
Abstract
Due to loss of spoken language and resulting complex communication needs, people with Rett syndrome are obvious candidates for communication intervention. To advance evidence-based practice and guide future research efforts, we identified and summarized 16 communication intervention studies published since a previous 2009 review on this topic. Studies were summarized in terms of (a) participants, (b) dependent variables related to communication, (c) intervention characteristics, (d) outcomes, and (e) certainty of evidence. Across the 16 studies, intervention was provided to a total of 100 participants from 3 to 47 years of age. Half of the studies used systematic instruction to teach aided AAC. Other interventions and associated technologies included music therapy, eye tracking technology, and transcranial stimulation. Positive outcomes (e.g., using AAC devices to make requests and/or initiate social-communication interactions) were reported in 13 of the studies. These 16 new studies provide additional guidance on how to enhance the communicative functioning of people with Rett syndrome. Future research directions are highlighted.
Rett syndrome is an X-linked genetic disorder associated with severe developmental regression (Amir et al., Citation1999; Neul et al., Citation2010; Sandweiss et al., Citation2020). While it does rarely occur in males (Reichow et al., Citation2015), it is considerably more prevalent in females; approximately 1 case for every 10,000 female births (Fehr et al., Citation2011). At this prevalence rate, Rett syndrome appears to be the single most common cause of profound/multiple disability in girls (Smeets et al., Citation2012; Tarquinio & Percy, Citation2016).
In many cases the diagnosis can be confirmed due to mutations on the MECP2 gene (Amir et al., Citation1999). Regression usually begins early (between 6 and 18 months of age) and progresses rapidly, leading almost always to significant impairments by 4 years of age (Einspieler & Marschik, Citation2019; Foxe et al., Citation2016). The developmental course of Rett syndrome has been characterized in terms of four clinical stages (Fabio et al., Citation2020; Neul et al., Citation2010; Percy & Glaze, Citation2017). Generally, it is at Stage I—from about 6 to 18 months of age—when concerns such as poor muscle tone and delayed motor development might first be noticed. Next, from about 1 to 3 years of age (Stage II) the children often show developmental regression along with appearance of seizures (usually after age 2), acquired microcephaly, hyperventilation, scoliosis, loss of purposeful hand use, and emergence of stereotyped hand mannerisms. As the child ages and progresses to Stages III and Stage IV, most children will eventually present with significant communication and motor impairments. In addition, scoliosis has been estimated to occur in 85% of individuals by 16 years of age (Percy & Glaze, Citation2017).
In addition to these clinical stages, two main types of Rett syndrome have been identified: classic and atypical (Operto et al., Citation2019). With certain atypical variants there can be some preserved speech and greater motor/ambulation ability (Marschik et al., Citation2014; Skjeldal, Citation2020). In terms of evaluating interventions aimed at enhancing the functioning of people with Rett syndrome, it might be of some importance to ascertain the participants’ type and stage of Rett syndrome. Interventions effective for children in Stage III, for example, might not be useful at Stage II; however, there does not appear to be any research demonstrating intervention by type/stage interactions.
A number of studies have reported on the extent of spoken language abilities that remain as the disease progresses. Neul et al. (Citation2014), for example, reported that the ability to communicate using phrases and single words was lost by nearly all the 638 females with both classic (n = 542) and atypical (n = 96) Rett syndrome in their longitudinal study. This finding is consistent with multiple other reports indicating that regressive (and extensive) loss of spoken language ability occurs for most children with both classic and atypical Rett syndrome (Bartolotta et al., Citation2011; Foxe et al., Citation2016; Hagberg, Citation2002; Marschik et al., Citation2014).
In light of these reports of significant spoken language impairment, it is not surprising that communication intervention, including augmentative and alternative communication (AAC) intervention, is a major treatment priority for people with Rett syndrome (Larriba-Quest et al., Citation2020). In short, people with Rett syndrome have complex communication needs and are likely to require extensive communication supports, including interventions aimed at teaching alternatives to speech (Light & McNaughton, Citation2011) and/or interventions aimed at expanding and strengthening the person’s existing communication skills (Julien et al., Citation2015).
Meeting the communication needs of people with Rett syndrome is likely to be challenging due to several unique characteristics associated with this condition. Along with communication and motor difficulties—which are challenging in their own right—Rett syndrome is also characterized by scoliosis, seizures, fluctuating levels of alertness, loss of purposeful hand use, and emergence of stereotyped mannerisms, such as hand mouthing, clapping, and wringing/washing-like hand movements (Ferreira & Teive, Citation2020; Neul et al., Citation2010). This latter characteristic will likely complicate and perhaps even contraindicate the use of certain alternative communication modes that require precise voluntary control of the fingers, hands, and/or arms, such as manual signing, picture exchange, and pointing to graphic symbols.
Given these unique challenges, an important question is whether there are in fact any empirically-validated (and successful) interventions for enhancing the communication functioning of people with Rett syndrome. A 2009 review by Sigafoos et al. offered a preliminary answer to this question. That review identified nine studies that collectively provided communication intervention to 31 children (from 2 to 17 years of age) with Rett syndrome. Three communication modes (i.e., speech, gestures, and selection of graphic symbols from a communication board or speech-generating device) were targeted for instruction across the nine studies. Participants were taught to use the targeted communication mode for a range of functions, primarily (a) requesting preferred objects/interaction, (b) naming/commenting, (c) imitating speech, and (d) receptive language tasks (e.g., responding to another’s request, answering questions, and pointing to named symbols). Intervention generally involved applying systematic instructional tactics (e.g., response prompting and reinforcement) or following a general therapeutic approach, such as providing music therapy or early intensive behavioral intervention. Improved communication outcomes (e.g., increased used of AAC symbols to make choices, request preferred objects, comment, name pictures, and respond to questions) were reported for 24 of the 31 children (84%); however, methodological limitations rendered the results inconclusive for all but one of the studies and that study had a sample size of only three children; thus, as of 2009, there were relatively few studies on providing communication intervention to people with Rett syndrome and most of these had methodological limitations.
