
Abstract
Objective: To examine whether individual differences in Type D personality (combination of negative affectivity (NA) and social inhibition (SI)) could explain heterogeneity in perceived social support and relationship adjustment (intimate partner relationship) among people living with diabetes.
Design: In the Diabetes MILES—The Netherlands survey, 621 adults with type 1 or type 2 diabetes (54% female, age: 56 ± 14 years) completed measures of Type D personality (DS14), perceived social support and relationship adjustment. We used established DS14 cut-off scores to indicate Type D personality, high NA only, high SI only and reference groups.
Results: Participants from the Type D and NA only groups perceived lower levels of social support (Welch[3,259] = 37.27, p < 0.001), and relationship adjustment (Welch[3,191] = 14.74; p < 0.01) than those from the SI only and reference groups. Type D was associated with lower social support (lowest quartile; adjusted OR = 8.73; 95%CI = 5.05 ∼ 15.09; p < 0.001) and lower relationship adjustment (lowest quartile; adjusted OR = 3.70; 95%CI = 2.10 ∼ 6.53; p < 0.001). Type D was also associated with increased levels of loneliness.
Conclusion: Participants with Type D and participants with high NA only tend to experience less social support and less relationship adjustment. Type D personality was also associated with more loneliness. Experiencing lower social support and relationship adjustment may complicate coping and self-management in people with diabetes.
Introduction
Most people need other people to live happy lives. Social support helps people cope with stressors and maintain or improve well being (Siedlecki, Salthouse, Oishi, & Jeswani, Citation2014; Wethington & Kessler, Citation1986). People with diabetes have to live with a chronic condition that they have to manage 24 hours per day. Adequate self-management with oral medication and/or insulin therapy is needed to avoid short term complications (hypoglycemia, of severe hyperglycemia) and long term micro- and macro-vascular complications. Self-care can be complex, as glucose excursions can be unpredictable. It may be easier to cope with these serious stressors when receiving social support (Baek, Tanenbaum, & Gonzalez, Citation2014; Gao et al., Citation2013). Moreover, research has shown that social support can increase the quality of self-management in people with diabetes (Schi⊘tz, B⊘gelund, Almdal, Jensen, & Willaing, Citation2012; Searle, Norman, Thompson, & Vedhara, Citation2007; Van Dam et al., Citation2005). A special and important source of social support is the intimate partner. He or she may be a very important agent in the self-management of diabetes by taking part in or encouraging self-management of diabetes (Searle et al., Citation2007; Van Puffelen et al., Citation2014). From earlier research, we know that following diabetes medication treatment recommendations is greater among partnered people compared to people without a partner (Haines, Coppa, Harris, Wisnivesky, & Lin, Citation2018). Furthermore, better relationship adjustment is associated with better following of medication and diet recommendations (Pereira, Pedras, Ferreira, & Machado, Citation2017). On the other hand, in less adjusted relationships, partner support in self-management of diabetes may be perceived as controlling, and may therefore be interpreted negatively (Newton-John, Ventura, Mosely, Browne, & Speight, Citation2017; Tanaka, Trief, Scales, & Weinstock, Citation2017). Suboptimal support is also likely when partners are very worried about hypoglycemia (Nefs et al., Citation2016; Nefs & Pouwer, Citation2018). In a study of adults with cardiac conditions, the partners were even more anxious about the illness than the people with the condition, and this was associated with Type D personality (Pedersen, Van Domburg, Theuns, Jordaens, & Erdman, Citation2004); this could also be the case in partners of people with diabetes.
A recent meta-analysis, based on 28 studies involving 5242 participants, studied the association between social support and diabetes self-care. High heterogeneity was found in the strength of the associations for different subgroups of participants (Song, Nam, Park, Shin, & Ku, Citation2017). Although subgroup analyses were conducted, high heterogeneity could not be resolved for most subgroups, and therefore it remained unclear what caused the heterogeneity. For example, there was high heterogeneity with respect to diabetes type subgroups, which makes it hard to say if social support is more important for type 1 of type 2 diabetes. Type 1 diabetes requires intensive management 24 hours per day to prevent glucose excursions. Moreover, few people with type 1 diabetes know other people with type 1 diabetes (unless they are involved in peer support groups). These difficult aspects of type 1 diabetes could possibly be easier to overcome with good social support. Type 2 diabetes on the other hand, is usually diagnosed in later life, when people may live with a partner and a family. Developing a healthier lifestyle is a cornerstone in the management of type 2 diabetes, which makes at least some support from the partner necessary to be successful (Beverly, Wray, & Miller, Citation2008; Miller & Brown, Citation2005; Pereira, Pedras, & Machado, Citation2014).
One possible reason for the heterogeneity that was found in the Song et al. meta-analysis could be personality differences, because personality is associated with how people perceive and mobilise social support (Swickert, Hittner, & Foster, Citation2010). Moreover, people’s personality is an important factor in intimate partner relationships (Barelds & Barelds-Dijkstra, Citation2006). Type D personality is characterised by the combination of high negative affectivity (NA) and high social inhibition (SI). Individuals with Type D personality tend to experience negative emotions like anger, annoyance, gloom and worry (NA component), while they do not feel free to express themselves towards others (SI component). Research has indicated that people with Type D personality experience less social support compared to others (Bagherian Sararoudi, Sanei, & Baghbanian, Citation2011; Denollet et al., Citation1996, 2000; Ginting, Van de Ven, Becker, & Näring, Citation2016; Grande, Romppel, Michal, & Brähler, Citation2014; J. Li et al., 2016; Pedersen, Spindler, Erdman, & Denollet, Citation2009; Williams et al., Citation2008; Zohar, Denollet, Ari, & Cloninger, Citation2011). In people with diabetes, Type D has been associated with suboptimal health behaviors (Conti, Carrozzino, Patierno, Vitacolonna, & Fulcheri, Citation2016; X. Li, et al., 2016; Nefs et al., Citation2015) and with higher HbA1c (X. Li, et al., 2017; Shao, Yin, & Wan, Citation2017).
