
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objective
To test the effect of autonomy-supportive message framing on people’s perceived autonomy-support while considering the individual need for autonomy as a moderator. Also, to test whether autonomy-supportive message frames – through increased perceived autonomy-support - lead to more self-determined motivation, and increased intention to quit smoking.
Design
An online 2(autonomy-supportive; controlling language) × 2(choice; no choice) between-subjects design with control condition (generic advice) with adult smokers intending to quit (N = 626).
Main outcome
Intention to quit smoking (Theory of Planned Behaviour).
Measures
Perceived autonomy-support (Virtual Climate Care Questionnaire), need for autonomy (Health Causality Orientations Scale), self-determined motivation (Treatment Self-Regulation Questionnaire), attitudes, social influence, self-efficacy (I-Change Model).
Results
Structural equation modelling revealed no significant effect of autonomy-supportive-message frames on perceived autonomy-support or self-determined motivation, neither did the need for autonomy moderate these effects. Self-determined motivation had a positive, significant effect on intention to quit, mediated by attitudes, social influence, and self-efficacy.
Conclusion
Although message frames did not affect perceived autonomy-support or self-determined motivation, higher self-determined motivation increased intention to quit via attitudes, social influence, and self-efficacy. Before drawing the conclusion that message framing has no effect, we recommend to replicate this study in a real-life setting with smokers more likely to read and process the message frames more attentively.
Introduction
Smoking tobacco remains the leading preventable cause of ill-health and premature death worldwide (Bergh et al., Citation2017; World Health Organisation, Citation2018). There is a critical need to support smokers to successfully quit smoking. Alongside effective face-to-face behavioural therapies for smoking cessation, such as therapist advice, the Internet provides behaviour change interventions that have the potential to be cost-effective, because of the Internet’s great reach and low costs (Taylor et al., Citation2017). Previous research has shown that smokers can especially benefit from online computer-tailored (CT) health communication interventions (Etter & Perneger, Citation2001; Lustria et al., Citation2013; et al., Citation2012). Online CT interventions customize the provided information to a person’s specific characteristics by means of computer software and therefore provide relevant information only, which increases message processing and the likelihood for behaviour change (De Vries & Brug, Citation1999; Hawkins et al., Citation2008; Kreuter & Wray, Citation2003; Noar et al., Citation2009). However, Lustria et al. (Citation2013) conclude in their meta-analysis that effect sizes of online CT health interventions remain small.
Previous research found that people might process health messages better and are ultimately motivated to perform advocated behaviours when the way a message is presented or framed is adapted to preferred communication styles (Legault, Citation2016; Resnicow et al., Citation2008, Citation2014; et al., Citation2015). It is known that individual differences exist in people’s desire to regulate their behaviour themselves (Deci & Ryan, Citation1985b, Citation2000; Legault, Citation2016; Ryan & Deci, Citation2000). That is, some people choose their way of how to obtain a certain goal, such as to quit smoking, themselves and having a self-determined motivational orientation or high need for autonomy, while others have a lower need for autonomy and rather prefer to hear from an expert how to best to quit smoking (Gagné & Deci, Citation2005; Hagger & Chatzisarantis, Citation2011). The need for autonomy is a person’s inherent desire to perceive freedom in actions and to have control over own behaviour (Deci & Ryan, Citation2000). Thus, the need for autonomy seems to determine people’s preference for a communication style in health (i.e. autonomy-supportive style or not). For instance, Resnicow et al. (Citation2008, Citation2014) found that the need for autonomy moderated effects of fruit and vegetable intake promotion messages and cancer screening promotion messages. That is, people with a preference for an autonomy-supportive communication style who received leaflets framed autonomy-supportively had higher intake of fruit and vegetables or cancer screening rates than