
Abstract
This study explores how providing assisted dying services affects the psychological distress of practitioners. It investigates the influence of professional norms that endorse such services within their field. Study 1 included veterinarians (N = 137, 75.2% female, Mage = 43.1 years, SDage = 12.7 years), and Study 2 health practitioner students (N = 386, 71.0% female, Mage = 21.0 years, SDage = 14.4 years). In both studies, participants indicated their degree of psychological distress following exposure to scenarios depicting assisted dying services that were relevant to their respective situations. In Study 1, we found that higher willingness to perform animal euthanasia was associated with lower distress, as were supportive norms. In Study 2, a negative association between a greater willingness to perform euthanasia and lower psychological distress occurred only when the provision of such services was supported by professional norms. In conclusion, psychological distress is buffered by supportive professional norms.
Introduction
Although the appropriateness of assisted dying services for humans has been debated by scholars from many disciplines (Cartwright et al., Citation2006; Cuman & Gastmans, Citation2017), many countries and states have developed policies to legalize the services. For example, with various qualifying conditions, assisted dying is currently legal in Switzerland, the Netherlands, Spain, Belgium, Luxembourg, Canada, Colombia, New Zealand, Australia (Bellens et al., Citation2020; Verhofstadt et al., Citation2020) and some states in the US (e.g., Colorado, Oregon, Hawaii, etc.). In many other countries, the practice remains illegal, but is the subject of public debates and controversies within communities, as well as amongst practitioners who ultimately deliver the services (Stolz et al., Citation2015).
There are many terms used to refer to the services (e.g., euthanasia, assisted dying, assisted suicide, and medical assistance in dying). However, many scholars and practitioners distinguish euthanasia from assisted suicide (Andriessen et al., Citation2020). Defined narrowly, euthanasia refers to a procedure where a physician administers medication that causes a patient’s death, or in the case of an animal, a veterinarian conducts a procedure to end an animal’s life (Głębocka, Citation2018; Stolz et al., Citation2015). In contrast, assisted dying allows patients to hasten their own death with someone else’s help. In physician-assisted dying, a physician provides medication to the patient and may give instructions on how to take it, but they do not inject the medication or help the patient to swallow it (Curry et al., Citation2000). However, in Canada, Medical Assistance in Dying (MAID), the legal term used to govern assisted dying services includes the two methods: a physician or nurse practitioner directly administers a substance that causes death; and a physician or nurse practitioner provides or prescribes a drug that the eligible person takes themselves. In some cases, public or community views may have driven decisions defining what assisted dying is and how it is offered, independent of practitioner controversies (Brenna, Citation2021). Assisted dying laws are often enacted in the face of opposition by medical associations and professional societies (Brooks, Citation2019).
This research focuses on the reported psychological effects of offering assisted dying services (defined inclusively to encompass practices including euthanasia, assisted suicide, and medical assistance in dying) on practitioners’ own distress. Offering assisted dying services has been linked to practitioners’ psychological distress (Piers et al., Citation2012; Range & Rotherham, Citation2010) and ill health (Stevens, Citation2006). Psychological distress (as distinct from emotional distress; we return to this distinction in the discussion) is a state of suffering associated with stressors and demands that are perceived to be difficult to cope with in daily life (Arias-Ulloa et al., Citation2023). Given this context of practitioner risk, in two studies, we explore the relationship of supportive norms to willingness and psychological distress in assisted dying in veterinarians and human health practitioners. Our research questions are threefold: (1) Are practitioners with lower willingness to offer services at greater risk of psychological distress? (2) Do supportive professional norms lower psychological distress? and (3) Is the association of willingness to offer assisted dying services with psychological distress weaker when there norms are supportive, compared to when norms are less supportive?
Assisted dying services and psychological distress
Although laws supporting assisted dying services for human patients are relatively recent, a small body of research has highlighted the mental health implications for practitioners involved in such services. These include emotional pressures (Trankle, Citation2014), negative feelings and frustration (Bellens et al., Citation2020), apprehension and discomfort (Głębocka, Citation2018), and emotional and moral distress (Georges et al., Citation2008; Lokker et al., Citation2018; & Rietjens et al., Citation2014). Physicians and nurses are among the health practitioners most often confronted with patients’ requests for assisted dying and may be among those involved in providing it when the request is approved (Meeussen et al., Citation2011).
In addition to the research mentioned above, a rationale for concern is that veterinarians have been identified as having more than twice the prevalence of suicide than professionals in the dental profession, and four times the rate in the general population; furthermore, exposure to animal euthanasia is identified as one of the profession’s risk factors (Dalum et al., Citation2024; Stoeven, Citation2015; Witte et al., Citation2019). Engagement in euthanizing animals may impact veterinarians’ perceptions of death, potentially leading to self-justification and reduced inhibitions toward viewing suicide as a rational response to life’s challenges, if they have inadequate professional supports (Stoeven, Citation2015). Other than that, more frequent involvement in euthanizing animals is associated with serious suicidal thoughts (Dalum et al., Citation2024). However, others have argued that psychological distress may arise regardless of euthanasia per se and be associated with witnessing the suffering of animals and dealing with clients’ emotions, which can take a significant toll on practitioners’ mental health. In this research, we seek to test whether veterinarians experience varying levels of psychological distress depending on whether euthanasia falls within normative or non-normative contexts, or whether the psychological distress is consistent regardless of norms (Crane et al., Citation2023).
