separately for each sex group and adjusted for both baseline age and age at follow-up. Since we wanted to assess if pubertal timing independently influenced the outcome, we initially tested for the effects of SES and puberty only (Model 1), then added reserve capacity (Model 2) and finally, school achievement (Model 3). All models were estimated using a robust weighted least squares estimator, under missing data theory which used all available data. In such analyses, missingness was allowed to be a function of the observed covariates, but not the observed outcome (Muthén and Muthén Citation2012). Fit of the CFA and full models (Model 3) were assessed using the root mean square error of approximation (RMSEA) and the comparative fit index (CFI). RMSEA values < 0.08 and < 0.06 imply acceptable and good fits, respectively. Similarly, CFI values > 0.90 and > 0.95 imply acceptable and good fits, respectively (Hooper et al. Citation2007). Mplus 7.11 was used for both CFA and SEM analyses.
Results
Sample characteristics
presents the descriptive characteristics of the adolescents in the sample according to the main variables. The proportions of those who had low-to-middle adult education largely exceeded those who had high education among boys (70.1%) and girls (59.3%). The majority of adolescents with low-to-middle adult education had parents with similarly attained education. Among those with available data, the average age of pubertal onset for boys was 13.1 ± 1.3 years, while for girls it was 12.6 ± 1.1 years. In terms of reserve capacity, there were higher proportions of adolescents with very good self-rated health, better health-promoting behaviours, presence of nuclear families and ease of communication with parents and friends among those with high adult education compared to those with low education. The same pattern was observed in the distribution of school achievement.
Table 1. Characteristics of participants according to sex group and adult education level.
CFA results
Preliminary analyses showed that all factor loadings of the nine variables were statistically significant and the positive coefficients implied that each observed variable directly relates with latent reserve capacity (). Larger factor loadings reflect greater degrees of relationship with the latent variable. Among the nine variables, perceived stress symptoms and self-rated health, both of which are included in the perceived health dimension, contributed most to the measurement of the latent reserve capacity in both boys and girls. The estimated coefficients for the covariances indicate the relationship of variables with one another. showed that grouped variables had statistically significant covariances, implying that the observed variables were related within each dimension. RMSEA and CFI values signified good fit for our measurement models. Thus, the hypothesised reserve capacity framework in our study was consistent with observed data and provided support for our models in both boys and girls. The relationship of latent reserve capacity with other variables in the study is also illustrated in the bottom parts of and .
Figure 2. Boys: Structural equation model depicting relationships among family socioeconomic status (SES), pubertal timing, school achievement and reserve capacity in adolescence and adult education level (RMSEA = 0.05; CFI = 0.90). The values along the paths are standardised regression coefficients. Solid lines indicate statistically significant paths (p < 0.001).
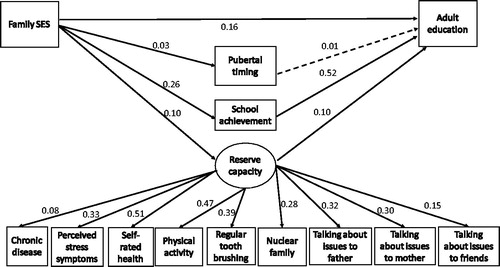
Figure 3. Girls: Structural equation model depicting relationships among family socioeconomic status (SES), pubertal timing, school achievement and reserve capacity in adolescence and adult education level (RMSEA = 0.04; CFI = 0.91). The values along the paths are standardised regression coefficients. Solid lines indicate statistically significant paths (p < 0.001).
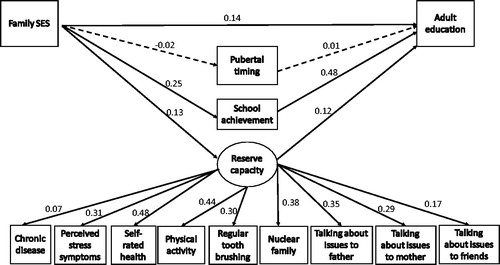
Table 2. Results from confirmatory factor analyses (CFA) of reserve capacity model regressed on nine observed variables presented as standardised (β) coefficients.
