
Abstract
The selection of high-tech AAC for children diagnosed with autism spectrum disorder can be a challenging process due to the vast array of options available. One of the decisions that clinicians need to make involves how vocabulary will be organized on the display. This study aimed to compare a visual scene display (VSD) with a grid display using a multiple-probe design across participants with an embedded adapted alternating treatment design. Four young children with autism spectrum disorder who were beginning communicators were recruited and taught to request preferred items using two display formats: VSD and grid layout on a mainstream tablet with an AAC app. Two of the participants achieved criterion with both displays, the other two participants failed to achieve criterion in either display. For all participants, progress was similar in both displays. The results are discussed through the lens of each participant’s characteristics with suggestions for clinical decision-making.
One of the salient characteristics of autism is the presence of communication disorder which can vary widely from one child to another (Mirenda, Citation2008, Citation2009). Some children present with average speech and language skills but experience difficulties with social communication while others have significant difficulties in the area of language and communication (Simpson, Citation2019). Research has indicated that up to 30% of these children do not develop functional speech (Rose et al., Citation2016), For these children, the use of AAC systems and strategies is a necessity to support the development of communication skills. This is particularly important as research has indicated that the development of communication skills is linked to improved educational and employment outcomes (Iacono et al., Citation2016).
A range of AAC systems can be successfully implemented with children with autism, both unaided and aided (Gevarter et al., Citation2014). Over the last 10 years, high-tech AAC which can provide speech output has become increasingly accessible to children with autism due to the development of mainstream tablet technology (Carnett et al., Citation2021). Such technology has increased the hardware and software options which are available, for example, appearance, and system features (Light & McNaughton, Citation2012b). With the range of options available, the clinician is expected to make complicated decisions regarding which system or combination of AAC systems/strategies to introduce to individual children with autism. These children are often beginning communicators who are in the prelinguistic or early linguistic stages of language development using communicative behaviors which are typical of early language development such as gestures and facial expressions to express themselves (Holyfield et al., Citation2019). Making evidence-based decisions about AAC systems is important when research suggests that there is great variability in AAC outcomes for children who present with autism (Sievers et al., Citation2018).
Meta-analyses have begun to elucidate which types of AAC systems are likely to be the best match for individuals with particular characteristics of autism (Aydin & Diken, Citation2020; Carnett et al., Citation2021). These publications have concluded that a range of AAC systems may be effective, but factors such as individual preference and communication goals should be considered when recommending an AAC system for a particular individual. Furthermore, it is noted that the characteristics of the individual such as the existing level of motor imitation abilities and fine motor skills are likely to impact the efficiency of learning to use AAC (Aydin & Diken, Citation2020; Ganz et al., Citation2012). Individualized assessment is, therefore, necessary to identify child characteristics to select the AAC system to ensure the best fit (Light et al., Citation2019). These studies suggest that much research still needs to be done to support clinicians to distinguish which child characteristics could guide the selection and learning of a particular AAC system.
The identification of an AAC system is the beginning of ongoing decisions and personalization processes which could include the organizational layout of vocabulary items on the display of speech-generating devices (SGDs). Organizational layout is forefronted in decisions because it has been suggested that how vocabulary is organized could be a key factor in the success or failure of AAC interventions (Light et al., Citation2019). Typically, children with developmental delays, including autism, rely on systems that make use of two types of vocabulary organization; grid formats and visual scene displays (VSDs) (Light et al., Citation2019). Grid formats are a method of representing the vocabulary on AAC displays in which symbols are presented in a row-column grid format enabling the users to construct a message by indicating cells sequentially from within the grid configuration. Visual scene displays (VSDs), on the other hand, offer an alternative method of vocabulary organization (Light & McNaughton, Citation2012a, Citation2012b). A VSD is typically a photographic scene that represents a meaningful and motivating event from an individual’s life (Blackstone, 2004). In a VSD, parts of the image have target areas, called hotspots, that when accessed emit a spoken utterance relevant to the element of the visual scene, e.g., ’let’s play ball’ is spoken when the hotspot ‘ball’ is accessed on a playground scene. Each of these display formats differs in how the vocabulary is presented as well as the cognitive processing demands that would be experienced by the user (Wilkinson et al., Citation2012).
Light and McNaughton (Citation2012a, Citation2012b, 2018, 2019) state that VSDs are advantageous to beginning communicators as they present language concepts in familiar scenes that are meaningful to the learner thus supporting early pragmatic and semantic development. This is in contrast to grid displays which may impose some meta-linguistic demands because words and concepts are presented out of context (Drager et al., Citation2019). Thistle and Thiessen (Citation2021) note that the biggest difference between the two display formats is the contextual support that VSDs may offer due to their holistic nature. Specifically, it has been stated that the use of VSDs may be appropriate for young children with autism as well as children with autism who are beginning communicators as they could benefit from this contextual support (Drager et al., Citation2004). Furthermore, it has been proposed that VSDs could be advantageous as they reduce the working memory demands when compared to grid formats (Light & McNaughton, Citation2012a, Citation2012b).
Researchers debate whether VSDs would impact the generalization of knowledge and use of words, as the visual representation of a word in a VSD is lacking in form and scene-context which could impact its use in other contexts (von Tetzchner, Citation2015). Researchers have acknowledged that VSDs may be less effective at supporting the development of syntax and morphology potentially restricting the child’s ability to create novel and complex sentences (Abbot & McBride, Citation2014). In a recent study by Thistle and Thiessen (Citation2021), clinicians and researchers expressed the view that VSDs are unlikely to support spontaneous utterance generation due to the nature of the preprogrammed language in these displays. The authors concluded that further research is still required to determine how multiple communicative functions can be fulfilled using VSDs. Grids therefore are advantageous as they provide increased capacity to support generative language as well as providing support for a range of communicative functions (Light et al., Citation2019).
Despite Light et al. (Citation2019) recent publications of evidence-based guidelines for the design for each type of display, it is still unclear which method of organizing vocabulary on the SGD display should be chosen for individual children (Thistle & Thiessen, Citation2021). Although not specific to children with autism, Light et al. (Citation2018) suggest that VSDs might be the chosen method of vocabulary organization for children who are beginning communicators.