Norms around assisted dying services
One survey of 909 physicians in the USA may indirectly provide insight into relevant norms of medical practitioners and found two key concerns among physicians (Curry et al., Citation2000). The Hippocratic oath, that affirms physicians’ primary duty to do no harm, is perceived among some medical practitioners to be in conflict with providing assisted dying services, threatening the credibility of the medical profession. In addition, they also feared the potential for abuse in vulnerable populations and where family members or medical practitioners face financial incentives for misuse. This may suggest that many practitioner’s perceptions of professional norms do not support assisted dying services. In contrast, other themes were reported among medical practitioners who support the legalization of assisted dying services, including the belief that such services are outcomes of compassion and alleviate suffering, and that assisted dying respects patients’ self-determination in the human context and allows to express compassion (Beuthin et al., Citation2018; Curry et al., Citation2000; Georges et al., Citation2008).
Psychological distress related to assisted dying services arises not only from direct involvement in the service, but also when health practitioners are faced with requests for the service (Georges et al., Citation2008). Health practitioners may experience distress in such situations and may opt for an avoidant coping mechanism, avoiding consideration or approval of the requests (Georges et al., Citation2008). However, factors that influence health practitioners’ distress regarding their involvement in assisted dying services also include specific regulations governing assisted dying services in the country, adherence to professional norms, and support from colleagues (Wibisono et al., Citation2022).
The roles of willingness and norms
One implication of the previous research is that the experience of distress from offering assisted dying services varied depending on practitioners’ willingness to offer the practice (Range & Rotherham, Citation2010; Rice et al., Citation2008). Empirical findings, however, are ambiguous on this point. In one descriptive analysis, 64% of nurse participants reported distress associated with involvement in assisted dying (Rice et al., Citation2008). However, little research has examined the association between willingness to offer assisted dying services and distress explicitly (Range & Rotherham, Citation2010).
Research on controversial actions and wellbeing reveals that the association between attitudes and the mental health outcome of a specific behavior is also likely to be affected by social norms, which are shared standards for what is seen as acceptable and right in a given context (Cislaghi & Heise, Citation2018; Lizzio-Wilson et al., Citation2023). Supportive norms (that is, norms that suggest that important others endorse the action or behavior) increase the likelihood that an attitude will be expressed behaviorally (Terry et al., Citation1999). In addition, social norms affect the mental health implications of enacting particular behaviors, with supportive norms generally reducing distress (Cislaghi & Heise, Citation2018). However, the impact of social norms in influencing the mental health implications willingness to engage in assisted dying services for practitioners have not been addressed to our knowledge.
In the context of assisted dying services, we focus on professional norms referring to the accepted and established standards of behaviors, beliefs, and values within professional communities and organizations regarding the practice (Wibisono et al., Citation2022). Therefore, to determine whether certain instances of assisted dying services are in line with norms or not, factors such as legal frameworks and professionals’ ethical consensus need to be considered. Although medical and veterinary professions may have settled professional norms, these norms can be influenced by larger factors such as religious and cultural factors, a point we return to in the discussion.
The present research
In the present research, we examine association between willingness to offer assisted dying services and psychological distress, and the moderating effects of professional norms in that association, in contexts where assisted dying services has been legalized. In two studies, we invited participants who were veterinarians (Study 1), and student health practitioners (Study 2) to consider and respond to scenarios of normative and non-normative animal euthanasia or assisted dying services, and to report their willingness to engage with the service, as well as their psychological distress. Professional norms were experimentally manipulated using scenarios. In Study 1, the normative animal euthanasia scenario featured animals experiencing intense pain, while in the non-normative scenario, the owner is considering putting the animal down for lifestyle reasons (Study 1). In Study 2, the normative assisted dying scenario featured a known patient with terminal illness who is sharp, confident of their decision, and fully supported by their family, while in the non-normative scenario, the patient is unknown, confused, anxious, and does not have family support. To determine whether the conditions were perceived by participants as normative vs. non-normative situations, we incorporated a manipulation check based on past research (Smith & Louis, Citation2008).
H1: Individuals with lower willingness to engage in assisted dying are hypothesized to be at greater risk of psychological distress.
H2: Professional norms that support assisted dying services lower psychological distress.
H3: A two-way interaction is anticipated in predicting distress between professional norms that support assisted dying services and willingness to engage in providing the services. Specifically, we expect that more supportive professional norms reduce the negative association of willingness with psychological distress.
Study 1
Participants
Participants were 137 practicing veterinarians recruited by sending an email via the Australian Veterinarian Association’s e-journal, group emails sent through state veterinary boards, social media advertisements, and emails sent out by the researchers in snowball sampling.Footnote1 Four participants were excluded based on an attention check question (i.e., “Please answer “a little” for this item”) and their consent to participate, leaving 133 participants in the analysis. Participants’ ages ranged from 23 to 75 years (Mage = 43.1, SDage = 12.7) and the majority were female (75.2%; male = 24.8%). Most of the participants (63.2%) worked full-time as veterinarians, while the rest were working part-time (26.3%), casually (6.8%), on leave (1.5%), or unemployed (2.3%).