SEM analyses
To disentangle the influence of the biological pathway from those of other intermediate pathways, we assessed how effects of puberty on adult education vary when only family SES was considered (model 1), then reserve capacity (model 2) and school achievement (model 3) were sequentially added (). Results showed that delayed pubertal timing increased the probability of low adult education in boys (models 1 and 2), but lost statistical significance once the school achievement pathway was included. On the other hand, family SES consistently predicted the probability of adult education, regardless of adolescent pathways added into the models in both boys and girls.
Table 3. Direct effects of family SES and biological pathway on adult education level in a structural equation model presented as standardised (β) coefficients.
Model 3 is referred to as the full model and is illustrated in and . To simplify the model presentations, estimates relating to age variables and their covariances, along with covariances among adolescent pathways and among variables within the same dimension of reserve capacity, were not shown.
Detailed results from SEM analyses of the full model depicting relationships among family SES, pubertal timing, school achievement and reserve capacity, while additionally controlling for age at baseline and at follow-up, showed that the models in both population groups ( and ) fit the data well based on the presented fit indices. The hypothesised pathways are described further below.
Hypothesis 1: Family SES is related to pubertal timing, reserve capacity and school achievement
This hypothesis was fully supported by the model in boys (). Direct paths from family SES to the following factors: pubertal timing (β = 0.03), reserve capacity (β = 0.10) and school achievement (β = 0.26) were all statistically significant (p < 0.001). The results in girls () partially supported this hypothesis, which showed only the pathways from family SES to reserve capacity (β = 0.13, p < 0.001) and from family SES to school achievement (β = 0.25, p < 0.001), as statistically significant. On the other hand, the relationship of family SES to girl’s pubertal timing differed from that found in boys. Among girls, a low family SES (β = –0.02, p = 0.05) decreased the probability of delayed pubertal timing.
Hypothesis 2: Pubertal timing and reserve capacity influence adult education level
This hypothesis was also partially supported by the results. and illustrate statistically significant paths from reserve capacity to adult education in boys (β = 0.10, p < 0.001) and girls (β = 0.12, p < 0.001), respectively. While, the paths from pubertal timing to adult education were not statistically significant, a positive coefficient (β = 0.01) indicated a direct relationship between delayed pubertal timing and low-to-middle education in both boys and girls.
Hypothesis 3: Family SES relates to adult education level directly and indirectly
The results for boys () and girls () fully support this hypothesis as direct pathways from family SES to adult education in both boys (β = 0.16, p < 0.001) and girls (β = 0.14, p < 0.001) were statistically significant. Estimation of indirect paths in showed that the effect of family SES on adult education is significantly mediated by reserve capacity (boys: β = 0.01; girls: β = 0.02; p < 0.001) and school achievement (boys: β = 0.14; girls: β = 0.12; p < 0.001) in the two groups. No mediation via pubertal timing was observed.
Table 4. Estimated indirect effects of family SES through adolescent pathways and the covariances among these pathways in the final structural equation model presented as standardised (β) coefficients.
How school achievement fits
Direct paths from school achievement to adult education level, as shown in and , were statistically significant in both boys (β = 0.52; p < 0.001) and girls (β = 0.48; p < 0.001), respectively. We also found statistically significant covariances among pubertal timing, reserve capacity and school achievement in boys, while, in girls, similar statistically significant covariances existed, except between pubertal timing and school achievement ().
The covariances indicate the direction of the relationship between the variables. As shown in , pubertal timing had a negative relationship with reserve capacity, but a positive relationship with school achievement. In our study, this means that delayed pubertal timing was related to better reserve capacity in both boys and girls, but lower school achievement in boys. On the other hand, a weak reserve capacity was related to low school achievement.
Discussion
Summary and interpretation of results
We investigated the relationships among family SES, the intermediate pathways in adolescence and adult education. We found that family SES directly predicted the measured adolescent pathways (except biological pathway in girls) and adult education. Reserve capacity and school achievement directly influenced adult education and mediated the relationship between family SES and adult education. Although we did not find statistical significance for the path between pubertal timing and adult education, unadjusted results suggested that delayed pubertal timing might be a risk for having low-to-middle adult education in both boys and girls. Additionally, we found that pubertal timing, reserve capacity and school achievement were inter-related, providing empirical evidence on how mechanisms in adolescence work to influence educational outcomes.