Although the literature on VSDs for autism is still emerging (Caron & Holyfield, Citation2019), some comparative studies such as those reported by Gevarter et al. (Citation2014, Citation2017, Citation2018) have focused on demonstrating the efficiency of vocabulary organized in VSDs in comparison to grid formats when teaching children with autism to request. In these studies, participants were taught to request single items using vocabulary formats which included a grid and VSD format. The results suggested that VSDs are more advantageous when teaching requesting to children with autism as learning was faster and more consistent with the VSD intervention.
In the Gevarter et al. studies a photo was used for the VSD while symbols or line drawings were used for the grid display. Gevarter et al. (Citation2017) note that it is likely that the use of photo images in the VSD played a role in the results as it appeared that the participants displayed greater difficulty learning less iconic symbols. While Romski and Sevcik (Citation2005) have suggested that such a difference should not influence the learning of the photo/symbol referent, Light et al. (Citation2019) note that photo material is easier to learn than line drawings in which case the results may have been predisposed toward the VSD.
Taken overall, the Gevarter et al. studies indicate that the VSD is a more efficient choice of display format, yet Gevarter et al. (Citation2018) have also noted that it is unlikely that one kind of display format is appropriate for all children with autism. Recently, Gevarter et al. (Citation2020) concluded that there appears to be minimal differences between the two displays for young children with autism. Furthermore, it has been suggested that future research that includes participants with different characteristics is needed to provide further information that can support clinicians in making decisions on how best to organize vocabulary for individual children (Caron & Holyfield, Citation2019; Gevarter et al., Citation2020; Thistle & Thiessen, Citation2021). The aims of the present research are therefore a) to compare the use of a grid format with a VSD format when teaching requesting to children diagnosed with autism who are beginning communicators and b) to extend on previous studies by ensuring that iconicity is the same for both VSDs and grid display formats.
Method
Participants
The participants were four young male children, aged between 4;09 (months; years) and 5;07, who attended mainstream schooling on a full-time basis. The four participants who met the following criteria were identified from the waiting list of an AAC assessment and intervention unit; (a) diagnosis of ASD from a psychologist independent of the study, (b) under the age of 6 years, (c) non-speaking or used less than 20 words for functional communication (Tager-Flusberg et al., Citation2009). The participants were offered a screening appointment in accordance with typical unit procedures with both a speech and language therapist (SLT; who was the first author) and an occupational therapist (OT) employed within the unit. During the screening appointment, further inclusion criteria were applied: (a) confirmation that the child verbalized less than 20 words using natural speech for functional communication through parental report and assessment of the child’s expressive communication, (b) no auditory/visual impairments that would impact on learning to use the AAC system.
All four families completed an informed consent process in which they were given an information sheet describing the study (approved by two university ethics boards). The parents of participants who met the inclusion criteria were given an information letter in Maltese and English inviting them to voluntarily participate in the study. The lead author answered any questions that the families had to ensure they understood their anticipated participation in the research project. The parents then signed a consent form for their children to participate in the study. The participant’s willingness to participate in sessions was taken as assent.
Before commencement of the study, assessments were administered to the participants to ensure adequate description of their individual characteristics (refer to ; all names are pseudonyms). Early communication skills were assessed by the first author using the Total Gestures section MacArthur Bates Communication Development Inventory: Words and Gestures (CDI) (Fenson et al., Citation2007). This caregiver-reported questionnaire of early language and social communication intended for typically developing children aged between 8 and 30 months has been utilized with older children with autism (Luyster et al., Citation2007). The Total Gestures section is organized into two kinds of gestures; those that involve social engagement and appear in the first 12 months, and those that appear at approximately 16 months and involve skills such as play and imitation.
Table 1. Summary of participant characteristics (all Names are Pseudonyms)
Social communication severity was assessed by the researcher and an OT using Module 1 of the Autism Diagnostic Observation Schedule-2 (ADOS-2) (Lord et al., Citation2012). This is designed to be administered to children who are non-speaking or use little speech and provides a measure of the level of autism spectrum-related symptoms.
The Vineland Adaptive Behavior Scales-II (VABS-II) (Sparrow et al., Citation2005), a structured caregiver interview, was administered by the first author to assess adaptive functioning. This instrument yields scores in four domains; communication, socialization, daily living, and motor scales as well as a Vineland Adaptive Behavior Score.
The Short Sensory Profile (SSP) (McIntosh et al., Citation1999) was administered by the OT. The SSP is a standardized parent questionnaire utilized to identify sensory processing difficulties in children aged 3-10 years. The profile generates a total SSP score. An SSP score between 155 and 190 points is considered typical.
Setting
The study took place in a clinic room measuring 5.7 × 6.3 m2 equipped with a child’s table and chair, and chairs for the adults. Objects the children liked (see Materials) were placed on a shelf out of reach but in sight close to the table. Two clinicians; SLT (first author) and OT and a caregiver were present for all sessions. One observer was present for all sessions to conduct interobserver agreement. Another was present for 30% of the sessions to carry out procedural fidelity checks.
Research design
This study used a multiple-probe design (MPD) across participants with embedded adapted alternating treatment design (AATD) which allowed for comparison of requesting behavior between two treatments: a VSD and a grid layout on a tablet. The MPD was chosen as an alternative to a multiple baseline design because it allows for intermittent data collection in the baseline phase based on the assumption that baseline behaviors are unlikely to change without intervention (Wolery, Citation2013). The AATD was chosen as it is useful when comparing interventions in which participants are taught nonreversible behaviors and its design specifically allows the comparison of efficiency of the VSD and the grid display (Wolery, Citation2013). The study consisted of four phases; baseline, intervention, post-intervention, and follow-up (Wolery et al., Citation2014).
Participants were taught to request using both display formats on a tablet. For this study, requesting, which was the dependent variable, was defined as the participant spontaneously picking up the tablet, reaching toward the communication partner with the tablet, and then touching a cell on the screen to activate the voice output in exchange for a motivator. The independent variable was the introduction of a prompting sequence, which was introduced to teach each participant to request with the tablet during the intervention phase for both VSD and grid layout conditions.
All participants commenced the baseline phase on the same day. Baseline probes were carried out once a week until the week prior to the commencement of intervention during which each participant then attended for three consecutive baseline sessions. This ensured that a stable baseline was established before the introduction of the intervention. The intervention was introduced to each participant sequentially, one week apart so the fourth participant remained in baseline for the longest period. The study was planned in this way to avoid long periods in baseline in the event that a participant did not make progress with the intervention (Gast et al., Citation2014). During the intervention phase, participants were taught to request two different sets of motivators using a tablet for each of the two visual displays: a VSD and a grid format. Each participant received 12 sessions of intervention: six in each condition. In the post-intervention, each participant received 3 further sessions similar to the baseline. Maintenance was assessed in the follow-up phase 4 weeks after the last post-intervention session.