Little research has yet been conducted on Type D and social support in people with diabetes. Initial evidence suggests that Type D may be associated with experiencing less social support (Shao et al., Citation2017) and feeling more lonely (Nefs, Pouwer, Pop, & Denollet, Citation2012b) in people with type 2 diabetes. Furthermore, there has not been any research yet on Type D personality and relationship adjustment. Relationship adjustment or dyadic adjustment describes how well couples function together: the level of agreement they experience, the amount and enjoyableness of time spent together, and the amount of commitment to remain a couple (Spanier, Citation1989).
Loneliness can be viewed as the opposite of social support, as it is the emotional distress that comes with poor quality of social relationships (Hawkley & Cacioppo, Citation2010). It has been shown that loneliness is associated with the metabolic syndrome in middle aged and older adults (Whisman, Citation2010), and that loneliness may increase biological aging (Hawkley & Cacioppo, Citation2010). Although not much is known on the direct link of loneliness and diabetes, loneliness is an issue for people with Type D personality (Beutel et al., Citation2017; De Moor, Denollet, & Laceulle, Citation2018; Kunst & Van Bon-Martens, Citation2011).
The aim of this study was to test whether individual differences in Type D personality characteristics explain differences in perceived social support, relationship adjustment and loneliness among people living with diabetes. We hypothesise that SI is associated with less perceived social support, because we expect that when people are more likely to keep their feelings and emotions to themselves, they will also be less likely to get support from others. We also expect that high NA and SI may interfere with the capacity to maintain a well-adjusted relationship with an intimate partner, so we expected negative associations between Type D personality characteristics and relationship adjustment. Furthermore, we expect that the evaluation of social relationships may be colored by personality and therefore expect differences between subgroups in the amount of loneliness that is experienced at a predetermined level of social support.
Materials and methods
Participants
Participants were 621 Dutch adults with type 1 or type 2 diabetes who completed the Diabetes MILES (Management and Impact for Long-term Empowerment and Success)—The Netherlands online survey (Nefs, Bot, Browne, Speight, & Pouwer, Citation2012a). This is a national cross-sectional survey focusing on the psychological aspects of living with diabetes. The whole MILES-NL study included 3960 participants; however, the Multidimensional Scale of Perceived Social Support (MSPSS) and the Dyadic Adjustment Scale (DAS) for relationship adjustment were presented to a randomly selected subgroup of the MILES sample (Nefs et al., Citation2012a). The DAS was completed by participants with a partner, a total of 458 respondents, and analysis including relationship adjustment were done with 458 respondents.
The study protocol was approved by the Psychological Research Ethics Committee of Tilburg University. Digital informed consent was obtained from all participants.
Type D personality traits
The DS14 is a 14-item scale assessing NA, SI, and Type D personality (Denollet, Citation2005). Items are rated on a five-point Likert scale, ranging from false to true. The NA and SI scales can be scored continuously. Both subscales range from 0 to 28 and scores of 10 or higher on both scales indicate Type D personality. The subscales are internally consistent with Cronbach’s alphas of 0.88 for negative affect and 0.86 for SI (Denollet, Citation2005). The two factor model of the DS14 was confirmed and adequate internal consistency, temporal stability and homogeneity has been shown in people with diabetes (Nefs et al., Citation2012b). Type D is assessed dichotomously or alternatively four groups are created based on DS14 scores: Type D personality as defined by the cut off of ≥10 (Denollet, Citation2005) on both the SI scale and the NA scale, a group with only NA ≥10 (NA + SI–), a group with only SI ≥10 (NA–SI+), and a group with both NA and SI scores ≤9 (NA–SI–).
Perceived social support
The MSPSS (Zimet, Dahlem, Zimet, & Farley, Citation1988) is a 12-item scale assessing subjective perceptions of social support. There are three subscales, concerning social support from family, friends and significant other. Answers are rated on a seven point Likert scale ranging from 1 ‘Very strongly disagree’ to 7 ‘Very strongly agree’. Total score ranges from 12 to 84; higher scores indicate more social support. Psychometric properties of the MSPSS are sound, and Cronbach’s alpha values between 0.85 and 0.91 (Canty-Mitchell and Zimet, 2000; Clara, Cox, Enns, Murray, & Torgrude, Citation2003; Zimet et al., Citation1988). The MSPSS was also validated in a Dutch study, confirming these findings (Pedersen et al., Citation2009).
Relationship adjustment
The DAS (Spanier, Citation1989) was used to assess relationship adjustment. It is a 32-item questionnaire measuring the quality of adjustment in couples, either married or living together, consisting of four empirically verified components: dyadic satisfaction, dyadic consensus, dyadic cohesion and affectional expression. The DAS has a range of 0 to 151, with higher scores indicating more relationship adjustment. The questionnaire was found to be reliable (α = 0.80) and valid (Montesino, Gómez, Fernández, & Rodríguez, Citation2013). A score of ≤97 is often used as a cutoff to identify distressed relationships (Eisenberg, Peluso, & Schindler, Citation2011). However, we examined the lowest quartile vs. the other three quartiles, using a cutoff of 111, because we were not primarily interested in distressed relationships per se, but in a much milder and more common form of maladjustment in relationships.