Clearly, our study showed that family SES predicted the adolescents’ educational outcomes, directly and indirectly, via pathways of reserve capacity and school achievement. The significant effect of SES on adult education implies that educational inequalities existed in our setting. This is comparable with analyses of more current data attributed to the rising income inequality observed in the region within recent years (OECD Citation2018). On the other hand, research also showed that higher levels of social mobility occur in welfare Scandinavian societies such as Finland, where the economic inequality gap is narrower than in many other countries (OECD Citation2018). Indeed, we observed greater upward social mobility where children born into low SES families ended up in higher SES than their parents ().
The revealed indirect pathways of SES supported previous knowledge that SES affects life-course developments such as psychosocial, behavioural and cognitive functioning (Kroenke Citation2008; Conger et al. Citation2010). We can infer that the parents’ SES influenced the reserve capacity and school achievement of the adolescents probably through family dynamics such as family stress processes and parenting practices including cognitive stimulation and parental investments for education (Conger et al. Citation2010; Martin et al. Citation2010). The adolescents with stronger reserve capacity and higher school achievement than their peers may have utilised their cognitive abilities, psychosocial and behavioural resources to cope with academic transitions and attain higher education and, consequently, better SES in the future. As one study showed, the pursuit of higher education, controlling for social origin, was dependent on academic motivation and abilities and subjective expectations and evaluations of return of investments on higher education (Becker and Hecken Citation2009).
Like Obeidallah et al. (2000), we did not observe a statistically significant direct effect of family SES on menarche. On the other hand, we found that a low family SES increased the probability of delayed pubertal timing in boys. Our results supported previous findings which had documented inverse associations between SES and pubertal onset within populations (de Muinich Keizer and Mul Citation2001; Parent et al. Citation2003). Living in low socioeconomic conditions might delay puberty because of a higher likelihood of malnutrition, acute or chronic illnesses and the presence of other adverse physical or psychological conditions compared to those living in privileged environments (Parent et al. Citation2003). In contrast, recent evidence revealed that low family SES markedly increased rates of early puberty in both boys and girls (Downing and Bellis Citation2009; Sun et al. Citation2017), possibly through interactions with biological systems regulating pubertal timing (Sun et al. Citation2017) or other risk factors such as having a higher body mass index (BMI) or being overweight (Downing and Bellis Citation2009; James-Todd et al. Citation2010) and experiencing stressful life events (James-Todd et al. Citation2010). However, a meta-analysis of studies among males found no significant association between family SES and pubertal timing (Xu et al. Citation2018). Since there is limited research on determinants of pubertal onset among boys, the processes influencing male pubertal development were much less understood (Graber Citation2013). We conclude that the inconsistent relationship of family SES with pubertal timing probably reflected inherent differences in study populations such as ethnic and geographic variations, gender and genetic predisposition and changes in underlying mechanisms influenced by SES to activate puberty such as intrauterine conditions, health, nutrition, stress and environmental exposures (Parent et al. Citation2003). Other methodological issues including differences in study designs and measurement of SES and pubertal timing indicators (Xu et al. Citation2018) might have contributed to this inconsistency.
In our study, low family SES increased the probability of having weak reserve capacity brought about by poor perceived health, health-promoting behaviour and social support. Our findings are congruent with previous evidence, albeit reserve capacity was measured using purely psychosocial resources (Kroenke Citation2008; Matthews and Gallo Citation2011). According to Gallo and Matthews (Citation2003), low-SES individuals have weaker reserve capacity due to frequent exposure to situations requiring use of their psychosocial resources and their environments inhibit them from developing and replenishing these resources ‘to be kept in reserve’. While reserve capacity was initially conceptualised as a potential mediating pathway in SES-health inequalities (Gallo et al. Citation2009), we have shown that it also served as a pathway connecting one’s family SES to future adult education. Indeed, an indirect effect of family SES through this pathway was statistically significant in both boys and girls. We believe that dealing with school transitions, along with puberty during adolescence, constantly requires the use of one’s reserve capacity. This may be implied in the reported covariances between reserve capacity and pubertal timing. Thus, those with low SES and weak reserve capacity might have educational transition difficulties. It has also been suggested that individuals with weak reserve capacity may lack the coping skills needed to attain higher education (Matthews et al. Citation2010). The observed direct effect of reserve capacity on adult education in our study supported this logic.