those with an autonomous preference who received leaflets written in a controlling language style. Thus, people with a higher need for autonomy may develop a self-determined motivation and a strong intention to substantially change their health behaviour (e.g. to quit smoking), only when feeling supported in their autonomy (i.e. perceive autonomy-support by means of autonomy-supportively framed messages) (e.g. Deci & Ryan, Citation1985a, Citation1985b; Ryan & Deci, Citation2000; Williams et al., Citation1999; Citation2002). Evidence from other offline health (care) contexts (i.e. interpersonal communication) has shown that the need for autonomy can be satisfied through autonomy-supportive message framing (Ng et al., Citation2012). That is, providing choice and using non-pressuring or autonomy-supportive language (e.g. using “you could” and “you may”) as opposed to controlling language style (e.g. directive and pressuring tone of voice and using ‘must’, ‘should’ and no provision of choice) (Deci & Ryan, Citation2000; Markland et al., Citation2005; Su & Reeve, Citation2011; Williams et al., Citation1999). Previous studies found effects of autonomy-supportive messages and environments on perceived autonomy-support, motivation and behavioural performance. To illustrate, Williams et al. (Citation1999) found that adolescents experienced physician-delivered appeals as autonomy-supportive when the appeals emphasised the adolescent’s decision making power of whether to start or quit smoking, or not. Appeals that were in fact perceived as autonomy-supportive subsequently affected participants self-determined motivation to refrain from smoking. As another illustration, Moustaka and colleagues (2012) found that, among women, an autonomy-supportive exercise instructor (e.g. offering opportunities for choice and delivering a meaningful rational for exercises) led to significantly more perceived autonomy-support, self-determined motivation to exercise, and also more frequent exercise behaviour than a controlling exercise instruction style. In sum, there is evidence that (offline) interpersonal autonomy-supportive messages can be effective in terms of generating perceived autonomy-support. Online CT health interventions could also be more effective when the way a message is presented or framed is adapted in an autonomy-supportive manner according to someone’s preferred communication style with regards to the need for autonomy (Resnicow et al., Citation2008, Citation2014; Smit et al., Citation2015).
As far as we know, it has not been investigated yet whether autonomy-supportive message framing can increase people’s perceptions of autonomy-support in an online (CT) smoking cessation context. Previous studies on autonomy-supportive messages considered both message elements in combination (e.g. Kinnafick et al., Citation2014, Kinnafick et al., Citation2016; Moustaka et al., Citation2012; Williams et al., 2006), i.e. (1) the provision of choice and (2) the use of autonomy-supportive language. We, however, propose to study the effect of both message elements on perceived autonomy-support, separately as it is unknown which message frame element (choice or autonomy-supportive language or their combination) reflects the effective ingredient resulting in increased perceived autonomy-support. Therefore, we aim to test the effect of autonomy-supportive message framing on people’s perceived autonomy-support while considering the individual need for autonomy as a potential moderator of effects in an online CT smoking cessation intervention.
Intervention content and message framing: from autonomy-support to intention
According to self-determination theory (SDT; Ryan & Deci, Citation2000), self-determined motivation mostly comes from own values or interests, but can also come from activity’s that align with own values (e.g. to quit smoking, because it is personally valued and important for self-satisfaction), and the satisfaction of the need for autonomy is essential in the development of self-determined motivation (Deci & Ryan, Citation2000). Research has consistently revealed a significant positive effect of self-determined motivation on positive affect and improved well-being (Deci & Ryan, Citation2000), as well as on the implementation of desired health behaviours, such as smoking cessation (i.e. Ng et al., Citation2012; Williams et al., Citation2002; 2006). In this sense, intentions are more likely to be translated into actions when the motivation to perform the target behaviour is self-determined (Hagger & Chatzisarantis, Citation2009).