Loneliness
Loneliness was measured by a single item on which participants could indicate whether they were lonely (1 = never lonely; 10 = always lonely). We used a single item measure to elicit a global impression about the amount of loneliness people experienced and to reduce respondent burden. This single item was also used in a large earlier study (DiaDDZoB study, Nefs, Pouwer, Denollet, & Pop, Citation2010).
Statistical analyses
All analyses were conducted with IBM SPSS Statistics 22. Characteristics of the sample were expressed in means, standard deviations and percentages. We calculated characteristics for the total sample for this study, but also for the four groups based on DS14 scores: Type D personality as defined by the cut off of ≥10 (Denollet, Citation2005) on both the SI scale and the NA scale, a group with only NA ≥10 (NA + SI–), a group with only SI ≥10 (NA–SI+), and a group with both NA and SI scores ≤9 (NA–SI–).
In order to study the unique and shared correlates of NA and SI, we used both continuous scores of NA and SI, and cut off scores to indicate Type D personality, high NA only, high SI only and a reference group. With the continuous scores of NA and SI, we calculated correlations. Because the assumption of equality of variances was violated, we conducted Welch analyses of variances (ANOVA), which are robust for this violation of ANOVA assumptions, with Games-Howel post-hoc tests. Furthermore, we also conducted logistic regression analyses with the lowest quartile (vs. the other three quartiles) of social support scores and the lowest quartile (vs. the other three quartiles) of relationship adjustment scores as the outcome variables and the four personality groups, sex, age, educational level and type of diabetes as predictors. In order to examine the predictors within the continuous approach to Type D personality, we Z transformed the NA and SI scales and constructed an interaction term. We included these three together with sex, age, educational level and type of diabetes, in logistic regression analyses with the lowest quartile (vs. the other three quartiles) of social support scores and the lowest quartile (vs. the other three quartiles) of relationship adjustment scores as the outcome variables. To prevent overfitting, we used the rule of thumb of at least 15 participants per predictor (Field, Citation2009). With 621 participants, we could have included 41 predictors, but we included only seven.
Post-hoc, by multivariable logistic regression analysis, we examined the prevalence of Type D among people who were simultaneously in the lowest quartiles of both social support and relationship adjustment. For exploratory purposes, by means of Welch ANOVA and Games-Howel post-hoc tests, we tested whether people with lower social support and Type D were more lonely compared with people with more support and no Type D, people with lower support but no Type D, and people with Type D but more support.
Results
Sample characteristics
The total sample consisted of 621 adults with type 1 or 2 diabetes (60% type 2). The mean age was 56 ± 14, 53% were female, 40% completed higher education, and 21% were single (). A total of 27% of participants had Type D personality, 17% had high NA only and 16% had high SI only. We found that participants with a Type D personality were younger (which resulted in less respondents being over 65, the retirement age in the Netherlands, compared to the other personality groups), had a paid job more often, were more often female, less educated, more often single, and had higher BMIs compared with the three other groups (All significant at p < 0.05.). Although Type D individuals were significantly younger, their diabetes durations were similar to the other groups, indicating that on average, they were younger when their diabetes was diagnosed.
Table 1. Demographic and clinical characteristics of participants for total sample and by personality subgroup.
Only participants with a partner were asked to complete the questionnaire about relationship adjustment. We performed additional analyses examining the group (N = 129) who could not fill out the relationship adjustment scale compared to those who did (N = 458). This showed that people without a partner had a significantly shorter diabetes duration (F = 3.64, df = 618, p = 0.04), were more often female (Χ2 = 3.21, df = 1, p = 0.08), and more often had Type D personality (Χ2 = 6.11, df = 1, p = 0.02).
Furthermore, we compared people with type 1 diabetes to people with type 2 diabetes. We found that people with type 1 diabetes were significantly younger (F = 25.85, df = 422, p < 0.01), had significantly lower BMI (F = 19.10, df = 608, p < 0.01), were living with diabetes significantly longer (F = 140.54, df = 347, p < 0.01), were more often female (Χ2 = 4.41, df = 1, p = 0.04), were more often highly educated (Χ2 = 12.96, df = 1, p < 0.01) and were in a paid job more often (Χ2 = 39.69, df = 1, p < 0.01). We did not find any significant differences for DAS total and subscale scores between type 1 and type 2 diabetes (p’s ranged from 0.30 to 0.84). Furthermore, we did not find significant differences between type 1 and type 2 diabetes on social support total scale and subscales (p’s ranged from 0.07 to 0.39).
Personality differences in social support
NA and SI were negatively correlated with perceived social support with r = –0.38 (p < 0.001) and r = –0.31 (p < 0.001) respectively. Correlations of NA and SI with the special person, family, and friends subscales of the MSPSS ranged between –0.21 and –0.38 (all p’s < 0.001).
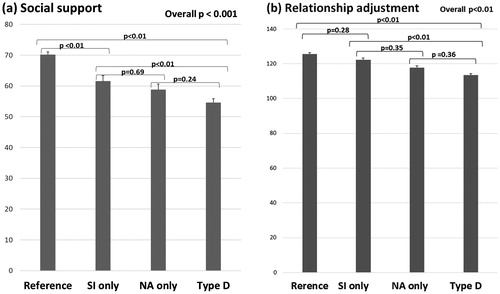
Regarding the total score on perceived social support, we found a significant difference between the four personality subgroups, Welch (3, 259) = 37.27, p < 0.001 (). We found significant personality differences regarding support from a special person (Welch [3, 258] = 16.99, p < 0.01), family support (Welch [3, 264] = 27.25, p < 0.01), and support from friends (Welch [3, 262] = 31.64, p < 0.01). Games-Howel post-hoc tests indicated that participants with Type D experienced significantly lower perceived social support compared with the reference and SI only groups, but not from the NA only group (). The SI only group and NA only group did not differ significantly from each other.