Partitioning the full model showed that delayed pubertal timing, along with family SES and reserve capacity, increased the probability of having low-to-middle education in both boys and girls. However, when we included school achievement in the model, pubertal timing lost its statistically significant effect on adult education. Instead, pubertal timing was more related with school achievement, especially in boys (based on the reported covariance), than with adult education. One study explained that pubertal status did not directly predict academic achievement, but rather influenced academic motivation, which then affected academic achievement (Martin and Steinbeck Citation2017). Our results replicate the findings from a British cohort study which showed that late pubertal development was associated with lower levels of educational attainment, but the said association weakened when test scores at age 16 years were factored in (Koerselman and Pekkarinen Citation2017).
While our results for girls showed no association between pubertal timing and adult education, other evidence has presented contrary findings (Hendrick et al. Citation2016; Gill et al. Citation2017). Previous research has shown that early maturing girls had a higher probability of being high school dropouts (Cavanagh et al. Citation2007; Hendrick et al. Citation2016) or having low-grade point averages (GPA) at the end of high school (Cavanagh et al. Citation2007). Gill et al. (2017) found that menarche occurring at later ages increased the schooling period. However, most studies have suggested that, beyond high school, the impact of early pubertal timing on educational outcomes ceases (Copeland et al. Citation2010; Hendrick et al. Citation2016). Still, as research on educational outcomes related to pubertal timing is relatively scarce, variations in the results of these studies imply that pubertal timing coincides with cognitive development in adolescence (Viner et al. Citation2012; Koerselman and Pekkarinen Citation2017), and likely interacts with structural and behavioural mechanisms to predict educational attainment (Johnson et al. Citation2011).
As shown in previous studies (Slominski et al. Citation2011; Brekke Citation2015; Acacio-Claro et al. Citation2018), school achievement has the largest effect on adult education. This is to be expected, as good grades obtained in high school strongly predicted enrolment in higher education (Brekke Citation2015). In fact, Entwisle et al. (Citation2005) demonstrated that academic performance as early as first grade influenced educational attainment. Our results also point to the direct role of family SES in predicting school achievement. Indeed, socioeconomic disparities in school achievement probably occur because material deprivation and low SES may reduce human capital investments of parents for their children, including cognitive stimulation, thus affecting their cognitive development (Kroenke Citation2008; Conger et al., Citation2010).
Strengths and limitations of the study
Using large, nationwide samples with good response rates, a long follow-up period and reliable register-based data allowed us to test our hypotheses about multiple direct and mediating pathways for the outcome of interest. Since no specific set of psychosocial resources comprise reserve capacity, our study expanded the concept of reserve capacity with the addition of health-promoting behaviours. We needed to use proxy indicators, whereas related studies had used psychological scales or other structured tools, because reserve capacity was conceptualised at a much later time than when our surveys were conducted. Nevertheless, we have measured a valid construct as proven by the good fit indices obtained for this latent variable.
We have identified intermediate adolescent pathways (pubertal timing, reserve capacity and school achievement) which account for the relationship of family SES with adult education. Even though our models had good fit, we recognise that there are other structural and individual factors that have not been measured in our study which could be probable pathways through which SES influences adult education. For instance, schools, neighbourhood and peers also affect adolescents’ learning potential and, consequently, one’s transition to adulthood (Viner et al. Citation2012). However, our data were not obtained from school-based or community-based surveys, so analysing those effects were beyond the scope of this study.