The present paper updates the earlier (2009) review by examining studies published from 2010 to 2022. The general aim of this review was to document the extent and nature of current communication intervention literature for people with Rett syndrome. The specific aims were to (a) ascertain what, if any, new data are available on intervening to enhance the communication functioning of people with Rett syndrome; and (b) provide a narrative summary of the studies carried out in the area. Of particular interest was whether studies provided more conclusive evidence related to some of the promising practices identified in the 2009 review. Of additional interest was whether the ensuing 12 years had resulted in any significant advances in the literature, such as expansion of the literature to adults and to a wider range of communication modes and functions. An updated review of this type could facilitate practice and stimulate future research on communicative supports for people with Rett syndrome.
Method
The procedures adopted for this review were informed by the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA; Page et al., Citation2021).
Inclusion and exclusion criteria
To be included in this review, the study had to have evaluated the effects of an intervention that was aimed at teaching, increasing, and/or strengthening one or more areas of communication functioning. The intervention also had to have been applied to at least one person with Rett syndrome. Communication intervention was defined as implementing one or more therapeutic/teaching procedures for the purpose of trying to increase or improve the person’s communicative functioning, skills, or abilities. Intervention studies not specifically focused on teaching or increasing communication skills, but which included at least one dependent variable related to communicative functioning (e.g., scores on a standardized measure of receptive and expressive communication), were included.
A number of exclusion criteria were applied. Review papers and papers providing general intervention guidance, but which did not evaluate the effects of an intervention, were excluded. Studies that assessed or described the communication abilities, skills, and/or needs of people with Rett syndrome (e.g., assessing choice making abilities) without providing an intervention to develop or teach communication skills were also excluded. This exclusion extended to studies that made use of the child’s existing communication skills during an assessment. Studies that focused on the perceptions and/or experiences of parents/caregivers or professionals regarding the use of a particular communication intervention or method (e.g., parents’ perceptions and experiences with eye gaze technology) were excluded. Finally, studies that included participants both with and without Rett syndrome were excluded if it was not possible to isolate the results for the participants with Rett syndrome (e.g., if only means for the overall participant pool were reported).
Search and screening methods
Searches were undertaken in the following five electronic databases: Cumulative Index of Nursing and Allied Health Literatures (CINAHL), Education Resources Information Center (ERIC), Linguistics and Language Behavior Abstracts (LLBA), Medline, and PsycInfo. The search was limited to peer-reviewed journal articles published in English from 2010 onwards. The database search was conducted by the second author on May 11 2022.
Based on advice from a University of Newcastle librarian, the CINAHL, Medline, and PsycInfo databases were searched using the term “communication” and, separately, the term “Rett syndrome.” These search terms were entered into the Anywhere field. These two sets of terms were first searched separately and then combined with the limiting parameters applied. For the ERIC and LLBA databases, we conducted a single advanced search using the combined terms “communication” and “Rett syndrome.” These terms were also entered into the Anywhere field and the same limiting parameters used in the other databases were applied.
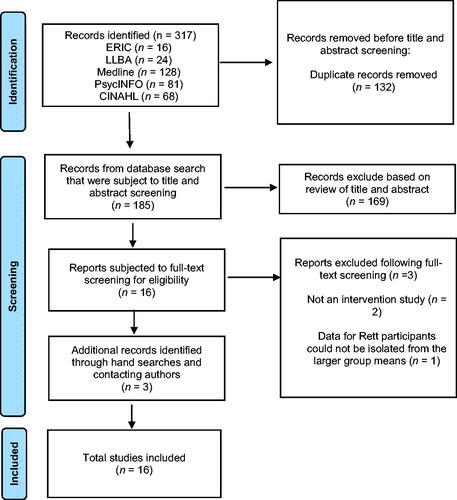
A total of 317 records were returned from the initial database search. Following the removal of duplicates (n = 132), the titles and abstracts of 185 records from the database search were independently screened by the first and second author. The purpose of this screening was to remove nonintervention studies, such as commentaries, review articles, and assessment-only studies. There was 98% agreement (four disagreements) on this initial screening. To resolve these four disagreements, the second author summarized each of these four studies and explained her rationale for including or excluding each of the four studies. The first author then responded by either agreeing with the second author or providing a rationale for any differing opinion. Through this process, the first and second author reached a consensus on the four initial disagreements. This resulted in 16 records being retained for full-text screening. Full-text screening was completed independently by the first and second authors. There was one disagreement (94% agreement) at this step. After reaching consensus on this disagreement, there was agreement between the first and second author that 13 studies met the inclusion criteria.
Subsequent hand searches were conducted of the reference lists for the 13 included studies. This occurred in June 2022. We also sent an e-mail to the lead or corresponding authors of the 13 already included studies. The e-mail informed them of our review and of their study or studies that had already been identified for inclusion. We asked if they had any additional papers on communication intervention for people with Rett syndrome for possible inclusion. These emails were sent on June 3rd and 4th, 2022 and 10 working days were allowed for responses. These subsequent search processes resulted in three additional studies being included; thus, a total of 16 studies were included in this review. provides a flowchart of the search and screening process.
Figure 1. Flowchart of process used to identify and screen studies for inclusion.
Data extraction
The 16 included studies were summarized in terms of (a) participants, (b) dependent variables related to communication, (c) intervention characteristics, and (d) main intervention outcomes. The first author extracted this information from each study and wrote a narrative summary of each study. The second author independently reviewed these summaries and any discrepancies were resolved by referring back to the original articles. We also contacted three author groups via email to clarify (a) procedural integrity checks (Byiers et al., Citation2014; Wandin et al., Citation2021) and (b) the version of the Vineland assessment that was used (Chou et al., Citation2019).
Certainty of evidence
The certainty of evidence for each study was rated as either conclusive, suggestive, or inconclusive based on the design and adequacy of reliability and procedural integrity checks to allow comparison with the previous Sigafoos et al. (Citation2009) review. Studies that used an experimental design (e.g., ABAB, multiple-baseline, control-group design) were rated as having the potential to provide conclusive evidence. Studies that did not use an experimental design (e.g., narrative case studies, pre-post testing without a control group, and A–B designs) were rated as providing inconclusive evidence. Studies with experimental designs also had to have adequate reliability (e.g., inter-observer or inter-rater agreement) and procedural integrity data (i.e., at least 20% of the sessions and 80% or better agreement/fidelity). If a study used an experimental design, but was found lacking with respect to reliability and/or procedural integrity, the certainty of evidence was considered suggestive.