Procedures and materials
Participants were invited to complete a survey on veterinarian well-being and euthanasia in Qualtrics, with the ethical clearance for this study granted by HREC Humanities and Social Sciences Committee at Macquarie University (Reference number: 52019610712349). Upon reading the information sheet and providing their written consent, the items measuring demographic variables were completed. Participants were then randomly exposed to a scenario of normative vs. non-normative euthanasia, in which they were presented with a scenario of a client requesting their dog to be euthanized and were asked to imagine themselves as the attending veterinarian. Random assignment allowed every participant to have an equal chance of being in either the normative or non-normative euthanasia manipulation condition. In the normative euthanasia scenario (coded +1), the dog has arthritis and is unable to enjoy basic pleasures anymore (e.g., food and walks). The client also has lifestyle reasons related to travel and family. In the non-normative scenario (coded −1), nothing is physically wrong with the dog, however the client has lifestyle reasons related to travel and family for euthanizing the dog. After considering the scenario, participants were asked to complete the manipulation check item (i.e., perceived supportive norms), as well as measures of willingness to euthanize, and experience of distress. Please refer to the supplementary materials for the complete materials and measures applied in Study 1.
Measures
We developed the manipulation and measures for the purpose of the study, considering the nature of the sample and the fact that participants are very busy with their tasks as health practitioners. Therefore, we did not apply the standardized long measures for some variables; instead, we focused on the operational definition of the psychological constructs, and the face validity of the scales.
Manipulation check
Participants responded to three items adapted from Smith and Louis (Citation2008) to evaluate perceived norms for the euthanasia decision (e.g., “Other veterinarians would agree that the animal should be euthanized”) on 7-point scales from 1 (not at all true) to 7 (very true). These items aimed to test the different levels of perceived norms. Participants exposed to the normative scenario should have significantly greater level of perceived normative support than those exposed to the non-normative scenario. Scores were averaged to create a measure of perceived supportive norms (α = .94).
Willingness to euthanize
Participants rated the probability that they would euthanize the animal on a scale from 0% (not at all likely; coded 1) to 100% (definitely likely; coded 10).
Psychological distress
Participants reported the extent to which they believed that they would experience distressing thoughts and feelings with five items (e.g., “A situation like this would be distressing for me”, “This situation would be likely to cause stress for me”) measured on a 7-point scale from 0 (not at all) to 6 (a lot). Scores were averaged to create a measure of greater perceived distress (α = .94).
Results
Manipulation check analysis
An independent sample t-test confirmed the success of the manipulation, showing that the participants exposed to the normative animal euthanasia scenario perceived more supportive norms for animal euthanasia (M = 4.5, SD = 1.4) than the participants exposed to the non-normative animal euthanasia scenario (M = 1.9, SD = 1.0), t(131) = 12.28, p < .001, Cohen’s d = 1.20.
Descriptive statistics and inter-correlations
As shown in , distress was negatively correlated with both willingness to euthanize and manipulated norms, ps < .001. In addition, norms had a positive association with willingness to perform animal euthanasia such that participants considering normative animal euthanasia had greater willingness to euthanize than the participants considering non-normative animal euthanasia, p <.001.
Table 1. Descriptive statistics and inter-correlations in Study 1.
The effects of manipulated norms, willingness to euthanise and their interaction on veterinarians’ distress
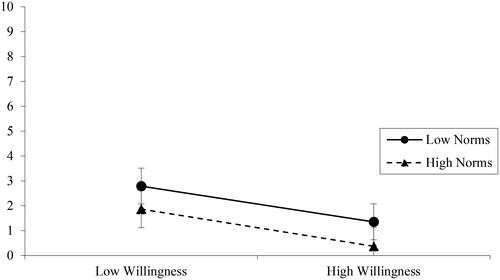
As presented in , in Block 1, willingness and norms were entered together and explained 51% of the variance in psychological distress, Fch(2, 130) = 67.47, p < .001. To answer the research question 1, are practitioners with lower willingness to offer animal euthanasia at greater risk of distress, we considered the unique relationship as reported in the multiple regression, and we indeed found that participants who were more willing to euthanize the animal showed lower levels of psychological distress, 𝛽 = −.50, p < .001, sr2 = .17. In addition, to answer the research question 2, do supportive norms lower psychological distress, we found that norms also had a negative influence on psychological distress, such that those considering normative (vs. non-normative) euthanasia had lower levels of distress, 𝛽 = −.30, p < .001, sr2 = .06. In Block 2, the interaction term was added to the model to test the research question 3. The interaction did not account for a significant increase in variance, Fch(1, 129) = 0.02, 𝛽 = −.01, p = .900, R2ch < .01.
Table 2. Moderated multiple regression analyses for distress in Study 1.
As presented in , parallel negative associations between willingness to perform animal euthanasia and psychological distress were found for veterinarians in both normative and non-normative conditions.
Figure 1. Simple slopes analysis shows there is no interaction between willingness to euthanize and norms in predicting the level of participants’ distress in Study 1.
Indirect effect of norms on psychological distress
Further analysis explored whether the high correlations between norms and willingness to perform animal euthanasia, and between willingness and psychological distress, were indicative of an indirect effect of norms upon distress via changing willingness to euthanize. The hypothesized mediation model was tested using PROCESS computation Model 4 with SPSS by applying Bootstrapping analysis with 5,000 resamples (Hayes, Citation2013). The data showed that norms positively predicted willingness to euthanize, 𝛽 = .56, p <.001, CI [1.41, 2.36], and greater willingness to euthanize negatively predicted the distress, 𝛽 = −.50, p <.001, CI [−0.28, −0.15]. In addition to the negative direct effect of norms on distress as reported above, in which the participants exposed to non-normative situation had a greater level of distress, 𝛽 = −.30, p < .001, CI [-0.67, −0.23], there was also a significant indirect effect via greater willingness, standardized IE = −.28, CI [-0.40, −0.17]. Thus, supportive norms increased participants’ willingness to euthanize, and the higher willingness could reduce participants’ psychological distress regarding offering the service.