We acknowledge some methodological limitations related to one of the pathways and the outcome variable studied. Age at spermarche or first ejaculation may not be an accurate indicator of pubertal onset, due to a high number of false negative results (Euling et al. Citation2008), which possibly diluted the effect of boys’ pubertal timing on adult education level in our study. The use of additional puberty markers, such as Tanner staging based on the appearance of secondary sexual characteristics, either through self-assessment or staging by a professional, was recommended for collection of puberty data (Euling et al. Citation2008), although this was not possible through mailed questionnaires. Still, the pubertal timing ages estimated in our study population closely resembled those described in other European countries which used more accurate staging methods for the same period (de Muinich Keizer and Mul Citation2001). For the outcome, we initially tried to use three categories of education (low, middle and high) where SEM results are ordered logistic regression coefficients. However, our current data did not support the proportional odds assumption required for the ordered three-category outcome. On the other hand, treating the categories as unordered or multinomial did not allow assessment of indirect effects, which is one of our main hypotheses. Thus, we decided to dichotomise adult education. Future research should assess if similar pathways operate for other categories of education such as middle education.
Generally our results, which expand on the work of earlier studies (Koivusilta and Rimpelä Citation2004, Acacio-Claro et al. Citation2018), have shown similar patterns, even with the different methodological techniques used (i.e. using a longer follow-up period and different analytic procedures), thus adding to the robustness and reliability of our study.
Conclusion
Our study underscores the role of family SES in predicting intermediate pathways in adolescence and adult education. Moreover, we elucidated the interplay of these pathways (pubertal timing, reserve capacity and school achievement) in influencing educational trajectories and mediating the effect of family SES on adult education. As important learning and school transitions occur during adolescence, which impact future adult education, support should be given to young people to help them adjust and cope well with various physical, behavioural and psychosocial developmental changes.
Acknowledgements
The authors thank Statistics Finland for access to their data and Lasse Pere for assistance in data management.
Disclosure statement
The authors report no conflict of interest.
Data Availability Statement
The data that support the findings of this study are not available for replication outside members of the research group due to contract specifications with Statistics Finland. The computing code or syntax for analyses are not useful without the data, but these may be shared upon request. However, we welcome other researchers to join our team in Tampere for further analyses of the data.
Additional information
Funding
References
- Acacio-Claro P, Doku DT, Koivusilta LK, Rimpelä AH. 2018. How socioeconomic circumstances, school achievement and reserve capacity in adolescence predict adult education level: a three-generation study in Finland. Int J Adolesc Youth. 23:382–397.
- Aksglaede L, Olsen LW, Sørensen TIA, Juul A. 2008. Forty years trends in timing of pubertal growth spurt in 157,000 Danish school children. Plos One. 3:e2728.
- Becker R, Hecken AE. 2009. Higher education or vocational training? An empirical test of the rational action model of educational choices suggested by Breen and Goldthorpe and Esser. Acta Sociol. 52:25–45.
- Bellis MA, Downing J, Ashton JA. 2006. Adults at 12? Trends in puberty and their public health consequences. J Epidemiol Commun Health. 60:910–911.
- Bleil ME, Adler NE, Appelhans BM, Gregorich SE, Sternfeld B, Cedars MI. 2013. Childhood adversity and pubertal timing: Understanding the origins of adulthood cardiovascular risk. Biol Psychol 93:213–219.
- Brekke I. 2015. Health and educational success in adolescents: A longitudinal study. BMC Public Health 15:619.
- Cavanagh SE, Riegle-Crumb C, Crosnoe R. 2007. Puberty and the education of Girls*. Soc Psychol Q. 70:186–198.
- Cinar AB, Tseveenjav B, Murtomaa H. 2009. Oral health-related self-efficacy beliefs and toothbrushing: Finnish and Turkish pre-adolescents' and their mothers' responses. Oral Health Prev Dent. 7:173–181.
- Conger RD, Conger KJ, Martin MJ. 2010. Socioeconomic status, family processes, and individual development. J Marriage Fam. 72:685–704.