Results
provides a summary of each included study’s (a) participants, (b) dependent variables related to communication, (c) intervention characteristics, (d) main intervention outcomes, and (e) certainty of evidence. The sections that follow provide collective summaries of the characteristics for this cohort of 16 studies.
Table 1. Summary of included studies.
Participants
Across the 16 included studies, 100 participants with Rett syndrome received intervention. Another 12 participants with Rett syndrome served as a control group (Study 4). The sample size of individual studies ranged from 1 to 31 (M = 7 participants per study). Four studies included only one participant (Studies 1, 5, 9, and 12). Nine studies included two to four participants (Studies 2, 3, 6, 10, 11, 13–16). The three remaining studies (Studies 4, 7, 8) were comparatively large, with sample sizes of 23, 31, and 28 participants, respectively.
All 112 individuals were female ranging from 3 to 47 years of age. Precise ages for individual participants were available for 30 participants because the three studies with the largest sample sizes (Studies 4, 7, 8) provided only age ranges and means. The overall grand mean age can be estimated at 14.5 years. Eight studies included at least one adult, 18 years of age or over (Studies 3–8, 11, 16). Seven studies included at least one preschool-aged child, 5 years or younger (Studies 2, 4, 8–10, 12, 14). Ten studies included at least one school-aged child/adolescent from 6 to 17 years of age (Studies 1–4, 7, 8, 10, 11, 13, 15).
Confirmed MECP2 mutations were reported for 92 participants included in Studies 4–9, 14 and 16 and for one of the two participants in Study 11; thus, 83% of the 112 total participants had a confirmed MECP2 mutation. Type of Rett syndrome (classic or atypical) was reported in two studies (Studies 2 and 11) representing six participants. Five had the classic type and one had an atypical variant. Participants’ stage of Rett syndrome was reported in seven of the 16 studies (44%). These seven studies (Studies 2, 5–8, 14, 15) included 73 participants, representing 65% of the total participant pool of 112. All but two of these 73 participants were in Stage III or IV. The other two participants, from Study 14, transitioned from Stage II to III during the intervention.
The presence or absence of functional speech (e.g., using spoken words to communicate) was reported in 12 studies covering 85 participants (Studies 2, 3, 5–8, 11–16). Only 1 of these 85 participants had functional speech (i.e., the participant used two words to make requests). For the remaining 27 participants across four studies (Studies 1, 4, 9, 10), information on their entry level spoken language abilities was not provided.
Dependent variables related to communication
Five different types of communication behavior served as dependent variables across the studies. Five studies (Studies 3, 11–13, 15) recorded the frequency with which participants selected graphic symbols or activated microswitches/speech-generating devices to request preferred items or events, such as requesting orange juice or asking to watch television. In Study 15, participants could also have other individualized goals that served as dependent variables, such as selecting messages from an AAC device to ask questions. In five other studies (Studies 1, 5–8), performance on various match-to-sample tasks was the communication behavior of interest. For example, selecting the correct choice picture or printed word from a two-choice array when presented with the corresponding spoken-word sample. Three studies (Studies 2, 9–10) recorded general conversational/turn-taking responses, such as initiating a communication interaction and responding to the communication initiations of a non-disabled adult communication partner. For two studies (Studies 4 and 14), standardized assessment scores served as dependent variables. Both of these studies reported scores from the Receptive, Expressive, and Written sub-domains of the Vineland Adaptive Behavior Scales (Sparrow et al., Citation1984, Citation2005). Study 14 also used the Assessment of Basic Language and Learning Skills-Revised (ABLLS-R; Partington, Citation2008) as a dependent measure. Finally, Study 16 recorded the rate at which participants selected core words (e.g., “MORE,” “FINISHED,” and “GOOD”) using a gaze-controlled communication device. Once a word had been selected, the device produced corresponding synthesized speech output.
Intervention characteristics
Seven different types of intervention approaches were implemented across the studies. These were (a) systematic instruction based on principles of applied behavior analysis (ABA), (b) staff/parent training, (c) music therapy, (d) implementation of specific curriculum, (e) aided language modeling, (f) transcranial direct current stimulation, and (g) a naturalistic interaction approach.
Eight studies (Studies 3, 6–8, 11–14) involved the use of various ABA-based systematic instructional tactics, such as most-to-least prompting, modeling, and reinforcement. Some of these studies employed named interventions, specifically: Functional Communication Training (Carr & Durand, Citation1985; Studies 3, 12), Early Intensive Behavioral Intervention (Reichow et al., Citation2014; Study 14), and a variation of the Picture Exchange Communication System (Bondy & Frost, Citation2001; Study 13). Three of these studies employed approaches referred to as Cognitive Empowerment Training (Studies 6, 7) and Cognitive Rehabilitation (Study 8), but the actual teaching procedures (e.g., verbal prompting, modeling, imitation, and generalization training) were based on operant conditioning/ABA principles.
The next most frequently used approach (used in three studies) involved training or coaching adult staff or parents. Study 2, for example, taught adults to use four strategies (i.e., create opportunities, present AAC devices, wait for child initiation, and respond to prelinguistic acts). Adults were taught to use these strategies to increase the child’s communicative initiations and responses. Study 12, already referenced above as an example of an ABA-based intervention, taught parents to use Functional Communication Training. Study 15, coached parents to use four strategies (a) presume competence, (b) follow the child’s lead, (c) acknowledge child responses, and (d) assign meaning to the child’s communicative attempts. These strategies were aimed at enabling participants to activate speech-generating devices via eye-tracking technology.
Two studies used music therapy (Studies 4, 9) and two studies implemented a specific curriculum; specifically the Accessible Literacy Learning (ALL) curriculum (Light & McNaughton, Citation2009) (Study 1), and Feuerstein et al. (Citation1988) mediated learning approach (Study 5). These curriculum-based programs appear to have also incorporated various systematic instructional procedures (e.g., time delay, modeling, shaping, and fading) to teach specifically sequenced skills. Another two studies (Studies 6 and 7) used transcranial direct current stimulation. Study 16 used an aided language modeling intervention (Sennott et al., Citation2016). With this approach, the communication partner pointed to symbols on the participant’s AAC device to model the use of the symbols for communication purposes. Finally, the intervention used in Study 10 was described as a type of naturalistic communication interaction. Interactions were conducted with and without eye-gaze technology to determine if that technology would facilitate the participant’s use of a computer-based communication device.