Figure 1. Social support and relationship adjustment levels for the four personality subgroups. SI: social inhibition; NA: negative affect.
Personality differences in relationship adjustment
We found significant negative correlations for NA and SI scores with relationship adjustment (r = –0.32; p < 0.01, and r = –0.22; p < 0.01, respectively). Correlations of NA and SI with the relationship adjustment subscales ‘dyadic satisfaction’, ‘dyadic consensus’, ‘dyadic cohesion’, and ‘affectional expression’ subscales ranged from –0.16 to –0.30 (all p’s < 0.001, data not shown).
When using the four personality subgroups, we found a significant difference between the four groups for the relationship adjustment total score, Welch (3, 191) = 14.74; p < 0.01. Games-Howel post-hoc tests showed that the Type D subgroup reported significantly lower relationship adjustment compared with the reference and SI only groups, but not significantly from the NA only subgroup (). The SI only and NA only subgroups did not differ significantly from each other.
We found significant personality differences regarding relationship adjustment subscales ‘dyadic satisfaction’ (Welch [3, 190] = 10.77, p < 0.01), ‘dyadic consensus’ (Welch [3, 192] = 12.33, p < 0.01), ‘dyadic cohesion’ (Welch [3, 198] = 7.12, p < 0.01), and ‘affectional expression’ (Welch [3, 190] = 9.22, p < 0.01). Games-Howel post-hoc tests showed that the Type D subgroup reported significantly lower ‘dyadic cohesion’ and ‘affectional expression’ scores compared to the three other groups. For ‘dyadic satisfaction’ and ‘dyadic consensus’ scores for participants with Type D and participants with high NA only did not differ significantly from each other; they did, however, differ significantly from participants with high SI only and the reference group (data not shown).
Lower social support and lower relationship adjustment
We defined the lowest quartile (≤52) of MSPSS scores as ‘lower social support’ and we constructed a multivariable logistic regression model that included the four personality groups, and based on our findings in , sex, age, educational level and type of diabetes (). Type D personality was independently associated with lower social support (OR = 8.73). NA only (OR = 3.73) and SI only (OR = 3.19) were also related to lower social support. Increasing age was associated with an increased odds of lower social support (OR = 1.03) (). For the interaction model, we found the Z transformed NA score to be a significant predictor (OR = 2.01), as were the Z transformed SI score (OR = 1.62) and age (OR = 1.03). We did not find a significant interaction effect for the Z transformed NA score * the Z transformed SI score.
Table 2. Multivariable logistic regression analyses of lower social support and lower relationship adjustment.
We defined the lowest quartile (≤111) of the relationship adjustment total score as ‘lower relationship adjustment’ and we conducted logistic regression analyses with the four personality groups, and based on our findings in , sex, age, educational level and type of diabetes as predictors (). We found that Type D personality significantly predicted lower relationship adjustment (OR = 3.70); for individuals from the high NA only subgroup we also found higher odds of experiencing lower relationship adjustment (OR = 2.51). For the interaction model, we found the Z transformed NA score to be the only significant predictor (OR = 1.72). We did not find a significant interaction effect for the Z transformed NA score * the Z transformed SI score.
Overall, 47 participants with a partner experienced both lower social support and lower relationship adjustment. In total 27 out of 110 (25%) of the participants with Type D personality had both lower social support and lower relationship adjustment, compared to 6% (20 out of 348) of the participants without Type D (Χ2 = 44.0; df = 2; p < 0.01).
Loneliness
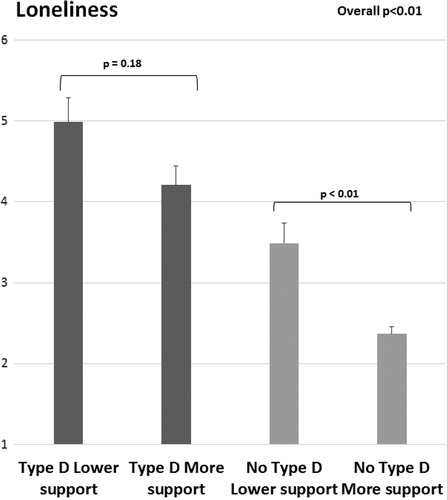
The level of loneliness of people with (a) both Type D personality and lower social support, (b) Type D and more support, (c) no Type D and lower social support and (d) no Type D and more support differed significantly; Welch (3, 161) = 38.20, p < 0.001. Games-Howell post-hoc tests indicated that participants with Type D had significantly higher loneliness levels compared with participants without Type D. However, participants with Type D with more social support did not have significantly lower loneliness levels compared with participants with Type D with lower social support. For people without Type D personality the amount of perceived social support was significantly related to their loneliness levels ().
Figure 2. Loneliness across personality types and social support levels. The range of the loneliness item is from 1 (never lonely) to 10 (always lonely).