- Copeland W, Shanahan L, Miller S, Costello EJ, Angold A, Maughan B. 2010. Outcomes of early pubertal timing in young women: a prospective population-based study. Am J Psychiatry. 167:1218–1225.
- de Muinich Keizer SM, Mul D. 2001. Trends in pubertal development in Europe. Hum Reprod Update 7:287–291.
- Downing J, Bellis M. 2009. Early pubertal onset and its relationship with sexual risk taking, substance use and anti-social behaviour: A preliminary cross-sectional study. BMC Public Health 9:446.
- Entwisle D, Alexander K, Olson L. 2005. First grade and educational attainment by age 22: a new story. American Journal of Sociology 110:1458–1502.
- Euling SY, Herman-Giddens ME, Lee PA, Selevan SG, Juul A, Sorensen TI, Dunkel L, et al. 2008. Examination of US puberty-timing data from 1940 to 1994 for secular trends: panel findings. Pediatrics 121 Suppl 3: S172–S191.
- Gallo LC, Matthews KA. 2003. Understanding the association between socioeconomic status and physical health: Do negative emotions play a role? Psychol Bull 129:10–51.
- Gallo LC, Espinosa de los Monteros K, Shivpuri S. 2009. Socioeconomic status and health: What is the role of reserve capacity? Curr Directions Psychol Sci 18:269–274.
- Gill D, Del GM, Rawson TM, Sivakumaran P, Brown A, Sheehan NA, Minelli C. 2017. Age at menarche and time spent in education: a mendelian randomization study. Behav Genet 47:480–485.
- Golub MS, Collman GW, Foster PMD, Kimmel CA, Rajpert-De Meyts E, Reiter EO, Sharpe RM, et al. 2008. Public health implications of altered puberty timing. Pediatrics 121:S218–S230.
- Graber JA. 2013. Pubertal timing and the development of psychopathology in adolescence and beyond. Horm Behav 64:262–269.
- Grace JB, Bollen KA. 2005. Interpreting the results from multiple regression and structural equation models. Bull Ecol Soc Am 86:283–295.2.0.CO;2.
- Hendrick CE, Cohen AK, Deardorff J, Cance JD. 2016. Biological and sociocultural factors during the school years predicting women's lifetime educational attainment. J Sch Health 86:215–224.
- Hooper D, Coughlan J, Mullen MR. 2007. Structural equation modeling: guidelines for determining model fit. The Electronic Journal of Business Research Methods 6:53–60.
- Jacobsen BK, Oda K, Knutsen SF, Fraser GE. 2009. Age at menarche, total mortality and mortality from ischaemic heart disease and stroke: the Adventist health study, 1976-88. Int J Epidemiol 38:245–252.
- James-Todd T, Tehranifar P, Rich-Edwards J, Titievsky L, Terry MB. 2010. The impact of socioeconomic status across early life on age at menarche among a racially diverse population of girls. Ann Epidemiol 20:836–842.
- Johnson MK, Robert C, Elder GH. 2011. Insights on adolescence from a life course perspective. J Res Adolesc 21:273–280.
- Keenan K, Culbert KM, Grimm KJ, Hipwell AE, Stepp SD. 2014. Timing and tempo: Exploring the complex association between pubertal development and depression in African American and European American girls. J Abnorm Psychol 123:725–736.
- Koerselman K, Pekkarinen T. 2017. The timing of puberty and gender differences in educational achievement. Bonn, Germany: IZA Institute of Labor Economics initiated by Deutsche Post Foundation. Report nr IZA DP No. 10889.
- Koivusilta L, Rimpelä A. 2004. Pubertal timing and educational careers: A longitudinal study. Ann Hum Biol 31:446–465.
- Koivusilta LK, Rimpelä AH. 2006. Pubertal timing and health-related behaviours in adolescence - socio-economic outcomes in a follow-up study from Finland. Italian Journal of Public Health 3:41–52.
- Koivusilta L, West P, Saaristo VMA, Nummi T, Rimpela A. 2013. From childhood socio-economic position to adult educational level - do health behaviours in adolescence matter? A longitudinal study. BMC Public Health 13:711.