Intervention intensity was defined as the total number of minutes or hours of intervention received by participants, which provides a rough estimate of one common measure of treatment intensity (Warren et al., Citation2007). Calculations were derived from multiplying the number of individual intervention sessions by session duration and/or the overall length of the intervention phase. The most intense interventions were used in Studies 5 and 14. The 21-year-old participant in Study 5, for example, received 4, 50-min sessions per week over a 10-year period resulting in approximately 1733 h of intervention. The twins participating in Study 14 each received from 30 to 35 h of intervention per week for 3 years for a total of 4680–5460 h of intervention. The next most intense intervention was delivered to the 23 participants in Study 4, each of whom received 96 h of music therapy. In Study 13 participants received from approximately 26–53 h of intervention, which was aimed at teaching requesting skills using picture exchange and speech-generating devices. In half of the studies (Studies 1, 3, 6–9, 11–12, 16) the amount of intervention per participant ranged from about 1 to 10 h. Intervention intensity could not be determined for three studies (Studies 2, 10, 15).
In terms of communication modalities, half of the included studies used one or more forms of aided AAC (Studies 2, 3, 10–13, 15, 16). Aided AAC forms included (a) pointing to photographs or picture symbols (e.g., Studies 2 and 13), (b) touching a microswitch that then activated speech output (e.g., Studies 2 and 3), and (c) selecting symbols on a computer-based speech-generating device either directly or via eye-gaze technology (Studies 10, 11, 13, 15, 16). Seven studies targeted receptive and/or expressive speech modes (Studies 1, 4–8, 14), whereas Study 9 focused primarily on increasing prelinguistic behavior (e.g., body movements, eye gaze, and vocalizations) for some of the participants.
Intervention outcomes
Thirteen studies (Studies 1–3, 5, 6, 9–16) reported positive intervention outcomes. Positive outcomes included, for example: (a) increases in the percentage of correct responses (Studies 1, 11), (b) increases in the number of words, syllables, or letters learned (Studies 5, 6), (c) increased use of AAC devices to make requests (Studies 3, 12, 13), (d) increased frequency of communication initiations and responses to initiations (Studies 2, 9, 10), (e) increased Vineland scores in the communication domain (Study 14), and (f) attainment of individually set communication goals (Study 15). Two studies reported mixed outcomes (Studies 4 and 7). Specifically, in Study 4, music therapy was associated with significant increases in Vineland scores, but only for the receptive communication sub-domain. In Study 7, there was an increase in the production of vowels and phonemes for participants in the non-sham transcranial direct current stimulation condition, but no significant differences in the sham versus non-sham conditions on the number of words produced. Only one study (Study 8) reported a lack of any intervention effect for communication-related variables. In that study, intervention did not increase the production of correct identification of vowels, phonemes, or words.
Certainty of evidence
The certainty of evidence was rated as conclusive for four studies (Studies 1, 3, 11, 12). All four of these studies employed experimental designs and included adequate reliability (e.g., inter-observer or inter-rater agreement) and procedural integrity data. The evidence from another four studies was rated as suggestive (Studies 7, 8, 13, 16). These four studies employed experimental designs but lacked formal reliability and/or procedural integrity checks. The remaining eight studies (Studies 2, 4–6, 9, 10, 14, 15) were rated as providing inconclusive evidence because of pre-experimental designs and lack of formal reliability and/or procedural integrity checks.
Discussion
A previous review (Sigafoos et al., Citation2009) identified nine studies, published over a 10-year period (1995–2005), on enhancing communication functioning of people with Rett syndrome. The present updated review—covering the 12 year-period from 2010 to May 2022—identified 16 new studies. These 16 new studies extend the literature in relation to participant and intervention characteristics and the overall certainty of available evidence. Given the intervention challenges associated with Rett syndrome, these extensions to the literature could be seen as representing important advances.
The participant pool in this updated review is larger, more age-diverse, and generally better described than for the 2009 review. In terms of the total number of participants, the 2009 review covered 31 participants, whereas the present updated review covers 112 participants, 100 of whom received intervention; thus, the average sample size of studies increased from just over three participants per study in the 2009 review to a mean of seven participants per study in this updated review.
In addition to increased numbers of participants receiving intervention, the present set of 16 studies also covered a wider age range. Specifically, participant ages in the 2009 review ranged from 2:7 to 17:0 (years:months), whereas the participants covered by the current updated review ranged from 3 to 47 years of age. Eight studies in the present review included at least one adult participant, aged 18 years or older. The inclusion of adult participants is a significant extension given the relative lack of research into their learning and behavioral characteristics (Matson et al., Citation2008). Encouragingly, all but one of the eight studies that included adult participants (i.e., all but Study 8) reported positive outcomes. These generally positive outcomes support the potential value of providing communication intervention to the adult population, which is significant in light of recent evidence showing increased medical problems and deterioration of mood in people with Rett syndrome as they age (Cianfaglione et al., Citation2016). Such age-related problems might be expected to complicate the challenges already inherent in providing effective communication intervention to people with Rett syndrome. While it is encouraging that seven studies showed some positive intervention outcomes for adults with Rett syndrome, it is important to note that the oldest participant was 47 years old; thus, the extent to which even older adults might show a positive response to intervention will require additional research. It is also the case that none of the studies included in this review examined the potential impact of age-related health and mood problems. Exploring response to intervention in light of age-related changes would be a useful future research direction.
In the present review, most participants had a confirmed MECP2 mutation (83%). No such confirmation was provided in any of the nine studies included in the 2009 review, which is understandable given that the genetic basis of Rett syndrome was not discovered until 1999 (Amir et al., Citation1999). In addition, genetic testing in neurodevelopmental disorders has only recently become more routine (Du et al., Citation2022). The currently high confirmation rate increases diagnostic validity (Smith et al., Citation2003), which is critical for comparing response to intervention across and within different populations, such as comparing children with Rett syndrome to children with Angelman syndrome.