Discussion
In the following paragraphs, we provided the summary of the results, and delved into a detailed discussion of each research question individually. Study 1 found that willingness to euthanize was directly associated with lower psychological distress on veterinarians. Moreover, regarding research question 2, normative support from professional groups led to higher willingness to euthanize, and lower levels of psychological distress. Regarding research question 3, group norms did not significantly moderate the association of willingness to euthanize with distress in the context of animal euthanasia. Instead, norms exerted a significant indirect effect to lower psychological distress via strengthened willingness to perform animal euthanasia.
It is important to note that there is theoretical justification for the findings that norms directly lower distress (Keohane & Richardson, Citation2018) and shape attitudes (Dempsey et al., Citation2018), but they could also moderate the willingness-distress link (see Amiot et al., Citation2013, Citation2020). Thus, we considered that the different paths might operate with different strengths depending on the power of norms and the different contexts. Here, in the context of veterinarians, we found that manipulated norms had a dominant role in driving an indirect effect on distress via willingness: supportive norms led to greater willingness, which was associated with lower distress.
Study 2
We examined the interpretation of Study 1’s findings in Study 2, which was conducted among health practitioner students. Compared to the management of pain and suffering through assisted dying services in veterinary practice, such services are more controversial for human health practitioners, more recently introduced, and therefore perhaps less supported by professional norms.
Participants
Health practitioner students in medicine, nursing, and psychology (N = 386) were screened based on their statement on informed consent items (one participant was excluded); level of completion (96 participants were excluded); and their answer on attention check item (i.e., “Please answer ‘2 Disagree’ on this item to show you are paying attention”; n = 30 were excluded). The final sample of participants (N = 259) was predominantly female (71% female, 25% male, 2% non-binary, 2% other) and relatively young (Mage = 21.0 years old, SDage = 14.4 years). The criteria that we used was to recruit student practitioners from professions which come into contact with end-of-life patients and requests for assisted dying, which (in the jurisdiction sampled) include nurses, doctors, and others such as psychologists who may be called to assess competencies for decision-making, to attempt to treat depression, or to alleviate psychological distress.
Procedures and materials
The design of Study 1 was replicated in Study 2 and adapted to the context of health practitioners considering scenarios of normative vs. non-normative assisted dying services. Ethical clearance for this study was granted by the Ethics Committee at University of Queensland (Project number: 2021/HE001341). In the survey, screening questions (e.g., whether they were intending to practice as health practitioners, and in which professions) were followed by demographic variables and then participants were randomly assigned to either the normative or non-normative assisted dying condition. Participants read a scenario in which they were a health practitioner assessing a patient for assisted dying services in a State where these services are legalized. In the normative scenario (coded +1), the patient had less than six months to live, had no mental health issues, and was fully supported by their family. The normative condition met all legal criteria in the Australian States where these services are legal. In the non-normative scenario (coded −1), the patient was terminally ill, but the timeframe was unclear, they had mental health issues, and their family members were opposed to their request. The non-normative condition met some legal criteria for suitability (e.g., terminal illness), but it was not clear whether it met other criteria (e.g., expectations of imminent death). After considering the scenarios, participants completed a measure of perceived norms as the manipulation check, as well as measures of willingness to offer assisted dying and distress. Please refer to the supplementary materials for the complete materials and measures applied in Study 2.
Measures
As in Study 1, we developed the manipulation and measures for the purpose of the study. Considering the nature of the participants, we did not apply the standardized long measures, instead, we focused on the operational definition of the psychological constructs, and the face validity of the scales.
Manipulation check
A single item adapted from Smith and Louis (Citation2008) was used as a manipulation check: “In this situation, the average health professional would offer assisted dying services when requested by the patient”. Participants were asked to rate their agreement with the statement in a 7-point Likert rating from 1 (Strongly disagree) to 7 (Strongly agree).
Willingness to participate in assisted dying services
A single item was used to measure participants’ willingness: “Based on the scenario you have just considered, how willing would you be to provide services for this patient for voluntary assisted dying?”. A 7-point Likert rating was applied from 1 (Very unlikely) to 7 (Very likely).
Distress
The extent to which participants feel distressed after exposure to the assisted dying scenario was assessed with a single item, “To what extent is this scenario personally distressing you?”. Participants responded on a 7-point Likert scale from 1 (Not at all) to 7 (Very much).
Results
Manipulation check analysis
As expected, an independent sample t-test showed that participants exposed to the normative scenario perceived more supportive norms (M = 5.2, SD = 1.3) than the participants exposed to the non-normative scenario (M = 3.5, SD = 1.5), t(256) = 9.89, p < .001, Cohen’s d = 1.41.
Descriptive statistics and inter-correlations
As presented in , for the human health practitioners, distress evoked did not correlate significantly with willingness to offer assisted dying services or with perceived norms, p = .490 and p = .258, respectively. However, norms had a positive correlation with willingness. Participants exposed to the normative scenario had a significantly higher willingness to offer assisted dying services than the participants exposed to the non-normative scenario, p <.001.
Table 3. Descriptive statistics and inter-correlations in Study 2.
The effects of norms, willingness, and their interaction on distress
Moderated multiple regression was conducted to examine the associations between manipulated norms, willingness to provide assisted dying services in the scenario, and psychological distress. Willingness to provide assisted dying service was mean-centered, and the interaction variable was created from the result of multiplication of the mean-centered score and manipulated norms.