Researchers
The first author is a SLT and provided the intervention described in this study. An OT, trained by the first author who was employed on the same assessment team, supported the data collection.
Materials
Motivators
Food and toys that the children liked were identified for each participant using a two-stage assessment process prior to study commencement (Kang et al., Citation2013). Stage 1 of the motivator assessment was an indirect assessment carried out through a 30-minute caregiver interview adapted from Green et al. (Citation2008) designed to identify snacks and toys that the participant enjoys, and which were suitable for intervention in a clinic setting. In stage 2, the motivators identified in stage 1 were presented to the participants on three separate occasions over 1-2 weeks. All identified motivators were presented in 2 groups: snacks and toys. Snacks and toys were ranked separately using the formula (number of selections/number of offers)x100% (). Two equitable sets of four motivators were created and each set was randomly allocated to each of the two treatment conditions to ensure that change in requesting behavior was not influenced by how motivating the items were (Wolery et al., Citation2014).
Table 2. Reinforcer assessment results
Speech-output technology
The speech-output technology used for all phases of the study was a mainstream tablet; an iPad 4Footnote1 encased in a Big GripsFootnote2 cover with iOS 9.2.0 with Scene and Heard appFootnote3 version 3.0. This app was chosen as it could be used for both display conditions; the VSD and grid conditions (refer to for examples). The app had the capacity to import photographs and make recordings according to the motivators identified for each participant in the pre-baseline phase. For the VSD condition, a photograph of the motivators on a shelf as they were presented for the sessions was imported into the app. The first author was in the photograph as the use of human figures in the VSD serves to attract and maintain interest (Wilkinson et al., Citation2012). To provide contextual support, the figure in the VSD is reaching toward an object to indicate that the participant can have a desired object. The VSD was programmed with four hotspots which could be activated by touch to emit voice output. The grid display condition was configured with four cells in a 2 × 2 cell layout which were programmed to emit a voice recording when the cell was activated. Photographs were also used in this condition to ensure that different levels of symbol iconicity did not impact the results. Each child had an individualized VSD and grid display which was personalized according to the results of the motivator assessment.
Figure 1. Example of the tablet configured to visual scene display (left) and to the grid layout (right)

Procedures
General procedures were maintained across all the study phases. While in the waiting room, the participant was shown a photograph of the screen display which was used for each session; VSD or grid display. The researcher pointed to the items in the photo while saying ‘Today you can ask for these things using this picture‘. Each participant had two photographs reflecting the motivator sets identified in the motivator assessment to support discrimination between the two conditions (Schlosser, Citation2003).
All sessions lasted 20 min during which participants could request motivators as frequently as they desired. The motivators identified for the VSD and grid display conditions for each participant were made available on a shelf in the clinic room which was in sight but out of reach. On entering the room, the participant was directed to the items on the shelf and asked, ‘What do you want to do?’ The participant could select by pointing, reaching, or using the tablet. If the participant did not make a choice within 10 s, two motivators were selected by the researcher and offered to the participant to make a choice. If no choice was made within a further 10 s one of the motivators was replaced with another. This was continued until all four motivators were offered. Once a motivator was selected, natural routines were used to create opportunities for requesting, for example, during bubble play the clinician waited a maximum of 10 s for the child to initiate requesting (Halle, Citation1982). Motivators were provided immediately, and the clinician stated the name of the requested object paired with verbal reinforcement. Participants were able to request as frequently as desired.
Session schedule
Each participant attended for three sessions of 20 min duration on a weekly basis. All sessions were scheduled at the same time for each participant for all phases of the study. Randomization was used to determine the order of the treatments for each participant with no more than two consecutive sessions of the same treatment to ensure that the dimension of alternation of the two treatments would not be lost (Wolery, Citation2013). Randomization of participants and display formats was also applied to the tiers in the MPD.
Baseline
An initial measure of the participants’ spontaneous requesting skills using the tablet was obtained in the baseline against which the effects of the treatment could be measured. The 20-min session was divided into two 10-min sessions; one for each display condition to assess participant performance with both displays before intervention commenced (Gast et al., Citation2014). The order of the conditions was randomly decided for each participant. The tablet was available on the table during all baseline sessions. Participants were not directed to it or taught how to use it for requesting. Procedures as described above were used during this phase. All attempts to request motivators using pointing, reaching, or vocalizations were honored by the researcher by providing immediate access to the item, and appropriate verbal reinforcement was provided.
Intervention
Intervention sessions were identical to those in the baseline except that a prompting sequence utilizing most to least prompting adapted from Agius and Vance (Citation2016) was implemented to support the child to request using the tablet (). Participants were able to request reinforcing items as often as they wanted to within a 20 min period. The participant could make a request by pointing, reaching, or using the tablet. Procedures as described above were used to support requesting. The participants were allowed to play or consume items for as long as they wanted but to ensure requesting of at least two motivators per session, the researcher used the phrase; ‘let’s tidy up and choose something else’ if the child requested the same object for longer than 10 min.
Table 3. Prompting sequence
If the participant requested a different item from the current motivator, for example, if the child was playing with a ball, but touched bubbles on the tablet, a correspondence check in which both objects, i.e., the ball and the bubbles were offered to the child. If there was no correspondence, for example, the child touched bubbles but reached for the ball, a sequence was initiated to support the participant to correctly discriminate between visual options. The sequence utilized full physical prompting to teach the child to discriminate between the graphic symbols/hotspots on the tablet display once the child initiated a request for the desired item. Prompting was faded out gradually according to the prompting sequence described in .
Nathan required procedural modifications as he did not make progress in either of the conditions. After the eighth intervention session, the prompting procedure was altered to commence with 10 fully physically prompted consecutive trials at the start of the session to support Nathan to perform the full motor chain. Graduated guidance was then used.
Post-intervention
Each participant received three sessions identical to baseline in the post-intervention phase. Half of the participants randomly commenced with the VSD condition, the other half with the grid display condition to decrease sequence effects.
Follow-up
Maintenance was assessed in one session 4 weeks after the last post-intervention session using procedures identical to those in the baseline phase. Participants were randomly assigned to commence with either the VSD condition or the grid display condition.