Similar to the results of the 2009 review, participants were mainly in Stage III or IV, and had the classic variant; however, the stage and type of Rett syndrome were not consistently reported. Also, none of the studies in either the present update or the 2009 review was designed to compare intervention outcomes for participants in different stages or variants. These could be important variables to isolate in future research. It is possible, for example, that individuals with the preserved speech variant of Rett syndrome (Skjeldal, Citation2020) might be more responsive to speech-mode interventions.
Only one study in the current updated review provided intervention to participants who were reported to be at Stage II of the disorder (Study 14). The twin girls in that study entered intervention at Stage II and progressed to Stage III over the course of a 3-year early intensive behavioral intervention program. Stage II is associated with rapid developmental regression of acquired motor, communication, and social skills (Fabio et al., Citation2020). In this second stage of Rett syndrome, children also tend to lose purposeful hand function. Stage II changes would likely have an impact on the child’s response to intervention, including any intervention aimed at enhancing communicative functioning. In contrast, while Stages III and IV are associated with severely restricted adaptive behavior functioning, these stages also seem to be associated with less rapid skill loss, which would seem to be more conducive to intervention. This could also be why most communication intervention research has involved participants in these later stages. However, it is also important to note that the developmental progression and characteristics associated with Rett syndrome may not necessarily follow or conform to a standard series of four distinct stages (Feldman et al., Citation2016). There appears to be little research on the impact of intervention on the developmental trajectory of individuals with Rett syndrome. An interesting line for future research would be to investigate whether it is possible to preserve more speech in persons with atypical Rett syndrome through early intensive speech therapy.
Implications for practice
The present updated review provides additional empirical support for the use of systematic instruction procedures. Several studies in both the present updated review (e.g., Byiers et al., Citation2014; Simacek et al., Citation2016; Stasolla et al., Citation2014) and the previous 2009 review (e.g., Sigafoos et al., Citation1996; Van Acker & Grant Citation1995) demonstrated successful acquisition of aided AAC for functional requesting via the application of various ABA-based systematic instructional tactics. This is not surprising given that such procedures are well established for teaching a range of adaptive behaviors to individuals with neurodevelopmental disorders (Storey, Citation2022). The effectiveness of these procedures for teaching communication skills to individuals with Rett syndrome may depend on the extent to which the targeted response mode (e.g., touching a switch or selecting graphic symbols) is compatible with participants’ motor abilities. Acquisition might also depend on the extent to which participants are motivated to communicate (Drasgow et al., Citation1999). There is some consensus in the AAC field that teaching participants to request highly preferred stimuli is one way to help ensure or increase motivation and might thus represent a useful initial communication function to target when beginning an AAC intervention (Still et al., Citation2014).
Three studies employed intervention approaches that appear to be widely applied in practice, specifically music therapy and aided language modeling. Music therapy was used in two studies (Studies 4 and 9) with modestly positive results reported for the dependent variables related to communication; however, the specific music therapy procedures that were applied differed across these two studies as described in . To date, there are not enough data on any one approach to the provision of music therapy for enhancing communication in Rett syndrome. In terms of future evaluations, it is generally the case that music therapy tends to have a more comprehensive focus. Consequently, it could have varying effects on different areas of functioning (e.g., social interaction versus communicating a request). In light of this, a systematic review of the wider music therapy literature involving individuals with Rett syndrome would seem timely. The one study (Study 16) using aided language modeling reported positive outcomes in terms of increased production of synthesized speech output. While several studies have reported positive effects of this approach with other populations (Sennott et al., Citation2016), additional studies are needed to ascertain the extent to which such approaches might also be effective for improving the communication functioning among people with Rett syndrome more generally.
In addition to these more well-established intervention approaches, a few studies evaluated novel intervention approaches. One such novel approach involved the use of eye tracking technology. This technology appears promising and could provide a means by which participants with significant motor impairment could reliably access high-tech AAC devices. Another novel intervention involved the use of transcranial direct current stimulation. The two studies in which this was applied (Studies 6 and 7), reported some positive impact on the participants’ communication, but these participants also received systematic instruction. Still, additional research on the use of such stimulation would seem warranted.
Intervention intensity did not seem to be a critical variable. While studies with the most intensive interventions (Studies 5 and 14) reported positive results, other studies demonstrated clear evidence that the targeted communication skills had increased after relatively brief intervention (e.g., 1–10 h). Byiers et al. (Citation2014; Study 3), for example, taught three participants with Rett syndrome to use microswitches to request preferred stimuli, instead of resorting to problematic forms of prelinguistic requesting (i.e., self-injury, whining, or grabbing). All three participants learned this new requesting response within about 60 min of systematic instruction. Instead of total hours of training, targeting discrete communication forms and functions and applying systematic instruction seemed to be the more critical variables; however, this conclusion is tentative because none of these studies set out to investigate the effects of varying treatment intensity. In addition, parameters other than total hours of intervention provided should be considered when evaluating intervention intensity, such as comparing intervention outcomes when intervention sessions vary in terms of the number of teaching opportunities provided and responses made (Warren et al., Citation2007). Reichle et al. (Citation2021) noted “Treatment intensity is an aspect of communication intervention that has received limited empirical attention” (p. 146). Future research on a range of parameters related to treatment intensity could make for more efficient delivery of communication intervention.
Limitations and future directions
Only one of the nine studies in the previous 2009 review (Sigafoos et al., Citation2009) was judged to provide conclusive evidence. In contrast, eight studies in this updated review (50%) were rated as providing conclusive or suggestive evidence. This change is due to a higher percentage of studies using experimental designs to evaluate intervention effects. In that respect, the methodological quality of the communication intervention literature for people with Rett syndrome could be said to have improved over the past 12 years. This conclusion should be interpreted with caution, however, because in the present review was limited in its approach to the ascertainment of certainty of evidence. Specifically, we only considered whether the study had an experimental design and adequate reliability and procedural integrity data. Other factors, such as replicable procedures and operationally defined dependent variables, are also relevant when judging the certainty of evidence; however, these latter aspects would seem to involve more subjectivity of judgment. Still, this review has identified new studies that collectively add much needed quantity and quality to the intervention literature in enhancing communicative functioning in persons with Rett syndrome.