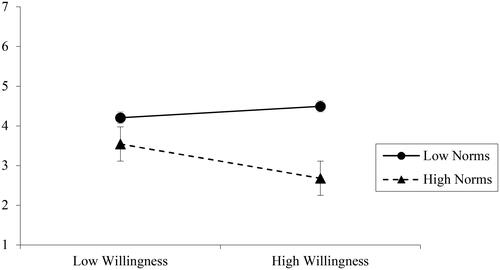
As presented in , when the direct effects were considered in Block 1, less than 1% of the distress variance was explained, Fch(2, 255) = 1.57, p = .210. In Block 2, however, there was a significant interaction effect of norms and willingness on distress over and above the direct effects in Block 1, Fch(1, 254) = 6.92, p = .009, R2ch = .03. More specifically, the interaction variable had a significantly negative association with psychological distress, 𝛽 = −.16, p = .009, CI = [−0.29, −0.04].
Table 4. Moderated multiple regression analyses for distress in Study 2.
To follow-up the significant interaction effect on distress, simple slope analyses were conducted to examine the association between willingness and distress in the normative and non-normative conditions. As presented in , in the non-normative condition, there was no significant association of willingness to participate in providing assisted dying services with distress, 𝛽 = .08, p = .494, CI = [-0.11, 0.22]: distress was uniformly high. However, in the normative condition, a higher willingness to provide assisted dying services was negatively associated with lower distress, 𝛽 = −.31, p = .004, 95%CI = [−0.47, −0.09], sr2 = .03. In the normative condition, participants who were more willing to provide such services had lower levels of distress.
Figure 2. Simple slopes analysis of the significant interaction effect of willingness to participate in providing assisted dying services and norms on distress level in Study 2.
The indirect effect of manipulated norms on distress
A second analysis was then conducted to replicate the test of the indirect effect observed in Study 2. We found that the normative condition positively predicted willingness, 𝛽 = .45, p <.001, CI [0.59, 0.96], but willingness did not significantly predict distress, 𝛽 = −.09, p =.176, CI [-0.21, 0.04]. Further analysis showed a non-significant direct effect of norms on distress as reported above, 𝛽 = .11, p =.256, CI [-0.08, 0.30], and also confirmed that the indirect effect via willingness was not significant, standardized IE = −.07, CI [−0.16, 0.03].
Discussion
In the human context, when exposed to a scenario of non-normative assisted dying services, practitioner distress was uniformly high. In addition, the negative association of willingness with psychological distress was only found when the assisted dying services were conducted in a normative context. The role of social norms in Study 2 is consistent with previous research showing that the norms can strengthen the influence of personal attitudes upon actors’ mental health (Vlasceanu & Coman, Citation2022). The two studies together provide an understanding of how different contexts shape the psychological implications of engagement in assisted dying services amongst practitioners.
General discussion
The current work provides new knowledge on the ongoing debate about the mental health implications of assisted dying services on practitioners. There are many prominent sources of psychological distress amongst community members and health practitioners when they contemplate requests for assisted dying. Previous research has suggested that practitioners’ psychological distress is associated with lower willingness (Curry et al., Citation2000). These findings are supported by the results of Study 1. In addition, supportive professional norms also reduce psychological distress (Study 1), consistent with the broader literature (Amiot et al., Citation2013, Citation2020).
The findings are also consistent with previous research in showing that psychological distress can arise when individuals have favorable attitudes toward assisted dying services, but that normative support is missing (Moore & Lucas, Citation2021). This finding reinforces themes arising in qualitative research among practitioners, highlighting that distressing factors may not only be associated with the presence of the service itself, but also with a lack of environmental, collegial, and organizational support (or ambiguity and conflict), so that the service cannot be properly decided and delivered (Beuthin et al., Citation2018). The patterns in ., negative associations of willingness to provide assisted dying services with psychological distress when there are supportive norms) are also consistent with qualitative research highlighting that exposure to assisted dying situations can be associated with distress among practitioners who are opposed to the practice (Bellens et al., Citation2020). In this sense, introducing assisted dying services when these are still widely opposed by practitioners and norms are not seen as supportive, might be associated with the psychological distress outcomes for practitioners.
The legalization of assisted dying services has in fact not been consistently associated with deference to health practitioner norms, which are sometimes persistently oppositional, and yet over-ridden by politicians at the behest of communities (Inghelbrecht et al., Citation2009). The possibility that other referent group norms are influential in the health context for human patients is one explanation for the lack of an association between willingness to offer the services and manipulated norms in Study 2. Future research examining health practitioners’ willingness should consider norms from other referent groups (such as religious or political groups) and the role that these alternative norms play in shaping practitioners’ attitudes and psychological distress.
Turning to the applied implications of these findings, it should be noted that those who personally support assisted dying services may choose to limit their involvement in the absence of perceived adequate legal and practice supports (Pesut et al., 2020; Citation2020). However, the lack of normative support for assisted dying itself may be distressing for those practitioners. Alternatively, for those who find themselves in contexts when they oppose assisted dying services, and it is normative, considerable psychological distress may be reported. The changing norms across contexts may also be associated with more variability in distress than the power of norms within a single context, where norms may operate to homogenize the variance as much as change the level of the means (Louis et al., Citation2003).