Discussion
The aim of this study was to test whether individual differences in Type D personality characteristics could explain differences in perceived social support and relationship adjustment among people living with diabetes. We found that 27% of our sample had Type D personality. This is comparable to percentages found in other studies in other populations (Dulfer et al., Citation2015; Einvik et al., Citation2011; Grande et al., Citation2011; Pedersen, Van den Broek, Erdman, Jordaens, & Theuns, Citation2010). As expected, we found a negative correlation between SI and social support. The results of the analysis with the four personality subgroups indicated that participants with Type D perceived significantly lower social support levels compared with participants from the SI only and reference group, but not from the NA only group, so this relationship seems to be driven by NA. We found that participants with Type D had an 8-fold higher odds of lower social support as defined by the lowest quartile of social support scores. Individuals with high NA only and individuals with high SI only had 3-fold higher odds of experiencing lower social support. For the interaction model, we found NA to be a significant predictor for low social support, as were SI and age. We did not find a significant interaction effect for the Z transformed NA score * the Z transformed SI score, indicating that there is no statistical interaction between NA and SI; however, this is not what is expected of Type D. The effect of Type D must be larger than the effects of high NA only and high SI only (Denollet, Pedersen, Vrints, & Conraads, Citation2013; Denollet, Sys, & Brutsaert, Citation1995; Smith Citation2011), which is called biological interaction. Indeed, for low social support we found that the odds ratio for Type D was higher than the odds ratios for high NA only and high SI only.
Both the NA and SI dimensions of Type D were negatively correlated with relationship adjustment. Participants with Type D differed significantly in relationship adjustment scores from the SI only and reference group, but not from the NA only group, indicating that this relationship may be driven by NA. Type D individuals had an almost 4-fold higher odds of experiencing lower relationship adjustment as defined by the lowest quartile of relationship adjustment scores. Individuals with high NA only had a 2.5-fold higher odds of experiencing lower relationship adjustment. For the interaction model, we found NA to be the only significant predictor for low social support, which supports the hypothesis that negative affect plays an important role in this association.
Type D personality was also significantly associated with an increased risk of both lower social support and lower relationship adjustment. Furthermore, we found that participants with Type D were more often single, and that Type D personality was more prevalent among women as compared to men. Earlier research (Joensen, Almdal, & Willaing, Citation2013) found that people living without a partner needed extra social support to prevent poorer diabetes outcomes, and that women seemed to be more susceptible to worse diabetes self-management when living without a partner.
Finally, we found that participants with Type D experienced more loneliness compared to people without Type D. Type D participants with more social support experienced similar levels of loneliness compared to Type D participants with lower social support. However, for people without Type D the amount of perceived social support was related to their loneliness levels. This may indicate that people with Type D personality tend to feel lonelier, regardless of the amount of social support they experience. Maybe the quality of their relationships is worse, thereby not alleviating the feelings of loneliness.
The relationship of Type D personality with less social support has been researched before in many different populations. In the general population, it was found that people with Type D personality experienced lower levels of social support (Williams et al., Citation2008; Zohar et al., Citation2011). In a German general population-based sample, both NA and SI measures from the DS14 were negatively correlated with social support (Grande et al., Citation2014). Research in cardiovascular disease showed that people with coronary heart disease and Type D personality may experience a lack of social support (Denollet et al., Citation1996). Type D personality was associated with lower levels of social support in Danish and Dutch Type D participants with cardiac arrhythmias (Pedersen et al., Citation2009), Iranian myocardial infarction patients (Bagherian Sararoudi et al., Citation2011), and Indonesian patients with coronary heart disease (Ginting et al., Citation2016). Initial evidence in people with type 2 diabetes also suggested that individuals with Type D personality may also experience less social support (Nefs et al., 2012; Shao et al., Citation2017). Our study confirms these findings, and extends them to people with type 1 diabetes.
However, it still needs to be investigated if people with Type D actually receive less social support or that they rather perceive lower levels of support. A recent study (De Moor et al., Citation2018) also showed that participants with Type D felt less connected to others. Are efforts of Type D individuals to mobilise social support not met by their family, friends and significant others? Or do people with Type D make less of an effort to connect to the people around them (Denollet, Citation2000)? This could be part of a more general disposition towards passivity, as shown for example by a more sedentary lifestyle (Borkoles, Polman, & Levy, Citation2010; Einvik et al., Citation2011; Hausteiner, Klupsch, Emeny, Baumert, & Ladwig, Citation2010; Mommersteeg, Kupper, & Denollet, Citation2010), and lower health care use (Nefs et al., Citation2015; Pelle, Schiffer, Smith, Widdershoven, & Denollet, Citation2010; Schiffer, Denollet, Widdershoven, Hendriks, & Smith, Citation2007). On the other hand, a recent study (Lambertus et al., Citation2018) found that Type D personality among depressed CHD patients is associated with more complex and enduring mental disorders, such as avoidant personality disorder. If this association is present in other populations as well, this might also be associated with making less connection with other people.
Social support is of great importance for people with diabetes, and even more so for Type D individuals with diabetes. Nefs et al. (Citation2015) already showed after analyses of data from the Diabetes MILES sample that Type D individuals were less likely to follow a healthy diet or to consult healthcare professionals in case of problems with diabetes management, and more likely to experience diabetes-specific social anxiety, barriers regarding medication use and symptoms of depression and anxiety. Low perceived social support may further add to the adverse health effects of emotional distress in people with diabetes. While social support can increase self-management of diabetes (Schi⊘tz et al., Citation2012; Searle et al., Citation2007; Van Dam et al., Citation2005), the lack of perceived support could be associated with worse self-management of diabetes. Our findings indicate that participants with Type D and participants with high NA only tend to experience less social support as well as less relationship adjustment. As far as we know, the relationship of Type D with relationship adjustment or other measures of intimate partner relationship quality has not been studied yet.
Strengths of this study include the large sample size, the use of psychometrically sound scales, and the statistical approach based on both continuous and dichotomous measures of perceived social support and relationship adjustment and Type D. Furthermore, the 4-group personality classification allowed us to study both the unique and shared correlates of NA and SI related to support and relationship adjustment. Limitations of the study are the cross-sectional design and the fact that we only measured perceived social support and not actual received social support, though it has been noted elsewhere that subjective perceptions can be more influential than objective measures (Lakey & Bennett Cassady, Citation1990).