Data collection and analysis
Direct systematic observational recording (DSOR) in which requesting behavior was observed and coded as it occurs by the communication partner was used to collect data on all requests for motivators for the duration of each session in all phases of the study (Ayres & Ledford, Citation2014). This enabled comparison of both the percentage of errors and sessions to criterion to compare the efficiency of two conditions (Schlosser, Citation2003). The percentage of independent responding was calculated post-hoc for each session using the formula: independent requests/(independent requests + prompted requests + incorrect requests)x100. The mastery criterion was considered achieved when the participant spontaneously requested on 80% of trials for two consecutive sessions.
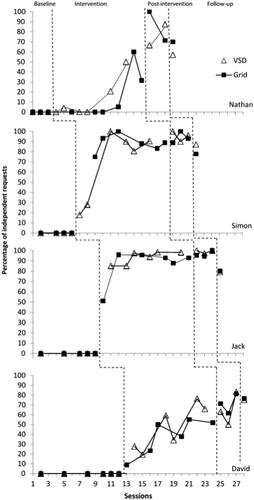
Data on requesting behavior was plotted on a line graph. Visual analysis was carried out on the graphed data to identify if there was a functional relationship between the introduction of the two treatments and requesting behavior of each participant (). Analysis involved a visual examination of the data for trend, level, and stability within and between the VSD and grid display conditions for each participant (Lane & Gast, Citation2014). In addition, Tau-U was calculated to evaluate the size of observed effects of the treatment (Parker et al., Citation2011). Tau-U yields a score between 0 and 1 which can be interpreted as follows; .20 or lower indicates a small effect; .20 and .60 is a moderate effect; between .60 and .80 is a large effect; and between .80 and 1 is a very large effect.
Figure 2. Percentage of correct requests for the VSD and grid display conditions
Procedural reliability
To assess reliability of the implementation of procedures, an independent observer who was a graduate SLT student collected live data in every third baseline and intervention session, and once in the post-intervention phase using a checklist of the procedural steps. Training of the observer consisted of implementing the checklist during live roleplays carried out by the first author and the OT until agreement was above 90%. Procedural reliability for each participant was collected in 32.1% of sessions. Reliability was calculated by dividing each step of the procedure implemented correctly by the total number of steps and multiplying by 100 to obtain a percentage. The overall mean for all four participants was 99%.
Interobserver agreement
For each session, percentages of agreement between the clinician and observer who collected live data on requesting behavior were calculated using the formula: agreements/(agreements + disagreements)x100 (Ayres & Ledford, Citation2014). Training of the observer who was a graduate speech and language therapy student was the same as that described for procedural reliability. Interobserver agreement ranged 94%-99% with an overall mean of 96% indicating strong agreement.
Results
presents the percentage of correct requests for the VSD and grid display conditions for the four participants. All four participants demonstrated a flat baseline; none requested using the tablet in either treatment condition. Simon activated the cells on the display in the first two baseline sessions to activate the voice output. Jack also demonstrated interest in the tablet systematically activating each hotspot/cell in both display conditions in three of the baseline sessions. David showed no interest in the tablet during the baseline sessions. Nathan attempted to exit the Scene and Heard app on several occasions but eventually stopped trying.
On introduction of the intervention, three participants demonstrated an immediate increase in the level of independent requesting for both conditions. Nathan demonstrated a delayed increase in independent requesting in both conditions. Simon and Jack achieved criterion in between 2 and 4 sessions for both conditions. Nathan and David failed to achieve criterion for both conditions, although an accelerating trend was evident during the intervention phase.
Tau-U was calculated for all participants, with no difference in the Tau-U score for any participant between the VSD and grid display conditions. Nathan’s Tau-U score was 0.5 (p = 0.2453) indicating a moderate effect. Simon’s Tau-U score was 1 (p = 0.0105) indicating a very large effect of the intervention in both display conditions. Similarly, for Jack the Tau-U score was 1 (p = 0.0062) indicating a very large effect, and for David the Tau-U score was also 1 (p = 0.0039) with a corresponding very large effect.
Nathan
Nathan failed to achieve criterion in both display conditions. Independent requesting using the tablet began after procedural modifications were made in session 8. Prior to this, Nathan was observed to exhibit sensory-seeking behaviors such as pressing his hands on the table or on the tablet display which prevented him from fully completing the required motor action to independently request. For the first 8 sessions, therefore, there was no overlap between the baseline and intervention conditions, and a flat trend was observed for both. After session 8 an accelerating trend was observed. During the intervention phase, Nathan requested with the VSD with 12.5% accuracy. Using the grid display, requesting accuracy was 16.1%.
Nathan missed one session in the post-intervention phase. In this phase, an accelerating trend was evident in the VSD condition while a decelerating trend was observed in the grid display condition. During post-intervention, Nathan requested independently at 74.1% in the VSD condition, and at 85.7% in the grid display condition. Independent requesting in the follow-up session was at a lower level than the post-intervention phase, particularly in the VSD condition (57.1%) when compared to the grid display (70%).
Simon
Simon achieved criterion in his fourth session in the VSD condition and in the third session in the grid display condition. The mean percentage of requesting was 67.9% in the VSD condition, and 88.9% in the grid display condition with an accelerating trend on introduction of the intervention. The data points overlapped on two occasions.
In the post-intervention phase, the mean level of requesting in both display conditions was higher than the intervention phase (87% in the VSD condition, and 77.8% in the Grid display condition). Simon’s independent requesting indicated a decelerating trend in the follow-up session as it was lower than the post-intervention phase (75% in the VSD condition, and 76.5% in the grid display) but requesting remained within criterion for both conditions.
Jack
Jack achieved criterion on the second and third sessions in the VSD and grid display conditions respectively with an accelerating trend evident in both once the intervention was introduced. Independent requesting was 93.1% in the VSD condition and 86.1% in the grid display condition. There were two overlap points where the data paths crossed between conditions. Anecdotally, Jack appeared to enjoy using the tablet to request from his first session. He smiled often and quickly learned to request with the tablet using fluid motor movements.
In the post-intervention phase, Jack continued to request within criterion levels in both display conditions (99.1% in the VSD condition and 96.7% in the grid display condition) exhibiting a continued increasing trend between the intervention and post-intervention phase for both conditions. Jack attended one follow-up session and requesting in both display conditions was lower than in the post-intervention phase but within criterion (79.2% and 80% in the VSD and grid display respectively). In the final sessions of intervention as well as post-intervention, and follow-up sessions, Jack made some errors due to activation of adjacent cells in the VSD condition which he self-corrected.