It should be noted that transient experiences of emotional distress may be an adaptive response to particular situations and stressors without lasting implications for mental health. In contrast, in the current research we have framed practitioners’ psychological distress as potentially lasting and generalized (Trankle, Citation2014), and as such we understand it to be an indicator of occupational risk for ill-being. Longitudinal research with health practitioners would be of value to test this association empirically in relation to their well-being. Two differences between the experiments would benefit from closer examination—one is that in Study 1, the subject of assisted dying is an animal and in Study 2, it is a human; the other is that the veterinarian participants in Study 1 may already have had first-hand experience with assisted dying for an animal, while it is unlikely that the health students had such experience. The attitudes of practitioners may change significantly as they gain experience, and for different targets. In future, comparative longitudinal research that follows practitioners’ norm perceptions for various reference groups, alongside their willingness to offer assisted dying services, and their personal experiences of distress and mental illness, would be of great value in illuminating these connections.
Another applied implication is that, taken at face value, attempts to reduce distress related to the decision and delivery of assisted dying services could focus on norms-based interventions. Qualitative research to explore the mechanism, and consideration of the normative context across a range of references, including the organization itself, could therefore also be important in organizations’ provision of employee guidance and support programs.
The present research is strengthened by a survey experimental design that worked through random assignment. This consistent experimental design is particularly important given that different patterns of associations are reported (at least concerning the direct role of normative support upon distress). Future research should take advantage of random experimental paradigms to explore within- and between-person effects more deeply, and in particular, to examine changing perceptions of norms, willingness, and distress over time (e.g., comparing contexts in which legalization has occurred with contexts in which it has not).
Longitudinal research capturing practitioners’ real services provision would also address another limitation in the present research. The use of scenarios allowed for more experimental control, but responses to scenarios may not mirror practitioners’ actual experiences of psychological distress. As noted above, in Study 1, it is probably the case that the practicing veterinarians had direct exposure to animal euthanasia in Australia, whereas the health practitioner students in Study 2 did not. However, it should be noted that many or all of our human health practitioner student participants may be expected to encounter assisted dying services, as they are increasingly widely offered and debated. As noted above, as the practices are normalized (or rolled back) over time, it may also be valuable to consider longitudinal research to explore norm changes in relation to distress as practitioners engage in the workforce. Considering the findings that supportive norms could reduce psychological distress in Study 1, future research should seek to replicate the experimental designs of the studies by considering contexts in which (for example) suffering is presented without an opportunity being given for assisted dying services to be offered, so that a baseline control condition is explicitly part of the design.
Future comparative work could be conducted to examine this hypothesis directly, examining contexts in which assisted dying services were legalized with more or less practitioners’ support. Overall, the broader point is that social norms about assisted dying services matter in determining how health practitioners feel about those services. Further, it is clear that oppositional norms and unfavorable attitudes create potential risk for distress, and possibly for future mental health outcomes such as have been observed for veterinarians in relation to euthanasia (Dalum et al., Citation2024; Stoeven, Citation2015; Witte et al., Citation2019).
In both studies, an additional limitation that must be acknowledged pertains to the measurement and manipulation of norms from only one referent group (i.e., practitioners’ professional group). Because social norms are defined as group standards of behavior, the specific reference groups that define the norm are important to individuals’ motivations to act (Amiot et al., Citation2020; Terry & Hogg, Citation1996). In the context of assisted-death services, it may be presumed that the voices of physicians and other practitioners involved will determine how the public will develop attitudes toward the practices. In the present study, willingness to engage in the service was indeed associated strongly with perceived normative support from practitioners (i.e., doctors and veterinarians). However, there are other possible referents, such as political and religious authorities, who may put forward views on assisted dying services. Interactions might be expected such that when participants do not base their attitudes and willingness on religious positions, professional norms might play a stronger role.
Considering the applied importance of this context, we encourage future scholars to seek to replicate these findings longitudinally in health practitioners’ context and with community samples for whom the issue is personally relevant, and in so doing to make a stronger contribution to the study of how social norms shape the mental health implications of particular attitudes and behaviors.
Supplemental Material
Download MS Word (15.2 KB)Disclosure statement
The authors declare no competing financial interests or personal relationships that could have influenced the work reported in this article.
Additional information
Funding
Notes
1 The research was conducted as part of a larger longitudinal study of euthanasia attitudes, perceived norms, and distress. At Time 2, a field experiment was conducted, which is the study reported in the present paper. Copies of the full longitudinal questionnaires are available from the corresponding author on request. The results of the longitudinal survey of veterinarians are presented in (Crane et al., Citation2023).