In sum, the findings of the current study clearly indicate that Type D and high NA only are associated with the tendency to perceive less support and experience less relationship adjustment. Furthermore, Type D personality is associated with feelings of loneliness in people living with diabetes. This may result in more difficulties in the self-management of diabetes, and less perceived social and partner support when coping with stress-related events. For people working in diabetes care, this is something to keep in mind: people with a Type D personality and people with high negative affect are more often on their own when coping with stress and difficulties in the self-management of diabetes. Therefore, they may need a little extra attention and encouragement from their professional caregivers.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Baek, R. N., Tanenbaum, M. L., & Gonzalez, J. S. (2014). Diabetes burden and diabetes distress: The buffering effect of social support. Annals of Behavioral Medicine, 48, 145–155. doi:10.1007/s12160-013-9585-4
- Bagherian Sararoudi, R., Sanei, H., & Baghbanian, A. (2011). The relationship between Type D personality and perceived social support in myocardial infarction patients. JRMS, 16, 627–633.
- Barelds, D. P. H., & Barelds-Dijkstra, P. (2006). Partner personality in distressed relationships. Clinical Psychology and Psychotherapy, 13, 392–396.
- Beutel, M. E., Klein, E. M., Brähler, E., Reiner, I., Jünger, C., Michal, … Tibubos, A. N. (2017). Loneliness in the general population: Prevalence, determinants and relations to mental health. BMC Psychiatry, 17, 97. doi:10.1186/s12888-017-1262-x
- Beverly, E., Wray, L. A., & Miller, C. K. (2008). Practice implications of what couples tell us about type 2 diabetes management. Diabetes Spectrum, 21, 39–45.
- Borkoles, E., Polman, R., & Levy, A. (2010). Type-D personality and body image in men: The role of exercise status. Body Image, 7, 39–45.
- Canty-Mitchell, J., & Zimet, G. D. (2000). Psychometric properties of the multidimensional scale of perceived social support in urban adolescents. American Journal of Community Psychology, 28, 391–400.
- Clara, P. I., Cox, B. J., Enns, M. W., Murray, L. T., & Torgrude, L. J. (2003). Confirmatory factor analysis of the multidimensional scale of perceived social support in clinically distressed and student samples. Journal of Personality Assessment, 81, 265–270.
- Conti, C., Carrozzino, D., Patierno, C., Vitacolonna, E., & Fulcheri, M. (2016). The clinical link between Type D personality and diabetes. Frontiers in Psychiatry, 7, 113. doi: 10.3389/fpsyt.2016.00113
- De Moor, E. L., Denollet, J., & Laceulle, O. M. (2018). Social inhibition, sense of belonging and vulnerability to internalizing problems. Journal of Affective Disorders, 225, 207–213.
- Denollet, J. (2000). Type D personality. A potential risk factor refined. Journal of Psychosomatic Research, 49, 255–266.
- Denollet, J. (2005). DS14: Standard assessment of negative affectivity, social inhibition, and Type D personality. Psychosomatic medicine, 67, 89–97.
- Denollet, J., Pedersen, S. S., Vrints, C. J., & Conraads V. M. (2013). Predictive value of social inhibition and negative affectivity for cardiovascular events and mortality in patients with coronary artery disease: The Type D personality construct. Psychosomatic Medicine, 75, 873–881.
- Denollet, J., Sys, S. U., & Brutsaert, D. L. (1995). Personality and mortality after myocardial infarction. Psychosomatic Medicine, 57, 582–591.
- Denollet, J., Sys, S. U., Stroobant, N., Rombouts, H., Gillebert, T. C., & Brutsaert, D. L. (1996). Personality as independent predictor of long-term mortality in patients with coronary heart disease. Lancet, 347, 417–421.
- Dulfer, K., Hazemeijer, B. A. F., Van Dijk, M. R., Van Geuns, R. J. M, Daemen, J., Van Domburg, R. T., & Utens, E. M. W. J. (2015). Prognostic value of type D personality for 10-year mortality and subjective health status in patients treated with percutaneous coronary intervention. Journal of Psychosomatic Research, 79, 214–221.
- Einvik, G., Dammen, T., Hrubos-Strøm, H., Namtvedt, S. K., Randby, A., Kristiansen, … Omland, T. (2011). Prevalence of cardiovascular risk factors and concentration of C-reactive protein in Type D personality persons without cardiovascular disease. European Journal of Cardiovascular Prevention & Rehabilitation, 18, 504–509.
- Eisenberg, S. D., Peluso, P. R., & Schindler, R. A. (2011). Impact of brief marriage and relationship education classes on dyadic adjustment. Retrieved from www.pairs.com
- Field, A. (2009). Discovering statistics using SPSS (3rd ed.). London: Sage Publications.
- Gao, J., Wang, J., Zheng, P., Haardörfer, R., Kegler, M. C., Zhu, Y., & Fu, H. (2013). Effects of self-care, self-efficacy, social support on glycemic control in adults with type 2 diabetes. BMC Family Practice, 14, 66.
- Ginting, H., Van de Ven, M., Becker, E., S., & Näring, G. (2016). Type D personality is associated with health behaviors and perceived social support in individuals with coronary heart disease. Journal of Health Psychology, 21, 727–737.
- Grande, G., Romppel, M., Michal, M., & Brähler, E. (2014). The Type D construct: Is social inhibition more than social fear? European Journal of Psychological Assessment, 30, 283–288.