David
David failed to reach criterion in either of the intervention conditions although an immediate positive change in baseline requesting was evident when the intervention was introduced. He achieved a mean of 47.2% independent requests in the VSD condition and 37.9% was achieved in the grid display condition. A large number of errors in both conditions were due to touching the incorrect cell to request the desired motivator. From session 5 onwards, David began to pay greater attention to the hotspot/cell he was touching but engaged in multiple tapping behaviors resulting in accidental activation of cells adjacent to the desired hotspot/cell.
In the post-intervention phase, a gradual accelerating trend was evident in both display conditions (65.5% in the VSD condition and 71.4% in the grid display condition). Errors in both conditions continued to be due to multiple tapping on the display resulting in activation of adjacent cells. In the final follow-up session, the percentage of independent requesting was slightly lower than the last session of the post-intervention phase (75% and 76.5% in the VSD and grid display conditions respectively).
Discussion
The first aim of this study was to add to the existing literature that compares the use of a VSD with a grid display when teaching children with autism to request. The second aim was to extend on these previous studies by ensuring that iconicity was the same in both the VSD and grid display. The results of this study highlight the variability that can be found in children with autism in terms of learning to use AAC. Two of the participants, Simon and Jack, learned to use both the VSD and the grid in a similar timeframe so for them it appears that both a VSD and a grid were viable options in terms of learning to request. This resonates with findings from the Gevarter et al. (Citation2014, Citation2017, Citation2018) studies which suggest that children with autism can benefit from both types of displays. In the present study, however, Nathan and David did not achieve criterion in either display. The accelerating trend evident in Nathan and David’s results combined with the post-intervention and maintenance data indicated that they would possibly have done so had more intervention sessions been provided. The results suggest, therefore, that both displays may have been appropriate for them as well.
When comparing the number of sessions to criterion, two participants, Simon and Jack, met criterion for both display formats in between two and four sessions. Jack required three sessions to learn to use the grid and two for the VSD, while Simon needed four to learn to use the VSD and three for the grid. The extra session required in the grid and VSD conditions for Jack and Simon respectively could be due to the condition in which intervention commenced as Simon commenced with the VSD while Jack commenced with the grid display. Examination of the data indicates that in the early sessions, the data points were cumulative so that what was learned in one condition appeared to carry over to the other demonstrating a level of generalization from one display to another despite the use of two separate sets of motivators. As Simon and Jack were able to learn to use both display formats in a comparable timeframe there is a possibility that for them there was no ‘best’ display which resonates with Gevarter et al. (Citation2018) findings.
Taken overall, the study results did not provide any evidence that there was a particular benefit associated with using a VSD as a method of organizing vocabulary for any of the participants. This runs counter to what was expected given the literature, for example, Light et al. (Citation2018), which suggests that the organization of symbols into rows and columns which is typical of grid displays decontextualizes their meaning thereby increasing learning demands. In this study, the results were similar for both displays for all the children who were beginning communicators and therefore the contextual support provided by the VSD did not provide the anticipated benefits at the level of single requests. This was unexpected as the authors suggest that beginning communicators are the main target group of children who would benefit from VSDs, and this therefore leads to questions of how useful VSDs really are and if so, for whom and for which intervention goals.
In this study, all the participants were classified as beginning communicators yet two participants were able to learn to use both displays in a relatively small number of sessions. In such a scenario, one consideration could be the participants’ longer-term language needs. Participants who progress as quickly as Simon and Jack are likely to need access to a much wider range of vocabulary in a shorter space of time to support their language and communication development. Vocabulary needs to be organized in a way to facilitate the child to access it when needed, in a range of situations. ‘Just in time’ technology for adding additional displays to VSDs could be a solution as this allows fast programming of vocabulary (Drager et al., Citation2019), but it is not yet clear how the VSDs could be connected to each other to form a robust language system capable of supporting access to morphology and syntax in the longer term. Research has demonstrated that VSDs may support early semantic and pragmatic development for some children, yet it is acknowledged that they may not be as effective at supporting morphological and syntactical development and that further research is needed to understand how this could be accommodated (Light & McNaughton, Citation2012a, 2021b; Thistle & Thiessen, Citation2021). Given that Simon and Jack demonstrated the ability to learn both displays in a relatively short timeframe, it appears that a grid display would be a more suitable option to commence intervention with as it provides the opportunity for novel utterance generation, appearing to be better suited to support the development of more complex language structures for those who demonstrate potential for quick progress. This, then leads to questions; as all the participants in this study were beginning communicators, are there some children who display characteristics that render them more likely to make quicker, or for that matter slower progress? If so, what are these characteristics, and can they be identified during the assessment phase? How should such individual characteristics be matched to display characteristics? A better understanding of both child and display characteristics may support the clinician to choose a VSD or a grid at the outset.
In previous research, for example, Gevarter et al. (Citation2014, Citation2017) a photo was utilized for the VSD while line drawings were used in the grid displays. One of the main differences in the present study was the use of photographic material to represent vocabulary in both displays thus ensuring that iconicity was the same for both conditions. Of note in the study results was the number of errors that Simon made in the VSD, which were four times the number of errors in the grid display. One reason for this may have been because Simon’s intervention commenced with two sessions in the VSD and he was still learning to discriminate between the graphic symbols, but another possibility is that the irregular arrangement of the hotspots on the VSD resulted in a greater number of errors. It is possible that once iconicity was the same for both the VSD and grid displays other challenges relating to how the hotspots are organized on these displays emerged. The more irregular placement of hotspots in the VSD could lead to a greater number of errors with this kind of display as the less predictable placement of hotspots in VSDs could influence accuracy. Wilkinson and Jagaroo (Citation2004) suggest that one potential advantage of grid displays is that the structure may support the individual to remember the placement of the vocabulary. Automaticity in AAC is achieved when a task is successfully carried out without the need for significant cognitive load (Higginbotham et al., Citation2007). While it is theorized that VSDs may reduce cognitive load (Wilkinson et al., Citation2012), the hotspots in VSDs are not necessarily programmed in a predictable way thus potentially negatively influencing the development of automaticity. In the later sessions, Jack made more errors in the VSD, and this could be because automaticity was not as supported by the VSD structure. During those sessions, he did not look at the screen as intently as in the earlier sessions when requesting and his actions appeared more automatic. Further research is needed to determine the impact of the placement of vocabulary on displays as it is possible that a grid display arrangement may better support automaticity due to the organization of cells which affords greater predictability.