- Kroenke C. 2008. Socioeconomic status and health: Youth development and neomaterialist and psychosocial mechanisms. Soc Sci Med 66:31–42.
- Kyweluk MA, Georgiev AV, Borja JB, Gettler LT, Kuzawa CW. 2018. Menarcheal timing is accelerated by favorable nutrition but unrelated to developmental cues of mortality or familial instability in Cebu, Philippines. Evolution and Human Behavior 39:76–81.
- Lakshman R, Forouhi NG, Sharp SJ, Luben R, Bingham SA, Khaw KT, Wareham NJ, Ong KK. 2009. Early age at menarche associated with cardiovascular disease and mortality. J Clin Endocrinol Metab. 94:4953–4960.
- Martin AJ, Steinbeck K. 2017. The role of puberty in students’ academic motivation and achievement. Learn Individual Differences. 53:37–46.
- Martin MJ, Conger RD, Schofield TJ, Dogan SJ, Widaman KF, Donnellan MB, Neppl TK. 2010. Evaluation of the interactionist model of socioeconomic status and problem behavior: a developmental cascade across generations. Dev Psychopathol. 22:695–713.
- Matthews KA, Gallo LC. 2011. Psychological perspectives on pathways linking socioeconomic status and physical health. Annu Rev Psychol. 62:501–530.
- Matthews KA, Gallo LC, Taylor SE. 2010. Are psychosocial factors mediators of socioeconomic status and health connections? A progress report and blueprint for the future. Ann N Y Acad Sci. 1186:146–173.
- Merritt DL, Buboltz W. 2015. Academic success in college: Socioeconomic status and parental influence as predictors of outcome. Open J Soc Sci. 03:127–135.
- Muthén LK, Muthén BO. 1998-2012. Mplus User’s guide. 7th ed. Los Angeles, CA.: Muthén & Muthén.
- Obeidallah DA, Brennan RT, Brooks-Gunn J, Kindlon D, Earls F. 2000. Socioeconomic status, race, and girls’ pubertal maturation: results from the project on human development in Chicago neighborhoods. J Res Adolesc. 10:443–464.
- Organisation for Economic Cooperation and Development [OECD]. 2018. Equity in education: breaking down barriers to social mobility. Paris: PISA, OECD Publishing.
- Pakpour AH, Sniehotta FF. 2012. Perceived behavioural control and coping planning predict dental brushing behaviour among Iranian adolescents. J Clin Periodontol. 39:132–137.
- Parent A, Teilmann G, Juul A, Skakkebaek NE, Toppari J, Bourguignon J. 2003. The timing of normal puberty and the age limits of sexual precocity: Variations around the world, secular trends, and changes after migration. Endocr Rev. 24:668–693.
- Robbins LB, Pender NJ, Ronis DL, Kazanis AS, Pis MB. 2004. Physical activity, self-efficacy, and perceived exertion among adolescents. Res Nurs Health 27:435–446.
- Slominski L, Sameroff A, Rosenblum K, Kasser T. 2011. Longitudinal predictors of adult socioeconomic attainment: The roles of socioeconomic status, academic competence, and mental health. Dev Psychopathol 23:315–324.
- Statistics Finland. Finnish Standard Classification of Education 2011 [Internet]; c2018. Available from: http://www.stat.fi/meta/luokitukset/koulutus/001-2011/index_en.html.
- Sun Y, Mensah FK, Azzopardi P, Patton GC, Wake M. 2017. Childhood social disadvantage and pubertal timing: A national birth cohort from Australia. Pediatrics 139. http://doi.org/10.1542/peds.2016-4099
- Viner RM, Ozer EM, Denny S, Marmot M, Resnick M, Fatusi A, Currie C. 2012. Adolescence and the social determinants of health. The Lancet 379:1641–1652.
- Xu Y, Norton S, Rahman Q. 2018. Early life conditions, reproductive and sexuality-related life history outcomes among human males: A systematic review and meta-analysis. Evol Hum Behav 39:40–51.
- Zhu J, Chan Y. 2017. Adult consequences of self-limited delayed puberty. Pediatrics 139:e20163177.