- Grande, G., Romppel, M., Vesper, J., Schubmann, R., Gleasmer, H., & Herrmann-Lingen, C. (2011). Type D personality and all-cause mortality in cardiac patients–Data from a German cohort study. Psychosomatic Medicine, 73, 548–556.
- Haines, L., Coppa, N., Harris, Y., Wisnivesky, J. P., & Lin, J. J. (2018). The impact of partnership status on diabetes control and self-management behaviors. Health Education & Behavior, 1–4. doi:10.1177/1090198117752783.
- Hausteiner, C., Klupsch, D., Emeny, R., Baumert, J., & Ladwig, K. H. (2010). Clustering of negative affectivity and social inhibition in the community: Prevalence of Type D personality as a cardiovascular risk marker. Psychosomatic Medicine, 72, 163–171.
- Hawkley, L. C., & Cacioppo, J. T. (2010). Loneliness matters: A theoretical and empirical review. Annals of Behavioral Medicine, 40, 218–227. doi:10.1007/s12160-010-9210-8
- Joensen, L. E., Almdal, T. P., & Willaing, I. (2013). Type 1 diabetes and living without a partner: Psychological and social aspects, self-management behaviour, and glycaemic control. Diabetes Research and Clinical Practice, 101, 278–285.
- Kunst, M. J. J., & Van Bon-Martens, M. J. H. (2011). Examining the link between domestic violence victimization and loneliness in a Dutch community sample: A comparison between victims and nonvictims by Type D personality. Journal of Family Violence, 26, 403–410. doi:10.1007/s10896-011-9374-4
- Lakey, B., & Bennett Cassady, P. (1990). Cognitive processes in perceived social support. Journal of Personality and Social Psychology, 59, 337–343.
- Lambertus, F., Herrmann-Lingen, C., Fritzsche, K., Hamacher, S., Hellmich, M., Jünger, J., … Albus, C. (2018). Prevalence of mental disorders among depressed coronary patients with and without Type D personality. Results of the multi-center SPIRR-CAD trial. General Hospital Psychiatry, 50, 69–75.
- Li, X., Gao, M., Zhang, S., Xu, H., Zhou, H., Wang, X., … Tian, D. (2017). Medication adherence mediates the association between Type D personality and high HbA1c level in Chinese patients with Type 2 Diabetes mellitus: A six-month follow-up study. Journal of Diabetes Research, 2017, 1–10. https://doi.org/10.1155/2017/7589184
- Li, J., Wu, X., Lin, J., Zou, D., Yang, X., Cheng, S., & Guo, Q. (2016). Type D personality, illness perception, social support and quality of life in continuous ambulatory peritoneal dialysis patients. Psychology, Health & Medicine, 24, 1–9.
- Li, X., Zhang, S., Xu, H., Tang, X., Zhou, H., Yuan, J., … Zhang, W. (2016). Type D personality predicts poor medication adherence in Chinese patients with type 2 Diabetes mellitus: A six-month follow-up study. PLoS One, 11, e0146892.
- Miller, D., & Brown J. L. (2005). Marital interactions in the process of dietary change for type 2 diabetes. Journal of Nutrition Education and Behavior, 37, 226–234.
- Mommersteeg, P. M. C., Kupper, N., & Denollet, J. (2010). Type D personality is associated with increased metabolic syndrome prevalence and an unhealthy lifestyle in a cross-sectional Dutch community sample. BMC Public Health, 10, 714.
- Montesino, M. L., Gómez, J. L., Fernández, M. E., & Rodríguez, J. M. (2013). Psychometric properties of the dyadic adjustment scale (DAS) in a community sample of couples. Psicothema, 25, 536–541.
- Nefs, G., Bot, M., Browne, J. L., Speight, J., & Pouwer, F. (2012a). Diabetes MILES–The Netherlands: Rationale, design and sample characteristics of a national survey examining the psychosocial aspects of living with diabetes in Dutch adults. BMC Public Health, 12, 925.
- Nefs, G., & Pouwer, F. (2018). The role of hypoglycemia in the burden of living with diabetes among adults with diabetes and family members: Results from the DAWN2 study in The Netherlands. BMC Public Health, 18, 156. doi:10.1186/s12889-018-5064-y
- Nefs, G., Pouwer, F., Denollet, J., & Pop, V. (2010). Psychological risk factors of micro- and macrovascular outcomes in primary care patients with type 2 diabetes: Rationale and design of the DiaDDZoB Study. BMC Public Health, 10, 388. doi:10.1186/1471-2458-10-388.
- Nefs, G., Pouwer, F., Holt R., Skovlund S., Hermanns N., Nicolucci A., & Peyrot M. (2016). Correlates and outcomes of worries about hypoglycemia in family members of adults with diabetes: The second Diabetes Attitudes, Wishes and Needs (DAWN2) study. Journal of Psychosomatic Research, 89, 69–77. doi:10.1016/j.jpsychores.2016.07.017
- Nefs, G., Pouwer, F., Pop, V., & Denollet, J. (2012b). Type D (distressed) personality in primary care patients with type 2 diabetes: Validation and clinical correlates of the DS14 assessment. Journal of Psychosomatic Research, 72, 251–257.
- Nefs, G., Speight, J., Pouwer, F., Pop, V., Bot, M., & Denollet, J. (2015). Type D personality, suboptimal health behaviors and emotional distress in adults with diabetes: Results from Diabetes MILES–The Netherlands. Diabetes Research and Clinical Practice, 108, 94–105.
- Newton-John, T. R. O., Ventura, A. D., Mosely, K., Browne, J. L., & Speight, J. (2017). ‘Are you sure you’re going to have another one of those?’ A qualitative analysis of the social control and social support models in type 2 diabetes. Journal of Health Psychology, 22, 1819–1829.