Overall, the results of this study suggest that each participant made similar progress in both displays yet there were notable differences between the participants in terms of how they progressed in the study, i.e., David and Jack achieved criterion, and Nathan and Simon did not. This is relevant as all four participants had a diagnosis of autism, were under the age of 6 years, were minimally verbal, and received the same intervention. Although only four participants took part in this study, understanding the differences between them could provide insight into why differences in responses emerged (Wolery, Citation2013).
Simon and Jake, who achieved criterion, had higher levels of overall adaptive functioning than Nathan and David suggesting that children diagnosed with autism who have lower levels of adaptive functioning may find it more difficult to learn to use aided AAC. These results appear to support the possibility that overall level of functioning may be a factor that predicts progress in learning to use aided AAC systems as suggested by Ganz et al. (Citation2011).
In relation to communication skills, David and Nathan presented with the lowest Total Gestures scores on the CDI-III and therefore lower levels of early communication skills at the outset of the study. Furthermore, David and Nathan also presented with the lowest receptive language scores indicating that when teaching children with autism to use tablets to communicate, low levels of receptive language should be factored into the clinician’s expectations. Romski and Sevcik (Citation1993) suggest that in such cases the child will take longer to establish the relationship between the graphic on the display and the real-world referent. It could be hypothesized that with low levels of early communication skills and low receptive language levels, the use of a VSD might support the child with autism to establish this relationship as the VSD may provide additional contextual clues. The results of this study, however, indicate that the VSD did not present any further advantage over the grid display layout.
Both Nathan and David presented with a co-morbid diagnosis of sensory processing disorder. Informal observations throughout the study indicated that these difficulties might have impeded their learning to request. This was especially evident in the initial stages, with Nathan, who sought deep pressure throughout those sessions. Assessment of sensory processing skills before commencing intervention could be considered as it could serve to determine if additional interventions are required to address sensory processing needs as an adjunct to the AAC intervention and for whom. It has been suggested that interventions aimed at targeting sensory processing differences may be utilized in conjunction with typical interventions with individuals who have autism and present with functional challenges related to sensory processing difficulties (Schaaf et al., Citation2014). Furthermore, research has begun to link specific profiles of sensory responsiveness with communication difficulties, for example, Feldman et al. (Citation2020) who recently published findings suggesting that certain sensory profiles are more likely associated with difficulties in communication and language in children with autism. Addressing Nathan and David’s sensory processing difficulties in conjunction with the AAC intervention might therefore have supported them to learn to use the tablet to make requests in a shorter timeframe although further research is required in this area.
Clinical implications
This study did not find any particular benefit of the use of VSDs for children with autism who are at the earliest stages of communication. This runs counter to the literature, for example., Light et al. (Citation2018). VSDs may, however, be useful to establish engagement and support early social interactions (Light & McNaughton, 2018). The study results do demonstrate that children with autism are capable of learning to use both VSDs and grid displays at similar rates of progress. In view of this, it is suggested to consider intervention goals as well as individual child characteristics when making decisions about which display to use.
For children with autism who present with higher adaptive functioning levels and appear to have stronger early communication skills development at the outset of intervention, it may be more appropriate to commence with a grid display which has the potential to provide access to more complex morphology and syntax at the outset. This is because for some children the use of a VSD could be restrictive, potentially limiting the possibility of generating novel sentences (Abbott & McBride, 2014)
Clinicians may also consider the sensory processing skills of children with ASD and its impact on learning to use AAC systems. This should be in addition to the current assessment guidelines which generally take into consideration existing communication skills and adaptive functioning (Ganz, Citation2011). When a child with autism presents with a co-morbid diagnosis of sensory processing disorder liaison with professionals such as Occupational Therapists who are skilled in providing interventions in this area may be key.
Limitations and future directions
Only four participants took part in the study, so it is not possible to generalize the findings to other children with ASD. A greater number of intervention studies would allow clinicians to better understand which kind of visual display is better for individual children.
The photographs used for the VSD condition in this study did not include the participant. Research has suggested that the use of people within these photos provides a social context that may be important for beginning communicators (Light et al., Citation2019). In view of this, research that includes VSDs with people in the photographs is recommended.
Longer-term studies that are designed to teach a wider range of linguistic functions may demonstrate other differences between VSDs and grid displays. This is important to understand how VSDs could be used to support the use of sentence generation. In view of this, studies that support children with ASD to learn to use tablets over longer periods of time may support a better understanding of the advantages of each of the display formats.
Social validity measures were not implemented so it is not known if the caregivers felt that the intervention was valuable and if they felt that one type of display was more acceptable than the other.
Conclusion
In this study, differences in the progress made between the children were evident, yet there did not appear to be any great difference between the learning of the VSD and the grid display for any of them. While it has been suggested that the characteristics of children with autism could impact the selection of and progress in learning to use AAC systems, it is also important to consider the linguistic potential of each display format. Decisions should be made according to the best fit for the individual child and the linguistic goals for that child.
It is suggested that VSDs could be suitable for children with ASD who are at very early levels of communication development and have lower adaptive functioning levels and for whom VSDs could be used to support early social interactions. For children who present with higher levels of adaptive functioning and communication skills at the outset, a grid display should be considered as it is more likely to provide access to morphology and syntax to support language development.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 The iPad® is a mainstream tablet produced by Apple Inc.
2 The Big Grips® cover is produced by KEM Ventures Inc.
3 The Scene and Heard® app version 3.0. is an app registered by Therapy Box Ltd.
References
- Abbot, M. A., & McBride, D. (2014). AAC decision-making and mobile technology: Points to ponder. Perspectives on Augmentative and Alternative Communication, 23(2), 104–111. https://doi.org/10.1044/aac23.2.104
- Agius, M. M., & Vance, M. (2016). A comparison of PECS and iPad to teach requesting to preschoolers with autistic spectrum disorders. Augmentative and Alternative Communication, 32(1), 58–68. https://doi.org/10.3109/07434618.2015.1108363
- Aydin, O., & Diken, I. H. (2020). Studies comparing augmentative and alternative communication systems (AAC) applications for individuals with autism spectrum disorder: A systematic review and meta-analysis. Education and Training in Autism and Developmental Disabilities, 55(2), 119–141.