In terms of future directions, subsequent reviews could aim to include grey literature and other steps to mitigate against publication bias. As mentioned before, future reviews would also be improved by considering a wider range of variables that influence a study’s certainly of evidence. Consideration of a wider range of parameters related to treatment intensity (e.g., number instructional opportunities) would also likely strengthen the quality of future reviews.
Conclusion
This updated review identified 16 studies that collectively would seem to extend the generality or external validity of the literature on communication intervention for people with Rett syndrome. Establishing the generality of intervention research depends in part on participant numbers and their characteristics (Murad et al., Citation2018). The present set of 16 studies included a relatively large and more age-diverse participant pool and thus extends the overall generality of the literature on enhancing communication functioning of children, adolescents, and adults with Rett syndrome. This updated review also provides additional experimental demonstrations that systematic instructional procedures can be successfully applied to teach functional use of aided AAC to individuals with Rett syndrome. This review also identified a number of novel intervention approaches that would seem worthy of additional research. Eye tracking technology for enabling participants to activate speech-generating devices is one such innovation that would seem to have considerable potential given the motoric impairments associated with Rett syndrome.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References *Indicates articles included in this review
- *Ainsworth, M. K., Evmenova, A. S., Behrmann, M., & Jerome, M. (2016). Teaching phonics to groups of middle school students with autism, intellectual disabilities, and complex communication needs. Research in Developmental Disabilities, 56, 165–176. doi:10.1016/j.ridd.2016.06.001
- Amir, R. E., Van den Veyver, I. B., Wan, M., Tran, C. Q., Francke, U., & Zoghbi, H. Y. (1999). Rett syndrome is caused by mutations in X-linked MECP2, encoding methyl-CpG-binding protein 2. Nature Genetics, 23(2), 185–188. doi:10.1038/13810
- *Bartolotta, T. E., & Remshifski, P. A. (2013). Coaching communication partners: A preliminary investigation of communication intervention during mealtime in Rett syndrome. Communication Disorders Quarterly, 34(3), 162–171. doi:10.1177/1525-740112453165
- Bartolotta, T. E., Zipp, G. P., Simpkins, S. D., & Glazewski, B. (2011). Communication skills in girls with Rett syndrome. Focus on Autism and Other Developmental Disabilities, 26(1), 15–24. doi:10.1177/1088357610380042
- Bondy, A., & Frost, L. (2001). The picture exchange communication system. Behavior Modification, 25(5), 725–744. doi:10.1177/0145445501255004
- Bruscia, K. E. (1987). Free improvisation model (Alvin Model). In K. E. Bruscia (Ed.), Improvisation models of music therapy (pp. 75–111). Charles C. Thomas.
- *Byiers, B. J., Dimian, A., & Symons, F. J. (2014). Functional communication training in Rett syndrome: A preliminary study. American Journal on Intellectual and Developmental Disabilities, 119(4), 340–350. doi:10.1352/1944-7558-119.4.340
- Carr, E. G., & Durand, V. M. (1985). Reducing behavior problems through functional communication training. Journal of Applied Behavior Analysis, 18(2), 111–126. doi:10.1901/jaba.1985.18-111
- *Chou, M.-Y., Chang, N.-W., Chen, C., Lee, W.-T., Hsin, Y.-J., Siu, K.-K., Chen, C.-J., Wang, L.-J., & Hung, P.-L. (2019). The effectiveness of music therapy for individuals with Rett syndrome and their families. Journal of the Formosan Medical Association = Taiwan yi zhi, 118(12), 1633–1643. doi:10.1016/j.jfma.2019.01.001
- Cianfaglione, R., Clarke, A., Kerr, M., Hastings, R. P., Oliver, C., & Felce, D. (2016). Ageing in Rett syndrome. Journal of Intellectual Disability Research, 60(2), 182–190. doi:10.1111/jir.12238
- Drasgow, E., Halle, J. W., & Sigafoos, J. (1999). Teaching communication to learners with severe disabilities: Motivation, response competition, and generalization. Australasian Journal of Special Education, 23(1), 47–63. doi:10.1017/S1030011200024507
- Du, X., Glass, J. E., Balow, S., Dyer, L. M., Rathbun, P. A., Guan, Q., Liu, J., Wu, Y., Dawson, D. B., Walters-Sen, L., Smolarek, T. A., & Zhang, W. (2022). Genetic testing in patients with neurodevelopmental disorders: Experiences of 511 patients at Cincinnati Children’s Hospital Medical Center. Journal of Autism and Developmental Disorders, 52(11), 4828–4842. doi:10.1007/s10803-021-05337-6
- Einspieler, C., & Marschik, P. B. (2019). Regression in Rett syndrome: Developmental pathways to its onset. Neuroscience and Biobehavioral Reviews, 98, 320–332. doi:10.1016/j.neubiorev.2019.01.028
- Eldevik, S., Jahr, E., Eikeseth, S., Hastings, R. P., & Hughes, C. J. (2010). Cognitive and adaptive behavior outcomes of behavioral intervention for young children with intellectual disability. Behavior Modification, 34(1), 16–34. doi:10.1177/0145443509351961
- Fabio, R. A., Capri, T., & Martino, G. (2020). Understanding Rett syndrome: A guide to symptoms, management and treatment. Routledge.