- Pedersen, S. S., Spindler, H., Erdman, R., & Denollet, J. (2009). Poor perceived social support in implantable cardioverter defibrillator (ICD) patients and their partners: Cross-validation of the multidimensional scale of perceived social support. Psychosomatics, 50, 461–467.
- Pedersen, S. S., Van den Broek, K. C., Erdman, R. A. M., Jordaens, L., & Theuns, D. A. M. J. (2010). Pre-implantation implantable cardioverter defibrillator concerns and Type D personality increase the risk of mortality in patients with an implantable cardioverter defibrillator. Europace, 12, 1446–1452. doi:10.1093/europace/euq296
- Pedersen, S. S., Van Domburg, R. T., Theuns, D. A. M. J., Jordaens, L., & Erdman, R. A. M. (2004). Type D personality is associated with increased anxiety and depressive symptoms in patients with an implantable cardioverter defibrillator and their partners. Psychosomatic Medicine, 66, 714–719.
- Pelle, A. J., Schiffer, A. A., Smith, O. R., Widdershoven, & J. W., Denollet, J. (2010). Inadequate consultation behavior modulates the relationship between Type D personality and impaired health status in chronic heart failure. International Journal of Cardiology, 142, 65–71.
- Pereira, M. G., Pedras, S., Ferreira, G., & Machado, J. C. (2017). Family and couple variables regarding adherence in Type 2 diabetes patients in the initial stages of the disease. Journal of Marital and Family Therapy, doi:10.1111/jmft.12281.
- Pereira, M. G., Pedras, S., & Machado, J. C. (2014). Family variables as moderators between beliefs towards medicines and adherence to self-care behaviors and medication in type 2 diabetes. Families, Systems, & Health, 32, 198–206.
- Schiffer, A. A., Denollet, J., Widdershoven, J. W., Hendriks, E. H., & Smith, O. R. F. (2007). Failure to consult for symptoms of heart failure in patients with a type-D personality. Heart, 93, 814–818.
- Schiøtz, M. L., Bøgelund, M., Almdal, T., Jensen, & B. B., Willaing, I. (2012). Social support and self-management behaviour among patients with Type 2 diabetes. Diabetes Medicine, 29, 654–661.
- Searle, A., Norman, P., Thompson, R., & Vedhara, K. (2007). Illness representations among patients with type 2 diabetes and their partners: Relationships with self-management behaviors. Journal of Psychosomatic Research, 63, 75–184.
- Shao, Y., Yin, H., & Wan, C. (2017). Type D personality as a predictor of self-efficacy and social support in patients with type 2 diabetes mellitus. Neuropsychiatric Disease and Treatment, 13, 855–861.
- Siedlecki, K. L., Salthouse, T. A., Oishi, S., & Jeswani, S. (2014). The relationship between social support and subjective well-being across age. Social Indicators Research, 117, 561–576.
- Smith, T. W. (2011). Toward a more systematic, cumulative, and applicable science of personality and health: Lessons from Type D personality. Psychosomatic Medicine, 73, 528–532.
- Song, Y., Nam, S., Park, S., Shin, I. S., & Ku, B. J. (2017). The impact of social support on self-care of patients with diabetes: What is the effect of diabetes type? Systematic review and meta-analysis. Diabetes Educator, 43, 396–412. doi:10.1177/0145721717712457.
- Spanier, G. B. (1976). Measuring dyadic adjustment: New scales for assessing the quality of marriage and similar dyads. Journal of Marriage and the Family, 1, 15–28.
- Spanier, G. B. (1989). Manual for the dyadic adjustment scale. North Tonawanda, NY: Multi-Health Systems.
- Swickert, R. J., Hittner, J. B., & Foster, A. (2010). Big five traits interact to predict perceived social support. Personality and Individual Differences, 48, 736–741.
- Tanaka, R., Trief, P. M., Scales, K., & Weinstock, R. S. (2017). “Miscarried helping” in adults with type 2 diabetes: Helping for Health Inventory—Couples. Families, Systems, & Health, 35, 409–419.
- Van Dam, H. A., Van der Horst, F. G., Knoops, L., Ryckman, R. M., Crebolder, H. F., & Van den Borne, B. H. (2005). Social support in diabetes: A systematic review of controlled intervention studies. Patient Education and Counseling, 59, 1–12.
- Van Puffelen, A. L., Rijken, M., Heijmans, M. J. W. M., Nijpels, G., Rutten, G. E. H. M., & Schellevis, F. G. (2014). Living with diabetes: A group-based self-management support programme for T2DM patients in the early phases of illness and their partners, study protocol of a randomised controlled trial. BMC Health Services Research, 14, 144.
- Wethington, E., & Kessler, R. C. (1986). Perceived support, received support, and adjustment to stressful life events. Journal of Health and Social Behavior, 27, 78–89.
- Whisman, M. A. (2010). Loneliness and the metabolic syndrom in a population-based sample of middle-aged and older adults. Health Psychology, 29, 550–554.
- Williams, L., O’Connor, R. C., Howard, S., Hughes, B. M., Johnston, D. W., Hay, J. L., … O’Carroll, R. E. (2008). Type-D personality mechanisms of effect: The role of health-related behavior and social support. Journal of Psychosomatic Research, 64, 63–69.
- Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52, 30–41.
- Zohar, A. H., Denollet, J., Ari, L. L., & Cloninger, C. R. (2011). The psychometric properties of the DS14 in Hebrew and the prevalence of Type D personality in Israeli adults. European Journal of Psychological Assessment, 27, 274–281.