References
- Amiot, C. E., Lizzio-Wilson, M., Thomas, E. F., & Louis, W. R. (2020). Bringing together humanistic and intergroup perspectives to build a model of internalisation of normative social harmdoing. European Journal of Social Psychology, 50(3), 485–504. https://doi.org/10.1002/ejsp.2659
- Amiot, C. E., Sansfaçon, S., & Louis, W. R. (2013). Uncovering hockey fans’ motivations behind their derogatory behaviors and how these motives predict psychological well-being and quality of social identity. Psychology of Sport and Exercise, 14(3), 379–388. https://doi.org/10.1016/j.psychsport.2012.12.004
- Andriessen, K., Krysinska, K., Dransart, D. A., Dargis, L., & Mishara, B. L. (2020). Grief after euthanasia and physician-assisted suicide. Crisis, 41(4), 255–272. https://doi.org/10.1027/0227-5910/a000630
- Arias-Ulloa, C. A., Gómez-Salgado, J., Escobar-Segovia, K., García-Iglesias, J. J., Fagundo-Rivera, J., & Ruiz-Frutos, C. (2023). Psychological distress in healthcare workers during COVID-19 pandemic: A systematic review. Journal of Safety Research, 87, 297–312. https://doi.org/10.1016/j.jsr.2023.07.016
- Bellens, M., Debien, E., Claessens, F., Gastmans, C., & Dierckx de Casterlé, B. (2020). It is still intense and not unambiguous. Nurses’ experiences in the euthanasia care process 15 years after legalisation. Journal of Clinical Nursing, 29(3–4), 492–502. https://doi.org/10.1111/jocn.15110
- Beuthin, R., Bruce, A., & Scaia, M. (2018). Medical assistance in dying (MAiD): Canadian nurses’ experiences. Nursing Forum, 53(4), 511–520. https://doi.org/10.1111/nuf.12280
- Brenna, C. T. A. (2021). Regulating death: A brief history of medical assistance in dying. Indian Journal of Palliative Care, 27(3), 448–451. https://doi.org/10.25259/ijpc_426_20
- Brooks, L. (2019). Health care provider experiences of and perspectives on medical assistance in dying: A scoping review of qualitative studies. Canadian Journal on Aging = La Revue Canadienne du Vieillissement, 38(3), 384–396. https://doi.org/10.1017/S0714980818000600
- Cartwright, C. M., Williams, G. M., Parker, M. H., & Steinberg, M. A. (2006). Does being against euthanasia legislation equate to being anti-euthanasia? Internal Medicine Journal, 36(4), 256–259. https://doi.org/10.1111/j.1445-5994.2006.01053.x
- Cislaghi, B., & Heise, L. (2018). Using social norms theory for health promotion in low-income countries. Health Promotion International, 34(3), 616–623. https://doi.org/10.1093/heapro/day017
- Crane, M. F., Kho, M., Thomas, E. F., Decety, J., Molenberghs, P., Amiot, C. E., Lizzio-Wilson, M., Wibisono, S., Allan, F., & Louis, W. (2023). The moderating role of different forms of empathy on the association between performing animal euthanasia and career sustainability. Journal of Applied Social Psychology, 53(11), 1088–1107. https://doi.org/10.1111/jasp.13000
- Cuman, G., & Gastmans, C. (2017). Minors and euthanasia: A systematic review of argument-based ethics literature. European Journal of Pediatrics, 176(7), 837–847. https://doi.org/10.1007/s00431-017-2934-8
- Curry, L., Schwartz, H. I., Gruman, C., & Blank, K. (2000). Physicians’ voices on physician-assisted suicide: Looking beyond the numbers. Ethics & Behavior, 10(4), 337–361. https://doi.org/10.1207/S15327019EB1004_2
- Dalum, H. S., Tyssen, R., Moum, T., Thoresen, M., & Hem, E. (2024). Euthanasia of animals – association with veterinarians’ suicidal thoughts and attitudes towards assisted dying in humans: A nationwide cross-sectional survey (the NORVET study). BMC Psychiatry, 24(1), 2. https://doi.org/10.1186/s12888-023-05402-7
- Dempsey, R. C., McAlaney, J., & Bewick, B. M. (2018). A critical appraisal of the social norms approach as an interventional strategy for health-related behavior and attitude change. Frontiers in Psychology, 9(2180), 2180. https://doi.org/10.3389/fpsyg.2018.02180
- Georges, J. J., The, A. M., Onwuteaka-Philipsen, B. D., & van der Wal, G. (2008). Dealing with requests for euthanasia: A qualitative study investigating the experience of general practitioners. Journal of Medical Ethics, 34(3), 150–155. https://doi.org/10.1136/jme.2007.020909
- Głębocka, A. (2018). Psychological determinants of attitude toward euthanasia: A comparative study of female nurses and female nonmedical professionals. Advances in Experimental Medicine and Biology, 1096, 93–103. https://doi.org/10.1007/5584_2018_191
- Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford Press.