- Ayres, K., & Ledford, J. (2014). Dependent measures and measurement systems. In D. L. Gast & J. R. Ledford (Eds.), Single case research methodology: Applications in special education and behavioral sciences. (pp.124–153). Routledge/Taylor & Francis Group.
- Blackstone, S., Light, J., Beukelman, D., & Shane, H. (2004). Visual scene displays. Augmentative Communication News, 16(2), 1–16.
- Caron, J., & Holyfield, C. (2019). High-tech aided AAC for individuals with autism spectrum disorder and complex communication needs. In J. B. Ganz & R. L. Simpson (Eds.), Interventions for individuals with autism spectrum disorder and complex communication needs. (pp. 103–128). Paul Brookes Publishing Co.
- Carnett, A., Martin, C., & Gevarter, C. (2021). Evaluating augmentative and alternative communication modalities for individuals with developmental disabilities: A brief review of the last 5 years. Current Developmental Disorders Reports, 8(2), 133–141. https://doi.org/10.1007/s40474-021-00226-0
- Drager, K. D., Light, J. C., Carlson, R., D'Silva, K., Larsson, B., Pitkin, L., & Stopper, G. (2004). Learning of dynamic display AAC technologies by typically developing 3-year-olds. Journal of Speech, Language, and Hearing Research, 47(5), 1133–1148. https://doi.org/10.1044/1092-4388(2004/084)
- Drager, K., Light, J., Currall, J., Muttiah, N., Smith, V., Kreis, D., Nilam-Hall, A., Parratt, D., Schuessler, K., Shermetta, K., & Wiscount, J. (2019). AAC technologies with visual scene displays and ‘Just in Time’ programming and symbolic communication turns expressed by students with severe disability. Journal of Intellectual & Developmental Disability, 44(3), 321–336. https://doi.org/10.3109/13668250.2017.1326585
- Feldman, J. I., Cassidy, M., Liu, Y., Kirby, A. V., Wallace, M. T., & Woynaroski, T. G. (2020). Relations between sensory responsiveness and features of autism in children. Brain Sciences, 10(11), 775. https://doi.org/10.3390/brainsci10110775
- Fenson, L., Bates, E., Dale, P. S., Marchman, V. A., Reznick, J. S., & Thal, D. J. (2007). MacArthur-Bates communicative development inventories. Paul H. Brookes Publishing Company.
- Ganz, J. B., Earles-Vollrath, T. L., Heath, A. K., Parker, R. I., Rispoli, M. J., & Duran, J. B. (2012). A meta-analysis of single case research studies on aided augmentative and alternative communication systems with individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(1), 60–74. https://doi.org/10.1007/s10803-011-1212-2
- Ganz, J. B., Earles-Vollrath, T. L., Mason, R. A., Rispoli, M. J., Heath, A. K., & Parker, R. I. (2011). An aggregate study of single-case research involving aided AAC: Participant characteristics of individuals with autism spectrum disorders. Research in Autism Spectrum Disorders, 5(4), 1500–1509. https://doi.org/10.1016/j.rasd.2011.02.011
- Gast, D. L., Lloyd, B. P., & Ledford, J. R. (2014). Multiple baseline and multiple probe designs. In J. R. Ledford and D. L. Gast (Eds.), Single case research methodology: Applications in special education and behavioral sciences. (pp.251–296). Routledge/Taylor & Francis Group.
- Gevarter, C., Horan, K., & Sigafoos, J. (2020). Teaching preschoolers with autism to use different speech-generating device display formats during play: Intervention and secondary factors. Language, Speech, and Hearing Services in Schools, 51(3), 821–838. https://doi.org/10.1044/2020_LSHSS-19-00092
- Gevarter, C., O’Reilly, M. F., Kuhn, M., Watkins, L., Ferguson, R., Sammarco, N., Rojeski, L., & Sigafoos, J. (2017). Assessing the acquisition of requesting a variety of preferred items using different speech generating device formats for children with autism spectrum disorder. Assistive Technology, 29(3), 153–160. https://doi.org/10.1080/10400435.2016.1143411
- Gevarter, C., O’Reilly, M. F., Rojeski, L., Sammarco, N., Sigafoos, J., Lancioni, G. E., & Lang, R. (2014). Comparing acquisition of AAC-based mands in three young children with autism spectrum disorder using iPad® applications with different display and design elements. Journal of Autism and Developmental Disorders, 44(10), 2464–2474. https://doi.org/10.1007/s10803-014-2115-9
- Gevarter, C., O'Reilly, M. F., Sammarco, N., Ferguson, R., Watkins, L., Kuhn, M., & Sigafoos, J. (2018). Comparison of schematic and taxonomic speech generating devices for children with ASD. Education and Training in Autism and Developmental Disabilities, 53(2), 222–238.
- Green, V. A., Sigafoos, J., Didden, R., Lancioni, G. E., Ollington, N., & Payne, D. (2008). Validity of a structured interview protocol for assessing children’s preferences. In P. Grotewell & Y. Burton (Eds.), Early childhood education: Issues and developments. (pp.87–103). Nova Science Publishers Inc.