- *Fabio, R. A., Castelli, I., Marchetti, A., & Antonietti, A. (2013). Training communication abilities in Rett syndrome through reading and writing. Frontiers in Psychology, 4, 911. doi:10.3389/f.psyg.2013.00911
- *Fabio, R. A., Gangemi, A., Capri, T., Budden, S., & Falzone, A. (2018). Neurophysiological and cognitive effects of transcranial direct current stimulation in three girls with Rett syndrome and chronic language impairments. Research in Developmental Disabilities, 76, 76–87. doi:10.1016/j.ridd.2018.03.008
- *Fabio, R. A., Giannatiempo, S., Semino, M., & Caprì, T. (2021). Longitudinal cognitive rehabilitation applied with eye-tracker for patients with Rett syndrome. Research in Developmental Disabilities, 111, 103891. doi:10.1016/j.ridd.2021.103891
- *Fabio, R., Gangemi, A., Semino, M., Vignoli, A., Priori, A., Canevini, M., Di Rosa, G., & Caprì, T. (2020). Effects of combined transcranial direct current stimulation with cognitive training in girls with Rett syndrome. Brain Sciences, 10(5), 276. doi:10.3390/brainsci10050276
- Fehr, S., Bebbington, A., Nassar, N., Downs, J., Ronen, G., De Klerk, M., & Leonard, H. (2011). Trends in the diagnosis of Rett syndrome in Australia. Pediatric Research, 70(3), 313–319. doi:10.1203/PDR.0b013e3182242461
- Feldman, D., Banerjee, A., & Sur, M. (2016). Developmental dynamics of Rett syndrome. Neural Plasticity, 2016, 6154080. doi:10.1155/2016/6154080
- Ferreira, M. G., & Teive, H. A. G. (2020). Hand stereotypies in Rett syndrome. Pediatric Neurology Briefs, 34(0), 2. doi:10.15844/pedneurbriefs-34-2
- Feuerstein, R., Rand, Y., & Rynders, J. (1988). Don’t accept me as I am: Helping retarded people to excel. University Park Press. 10.1007/978-1-4899-6128-0
- Foxe, J. J., Burke, K. M., Andrade, G. N., Djukic, A., Frey, H.-P., & Molholm, S. (2016). Automatic cortical representation of auditory pitch changes in Rett syndrome. Journal of Neurodevelopmental Disorders, 8(1), 34. doi:10.1186/s11689-016-9166-5
- *Hackett, S., Morison, C.-J., & Pullen, C. (2013). A retrospective practice-based evaluation of music therapy: A single-case study of a four-year-old girl with Rett syndrome—Rebecca’s story. The Arts in Psychotherapy, 40(5), 473–477. doi:10.1016/j.aip.2013.09.005
- Hagberg, B. (2002). Clinical manifestations and stages of Rett syndrome. Mental Retardation and Developmental Disabilities Research Reviews, 8(2), 61–65. doi:10.1002/mrdd.10020
- *Hsieh, Y.-H., Borgestig, M., Gopalarao, D., McGowan, J., Granlund, M., Hwang, A.-W., & Hemmingsson, H. (2021). Communicative interaction with and without eye-gaze technology between children and youths with complex needs and their communication partners. International Journal of Environmental Research and Public Health, 18(10), 5134. doi:10.3390/ijerph18105134
- Julien, H. M., Parker-McGowan, Q., Byiers, B. J., & Reichle, J. (2015). Adult interpretation of communicative behavior in learners with Rett syndrome. Journal of Developmental and Physical Disabilities, 27(2), 167–182. doi:10.1007/s10882-014-9407-z
- Kiresuk, T., Smith, A., & Cardillo, J. (1994). Goal Attainment Scaling: Applications, theory, and measurement. Lawrence Erlbaum.
- Larriba-Quest, K., Byiers, B. J., Beisang, A., Merbler, A. M., & Symons, F. J. (2020). Special education supports and services for Rett syndrome: Parent perceptions and satisfaction. Intellectual and Developmental Disabilities, 58(1), 49–64. doi:10.1352/1934-9556-581.49
- Light, J., & McNaughton, D. (2009). ALL curriculum guide. Mayer-Johnson.
- Light, J., & McNaughton, D. (2011). Supporting the communication, language, and literacy development of children with complex communication needs: State of the science and future research priorities. Assistive Technology : The Official Journal of RESNA, 24(1), 34–44. doi:10.1080/10400435.2011.648717
- Marschik, P. B., Vollmann, R., Bartl-Pokorny, K. D., Green, V. A., van der Meer, L., Wolin, T., & Einspieler, C. (2014). Developmental profile of speech-language and communication functions in an individual with the preserved speech variant of Rett syndrome. Developmental Neurorehabilitation, 17(4), 284–290. doi:10.3109/17518423.2013.783139
- Matson, J. L., Dempsey, T., & Wilkins, J. (2008). Rett syndrome in adults with severe intellectual disability: Exploration of behavioral characteristics. European Psychiatry : The Journal of the Association of European Psychiatrists, 23(6), 460–465. doi:10.1016/j.eurpsy.2007.11.008
- Murad, M. H., Katabi, A., Benkhadra, R., & Montori, V. M. (2018). External validity, generalisability, applicability and directedness: A brief primer. BMJ Evidence-Based Medicine, 23(1), 17–19. doi:10.1136/ebmed-2017-110800
- Neul, J. L., Kaufmann, W. E., Glaze, D. G., Christodoulou, J., Clarke, A. J., Bahi-Buisson, N., Leonard, H., Bailey, M. E. S., Schanen, N. C., Zappella, M., Renieri, A., Huppke, P., & Percy, A. K. (2010). Rett syndrome: Revised diagnostic criteria and nomenclature. Annals of Neurology, 68(6), 944–950. doi:10.1002/ana.22124
- Neul, J. L., Lane, J. B., Lee, H.-S., Geerts, S., Barrish, J. O., Annese, F., Baggett, L. M., Barnes, K., Skinner, S. A., Motil, K. J., Glaze, D. G., Kaufmann, W. E., & Percy, A. K. (2014). Developmental delay in Rett syndrome: Data from the natural history study. Journal of Neurodevelopmental Disorders, 6(1), 20. doi:10.1186/1866-1955-6-20
- Operto, F. F., Mazza, R., Giovanna Pastorino, G. M., Verrotti, A., & Coppola, G. (2019). Epilepsy and genetics in Rett syndrome: A review. Brain and Behavior, 9(5), e01250. doi:10.1002/brb3.1250
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ (Clinical Research ed.), 372, n71. doi:10.1136/bmj.n71
- Partington, J. (2008). The assessment of basic language and learning skills-revised (ABLLS-R): An assessment curriculum guide and skills tracking system for children with autism and other developmental disabilities. Behavior Analysts Inc.
- Percy, A. K., & Glaze, D. G. (2017). The natural history of Rett syndrome: Building on recent experience. In W. E. Kaufmann (Ed.), Rett syndrome (pp. 14–23). Mac Keith Press.