- Inghelbrecht, E., Bilsen, J., Mortier, F., & Deliens, L. (2009). Attitudes of nurses towards euthanasia and towards their role in euthanasia: A nationwide study in Flanders, Belgium. International Journal of Nursing Studies, 46(9), 1209–1218. https://doi.org/10.1016/j.ijnurstu.2009.02.009
- Keohane, A., & Richardson, N. (2018). Negotiating gender norms to support men in psychological distress. American Journal of Men’s Health, 12(1), 160–171. https://doi.org/10.1177/1557988317733093
- Lizzio-Wilson, M., Thomas, E. F., Louis, W. R., Crane, M. F., Kho, M., Molenberghs, P., Wibisono, S., Minto, K., Amiot, C. E., Decety, J., Breen, L. J., Noonan, K., Forbat, L., & Allen, F. (2023). Using latent profile analysis to understand health practitioners’ attitudes toward voluntary assisted dying. Omega, 302228221149453. https://doi.org/10.1177/00302228221149453
- Lokker, M. E., Swart, S. J., Rietjens, J. A. C., van Zuylen, L., Perez, R., & van der Heide, A. (2018). Palliative sedation and moral distress: A qualitative study of nurses. Applied Nursing Research: ANR, 40, 157–161. https://doi.org/10.1016/j.apnr.2018.02.002
- Louis, W. R., Mavor, K. I., & Terry, D. J. (2003). Reflections on the statistical analysis of personality and norms in war, peace, and prejudice: Are deviant minorities the problem? Analyses of Social Issues and Public Policy, 3(1), 189–198. https://doi.org/10.1111/j.1530-2415.2003.00025.x
- Meeussen, K., Van den Block, L., Bossuyt, N., Echteld, M., Bilsen, J., & Deliens, L. (2011). Dealing with requests for euthanasia: Interview study among general practitioners in Belgium. Journal of Pain and Symptom Management, 41(6), 1060–1072. https://doi.org/10.1016/j.jpainsymman.2010.09.020
- Moore, K. A., & Lucas, J. J. (2021). COVID-19 distress and worries: The role of attitudes, social support, and positive coping during social isolation. Psychology and Psychotherapy, 94(2), 365–370. https://doi.org/10.1111/papt.12308
- Pesut, B., Thorne, S., Schiller, C. J., Greig, M., & Roussel, J. (2020). The rocks and hard places of MAiD: A qualitative study of nursing practice in the context of legislated assisted death. BMC Nursing, 19(1), 12. https://doi.org/10.1186/s12912-020-0404-5
- Pesut, B., Thorne, S., Storch, J., Chambaere, K., Greig, M., & Burgess, M. (2020). Riding an elephant: A qualitative study of nurses’ moral journeys in the context of Medical Assistance in Dying (MAiD). Journal of Clinical Nursing, 29(19-20), 3870–3881. https://doi.org/10.1111/jocn.15427
- Piers, R. D., van den Eynde, M., Steeman, E., Vlerick, P., Benoit, D. D., & van Den Noortgate, N. J. (2012). End-of-life care of the geriatric patient and nurses’ moral distress. Journal of the American Medical Directors Association, 13(1), 80.e7–80.13. https://doi.org/10.1016/j.jamda.2010.12.014
- Range, L. M., & Rotherham, A. L. (2010). Moral distress among nursing and non-nursing students. Nursing Ethics, 17(2), 225–232. https://doi.org/10.1177/0969733009352071
- Rice, E. M., Rady, M. Y., Hamrick, A., Verheijde, J. L., & Pendergast, D. K. (2008). Determinants of moral distress in medical and surgical nurses at an adult acute tertiary care hospital. Journal of Nursing Management, 16(3), 360–373. https://doi.org/10.1111/j.1365-2834.2007.00798.x
- Rietjens, J. A., Voorhees, J. R., van der Heide, A., & Drickamer, M. A. (2014). Approaches to suffering at the end of life: The use of sedation in the USA and Netherlands. Journal of Medical Ethics, 40(4), 235–240. https://doi.org/10.1136/medethics-2012-100561
- Smith, J. R., & Louis, W. R. (2008). Do as we say and as we do: The interplay of descriptive and injunctive group norms in the attitude-behaviour relationship. The British Journal of Social Psychology, 47(Pt 4), 647–666. https://doi.org/10.1348/014466607x269748
- Stevens, K. R.Jr (2006). Emotional and psychological effects of physician-assisted suicide and euthanasia on participating physicians. Issues in Law and Medicine, 21(3), 187–200.
- Stoeven, D. L. (2015). Suicide in veterinary medicine: Let’s talk about it. The Canadian Veterinary Journal, 56(1), 89–92.
- Stolz, E., Burkert, N., Großschädl, F., Rásky, É., Stronegger, W. J., & Freidl, W. (2015). Determinants of public attitudes towards euthanasia in adults and physician-assisted death in neonates in Austria: A national survey. PloS One, 10(4), e0124320. https://doi.org/10.1371/journal.pone.0124320
- Terry, D. J., & Hogg, M. A. (1996). Group norms and the attitude-behavior relationship: A role for group identification. Personality and Social Psychology Bulletin, 22(8), 776–793. https://doi.org/10.1177/0146167296228002
- Terry, D. J., Hogg, M. A., & White, K. M. (1999). The theory of planned behaviour: Self-identity, social identity and group norms. The British Journal of Social Psychology, 38 (Pt 3)(3), 225–244. https://doi.org/10.1348/014466699164149
- Trankle, S. A. (2014). Decisions that hasten death: Double effect and the experiences of physicians in Australia. BMC Medical Ethics, 15(1), 26. https://doi.org/10.1186/1472-6939-15-26
- Verhofstadt, M., Audenaert, K., Van den Broeck, K., Deliens, L., Mortier, F., Titeca, K., Pardon, K., & Chambaere, K. (2020). Belgian psychiatrists’ attitudes towards, and readiness to engage in, euthanasia assessment procedures with adults with psychiatric conditions: A survey. BMC Psychiatry, 20(1), 374. https://doi.org/10.1186/s12888-020-02775-x
- Vlasceanu, M., & Coman, A. (2022). The impact of social norms on health-related belief update. Applied Psychology. Health and Well-Being, 14(2), 453–464. https://doi.org/10.1111/aphw.12313
- Wibisono, S., Minto, K., Lizzio-Wilson, M., Thomas, E. F., Crane, M., Molenberghs, P., Kho, M., Amiot, C. E., Decety, J., Breen, L. J., Noonan, K., Forbat, L., & Louis, W. (2022). Attitudes toward and experience with assisted-death services and psychological implications for health practitioners: A narrative systematic review. Omega, 302228221138997. https://doi.org/10.1177/00302228221138997
- Witte, T. K., Spitzer, E. G., Edwards, N., Fowler, K. A., & Nett, R. J. (2019). Suicides and deaths of undetermined intent among veterinary professionals from 2003 through 2014. Journal of the American Veterinary Medical Association, 255(5), 595–608. https://doi.org/10.2460/javma.255.5.595