- Halle, J. W. (1982). Teaching functional language to the handicapped: An integrative model of natural environment teaching techniques. Research and Practice for Persons with Severe Disabilities, 7(4), 29–37. https://doi.org/10.1177/154079698200700404
- Higginbotham, D. J., Shane, H., Russell, S., & Caves, K. (2007). Access to AAC: Present, past, and future. Augmentative and Alternative Communication, 23(3), 243–257. https://doi.org/10.1080/07434610701571058
- Holyfield, C., Caron, J., & Light, J. (2019). Programing AAC just-in-time for beginning communicators: The process. Augmentative and Alternative Communication, 35(4), 309–318. https://doi.org/10.1080/07434618.2019.1686538
- Iacono, T., Trembath, D., & Erickson, S. (2016). The role of augmentative and alternative communication for children with autism: Current status and future trends. Neuropsychiatric Disease and Treatment, 12, 2349–2361. https://doi.org/10.2147/NDT.S95967
- Kang, S., O’Reilly, M., Lancioni, G., Falcomata, T. S., Sigafoos, J., & Xu, Z. (2013). Comparison of the predictive validity and consistency among preference assessment procedures: A review of the literature. Research in Developmental Disabilities, 34(4), 1125–1133. https://doi.org/10.1016/j.ridd.2012.12.021
- Lane, J. D., & Gast, D. L. (2014). Visual analysis in single case experimental design studies: Brief review and guidelines. Neuropsychological Rehabilitation, 24(3–4), 445–463. https://doi.org/10.1080/09602011.2013.815636
- Light, J., & McNaughton, D. (2012a). Supporting the communication, language, and literacy development of children with complex communication needs: State of the science and future research priorities. Assistive Technology, 24(1), 34–44. https://doi.org/10.1080/10400435.2011.648717
- Light, J., & McNaughton, D. (2012b). The changing face of augmentative and alternative communication: Past, present, and future challenges. Augmentative and Alternative Communication, 28(4), 197–204. https://doi.org/10.3109/07434618.2012.737024
- Light, J., McNaughton, D., & Caron, J. (2018). New and emerging AAC technology supports for children with complex communication needs and their communication partners: State of the science and future research directions. Augmentative and Alternative Communication, 35(1), 26–41. https://doi.org/10.1080/07434618.2018.1557251
- Light, J., Wilkinson, K. M., Thiessen, A., Beukelman, D. R., & Fager, S. K. (2019). Designing effective AAC displays for individuals with developmental or acquired disabilities: State of the science and future research directions. Augmentative and Alternative Communication, 35(1), 42–55. https://doi.org/10.1080/07434618.2018.1558283
- Lord, C., Rutter, M., Dilavore, P., Risi, S., Gotham, K., & Bishop, S. (2012). Autism diagnostic observation schedule. (2nd ed.). Western Psychological Services.
- Luyster, R., Lopez, K., & Lord, C. (2007). Characterizing communicative development in children referred for autism spectrum disorders using the MacArthur-Bates communicative development inventory (CDI). Journal of Child Language, 34(3), 623–654. https://doi.org/10.1017/s0305000907008094
- McIntosh, D. N., Miller, L. J., Shyu, V., & Dunn, W., (1999). Overview of the short sensory profile. In. W. Dunn (Ed.), Sensory profile user’s manual. (pp.59–73) Pearsons.
- Mirenda, P. (2008). A back door approach to autism and AAC. Augmentative and Alternative Communication, 24(3), 220–234. https://doi.org/10.1080/08990220802388263
- Mirenda, P. (2009). Introduction to AAC for individuals with autism spectrum disorders. In P. Mirenda & T. Iacono (Eds.), Autism spectrum disorders and AAC. (pp.3–22). Paul. H. Brookes Publishing Co.
- Parker, R. I., Vannest, K. J., Davis, J. L., & Sauber, S. B. (2011). Combining nonoverlap and trend for single-case research: Tau-U. Behavior Therapy, 42(2), 284–299.
- Romski, M., & Sevcik, R. A. (2005). Augmentative communication and early intervention: Myths and realities. Infants & Young Children, 18(3), 174–185. https://doi.org/10.1097/00001163-200507000-00002
- Romski, M. A., & Sevcik, R. (1993). Language comprehension: Considerations for augmentative and alternative communication. Augmentative and Alternative Communication, 9(4), 281–285. https://doi.org/10.1080/07434619312331276701
- Rose, V., Trembath, D., Keen, D., & Paynter, J. (2016). The proportion of minimally verbal children with autism spectrum disorder in a community‐based early intervention programme. Journal of Intellectual Disability Research, 60(5), 464–477. https://doi.org/10.1111/jir.12284
- Schaaf, R. C., Benevides, T., Mailloux, Z., Faller, P., Hunt, J., Van Hooydonk, E., Freeman, R., Leiby, B., Sendecki, J., & Kelly, D. (2014). An intervention for sensory difficulties in children with autism: A randomized trial. Journal of Autism and Developmental Disorders, 44(7), 1493–1506. https://doi.org/10.1007/s10803-013-1983-8
- Schlosser, R. W. (2003). The Efficacy of augmentative and alternative communication. Academic Press.
- Sievers, S. B., Trembath, D., & Westerveld, M. F. (2018). A systematic review of predictors, moderators, and mediators of augmentative and alternative communication (AAC) outcomes for children with autism spectrum disorder. Augmentative and Alternative Communication, 34(3), 219–229. https://doi.org/10.1080/07434618.2018.1462849
- Simpson, R. L. (2019). Characteristics of individuals with autism spectrum disorder who have complex communication needs. In: J. B. Ganz & R. L. (Eds.), Interventions for individuals with autism spectrum disorder and complex communication needs. (pp.3–20). Paul H. Brookes Publishing Co.
- Sparrow, S. S., Cicchetti, D. V., Balla, D. A., & Doll, E. A. (2005). Vineland adaptive behavior scales: Survey forms manual. AGS Publishing.
- Tager-Flusberg, H., Rogers, S., Cooper, J., Landa, R., Lord, C., Paul, R., Rice, M., Stoel-Gammon, C., Wetherby, A., & Yoder, P. (2009). Defining spoken language benchmarks and selecting measures of expressive language development for young children with autism spectrum disorders. Journal of Speech, Language and Hearing Research, 52(3), 643–652. https://doi.org/10.1044/1092-4388(2009/08-0136)
- Thiessen, A., Thistle, J., & Brown, J. (2021). Clinical and research perspectives on visual scene displays. American Journal of Speech-Language Pathology, 30(3), 1134–1156.
- von Tetzchner, S. (2015). The semiotics of aided language development. Cognitive Development, 36, 180–190. https://doi.org/10.1016/j.cogdev.2015.09.009
- Wilkinson, K. M., & Jagaroo, V. (2004). Contributions of principles of visual cognitive science to AAC system display design. Augmentative and Alternative Communication, 20(3), 123–136. https://doi.org/10.1080/07434610410001699717
- Wilkinson, K. M., Light, J., & Drager, K. (2012). Considerations for the composition of visual scene displays: Potential contributions of information from visual and cognitive sciences. Augmentative and Alternative Communication, 28(3), 137–147. https://doi.org/10.3109/07434618.2012.704522
- Wolery, M. (2013). A commentary: Single-case design technical document of the What Works Clearinghouse. Remedial and Special Education, 34(1), 39–43. https://doi.org/10.1177/0741932512468038
- Wolery, M., Gast, D., & Ledford, J. (2014). Comparison designs. In J. Ledford & D. Gast (Eds.), Single case research methodology: Applications in special education and behavioral sciences. (pp.297–345). Routledge/Taylor & Francis Group.