- Reichle, J., Ganz, J. B., Pierson, L., & Rodriguez, D. (2021). Treatment intensity: Considering persons with autism spectrum disorder and intellectual disability who have complex communication needs. Research and Practice for Persons with Severe Disabilities, 46(3), 146–158. doi:10.1177/15407969211036202
- Reichow, B., Barton, E., Boyd, B., & Hume, K. (2014). Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD). Campbell Systematic Reviews, 10(1), 1–116. https://www.campbellcollaboration.org/library/early-intensive-behavioral-intervention-children-autism.html doi:10.4073/csr.2014.9
- Reichow, B., George-Puskar, A., Lutz, T., Smith, I. C., & Volkmar, F. R. (2015). Brief report: Systematic review of Rett syndrome in males. Journal of Autism and Developmental Disorders, 45(10), 3377–3383. doi:10.1007/s10803-015-2519-1
- Sandweiss, A. J., Brandt, V. L., & Zoghbi, H. Y. (2020). Advances in understanding Rett syndrome and MECP2 duplication syndrome: Prospects for future therapies. The Lancet. Neurology, 19(8), 689–698. doi:10.1016/S1474-4422(20)30217-9
- Sennott, S., Light, J. C., & McNaughton, D. (2016). AAC modeling intervention research review. Research and Practice for Persons with Severe Disabilities, 41(2), 101–115. doi:10.1177/1540796916638822
- Sigafoos, J., Green, V. A., Schlosser, R., O’eilly, M. F., Lancioni, G. E., Rispoli, M., & Lang, R. (2009). Communication intervention in Rett syndrome: A systematic review. Research in Autism Spectrum Disorders, 3(2), 304–318. doi:10.1016/j.rasd.2008.09.006
- Sigafoos, J., Laurie, S., & Pennell, D. (1996). Teaching children with Rett syndrome to request preferred objects using aided communication: Two preliminary studies. Augmentative and Alternative Communication, 12(2), 88–96. doi:10.1080/07434619612331277538
- *Simacek, J., Dimian, A. F., & McComas, J. J. (2017). Communication intervention for young children with severe neurodevelopmental disabilities via telehealth. Journal of Autism and Developmental Disorders, 47(3), 744–767. doi:10.1007/s10803-016-3006-z
- *Simacek, J., Reichle, J., & McComas, J. J. (2016). Communication intervention to teach requesting through aided AAC to two learners with Rett syndrome. Journal of Developmental and Physical Disabilities, 28(1), 59–81. doi:10.1007/s10882-015-9423-7
- Skjeldal, O. H. (2020). Rett syndrome. In A. El-Baz & J. S. Suri (Eds.), Neurological disorders and imaging physics (vol. 5, pp. 6.1–6.10). IOP Science. doi:10.1088/978-0-7503-2723-7ch6
- Smeets, E. E. J., Pelc, K., & Dan, B. (2012). Rett syndrome. Molecular Syndromology, 2(3-5), 113–127. doi:10.1159/000337637
- Smith, G. G., Cerham, J. H., & Invik, R. J. (2003). Diagnostic validity. In D. S. Tulsky, D. H. Saklofske, G. J. Chelune, R. K. Heaton, R. J. Invik, R. Bornstein, A. Prifitera, & M. F. Ledbetter (Eds.), Clinical interpretation of the WAIS-III and WMS-III (pp. 273–301). Academic Press. doi:10.1016/B978-012703570-3/50012-2
- Smith, T., Klevstrand, M., & Lovaas, O. I. (1995). Behavioral treatment of Rett’s disorder: Ineffectiveness in three cases. American Journal on Mental Retardation, 100(3), 317–322.
- Sparrow, S. S., Balla, D. A., & Cicchetti, D. V. (1984). Vineland adaptive behavior scales. American Guidance Service.
- Sparrow, S. S., Balla, D. A., & Cicchetti, D. V. (2005). Vineland adaptive behavior scales (Vineland™-II) (2nd ed.). Pearson.
- Still, K., Rehfeldt, R. A., Whelan, R., May, R., & Dymond, S. (2014). Facilitating requesting skills using high-tech augmentative and alternative communication devices with individuals with autism spectrum disorders: A systematic review. Research in Autism Spectrum Disorders, 8(9), 1184–1199. doi:10.1016/j.rasd.2014.06.003
- Storey, K. (2022). Systematic instruction of functional skills for students and adults with disabilities (3rd ed.). Charles C. Thomas.
- *Stasolla, F., De Pace, C., Damiani, R., Di Leone, A., Albano, V., & Perilli, V. (2014). Comparing PECS and VOCA to promote communication opportunities and to reduce stereotyped behaviors by three girls with Rett syndrome. Research in Autism Spectrum Disorders, 8(10), 1269–1278. doi:10.1016/j.rasd.2014.06.009
- Tarquinio, D. C., & Percy, A. K. (2016). Rett syndrome: Clinical aspects. In C. Sala & C. Vernelli (Eds.), Neuronal and synaptic dysfunction in autism spectrum, disorder and intellectual disability (pp. 301–323). Academic Press. doi:10.1016/B978-0-12-800109-7.00019-4
- *Titlestad, K. B., & Eldevik, S. (2019). Brief report: Modest but clinically meaningful effects of early behavioral intervention in twins with Rett syndrome—A case study. Journal of Autism and Developmental Disorders, 49(12), 5063–5072. doi:10.1007/s10803-019-04185-9
- Van Acker, R., & Grant, S. H. (1995). An effective computer-based requesting system for persons with Rett syndrome. Journal of Childhool Communication Disorders, 16(2), 31–38. doi:10.1177/1525740195016000205
- *Vessoyan, K., Steckle, G., Easton, B., Nichols, M., Mok Siu, V., & McDougall, J. (2018). Using eye-tracking technology for communication in Rett syndrome: Perceptions of impact. Augmentative and Alternative Communication (Baltimore, Md. : 1985), 34(3), 230–241. doi:10.1080/07434618.2018.1462848
- *Wandin, H., Lindberg, P., & Sonnander, K. (2021). Aided language modeling, responsive communication and eye-gaze technology as communication intervention for adults with Rett syndrome: Three experimental single case studies. Disability and Rehabilitation: Assistive Technology, 1–15. doi:10.1080/17483107.2021.1967469
- Warren, S. F., Fey, M., & Yoder, P. (2007). Differential treatment intensity research: A missing link to creating optimally effective communication interventions. Mental Retardation and Developmental Disabilities Research Reviews, 13(1), 70–77. doi:10.1002/mrdd.20139