The content of many effective online (CT) health interventions, such as the smoking cessation intervention used for the present study (Smit et al., Citation2016), is often based on reflective health behaviour change theories, such as the Theory of Planned Behaviour (TPB; Ajzen, Citation1991) and the I-Change Model (de Vries et al., Citation2003). In these theories of planned behaviour, the most proximal predictor of behaviour, such as smoking cessation, is a person’s intention to perform this behaviour, in this case, to quit smoking. Furthermore, intention is most often assumed to mediate the effect of three belief-based perceptions concerning the target behaviour on the behaviour, namely: attitudes, social influence (e.g. subjective norms) and self-efficacy. When based on theories of planned behaviour, interventions usually offer feedback, tips and tricks relating to those perceptions, in order to strengthen attitudes (i.e. a person’s overall evaluation of whether the performance of smoking cessation, will lead to desirable outcomes), social influence (i.e. an individual’s expectation of whether significant others would approve of him or her quitting smoking), and self-efficacy (i.e. one’s relative perceived difficulty or ease of smoking cessation). While positive changes in these three beliefs are argued to lead to an increased intention to quit smoking, not every smoker who forms an intention to quit smoking will eventually quit (Sheeran & Webb, Citation2016). Previous research on intention suggest that intentions to perform a target behaviour will most likely get translated into actual behaviour when they are strong (Hagger & Chatzisarantis, Citation2009; Sheeran & Webb, Citation2016). The underlying mechanism is that by enhancing self-determined motivation, intentions are strengthened through the satisfaction of, for instance, the need for autonomy and a consequent perception of autonomy-support. This is, because self-determined beliefs about a target behaviour have been found to better predict intention than controlling beliefs that are based on, for example, social pressure (Joseph et al., Citation2016; Sheeran & Orbell, Citation2000). Moreover, in their meta- analysis, Hagger and Chatzisarantis (Citation2009) provided evidence for the predictive power of self-determined motivation on intention via attitudes, subjective norms and self-efficacy. Thus, by integrating autonomy-supportive message framing in content-tailored interventions, SDT components are combined with constructs from theories of planned behaviour. Therefore, a potential way to increase online CT health intervention effectiveness, such as for smoking cessation, is to frame messages according to individual’s need for autonomy.
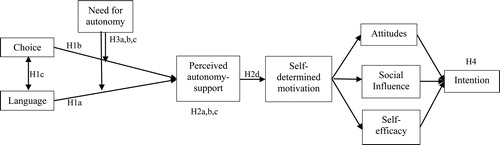
To the best of our knowledge, no study exists that has investigated whether satisfying the need for autonomy and enhancing perceived autonomy-support and self-determined motivation by means of autonomy-supportive message framing in an online CT smoking cessation intervention has the potential to increase intention to quit smoking and subsequently may enhance the effectiveness of such interventions. Therefore, the present study aims to investigate whether autonomy-supportive message frames – through an increased sense of autonomy-support – lead to more self-determined motivation, and subsequently to an increased intention to quit smoking. Yet, based on SDT and evidence from previous studies, we expect that both autonomy-supportive message elements, i.e. providing choice and autonomy-supportive language use, lead to higher levels of perceived autonomy-support. depicts the hypothetical model, based on SDT and theories of planned behaviour.
Figure 1. Hypothetical model.
Note. Simplified version of the hypothetical model used in the present study.
The following hypotheses will be tested:
H1: The use of autonomy-supportive language (H1a) and the provision of choice (H1b) will lead to higher levels of perceived autonomy-support than then the use of controlling language and no provision of choice. In addition, the combination of using autonomy-supportive language and the provision of choice will lead to higher levels of perceived autonomy-support than the use of autonomy-supportive language and the provision of choice alone (H1c).
H2: The use of autonomy-supportive language (H2a) and the provision of choice (H2b), and their combination even more so (H2c), will lead to higher levels of self-determined motivation than the use of controlling language and no provision of choice. This effect is mediated by perceived autonomy-support (H2d).
H3: The positive effect of autonomy-supportive language (H3a) and the provision of choice (H3b), as well as of their combination (H3c), on perceived autonomy-support is stronger for individuals with a high need for autonomy than for individuals with a low need for autonomy.
H4: Self-determined motivation leads to a higher intention to quit smoking through more positive attitudes, social influence and self-efficacy (H4).
Materials and methods
Design
A 2 (autonomy-supportive language vs. controlling language) × 2 (providing choice vs. not providing choice) between-subjects design with a control condition (generic advice) was employed.
Intervention
The online CT smoking cessation programme was based on a previously developed effective and cost-effective intervention (Smit et al., Citation2012; Citation2013) and grounded in the I-Change Model (de Vries et al., Citation2003). The I-Change Model seeks to explain motivational and behavioural change and includes theoretical concepts from different socio-cognitive theories, such as the TPB (Ajzen, Citation1991). In the I-Change Model, it is assumed that a person’s intention is regulated by motivation, attitudes, social influences and self-efficacy beliefs. After respondents were asked to provide information on their intention to quit smoking, sociodemographic and medical status, their smoking behaviour and need for autonomy, they were invited to provide information on their attitudes towards smoking cessation. Then, respondents received tailored advice on the basis of their answers. Next, questions about social influence, and self-efficacy perceptions were asked which was followed by another piece of tailored advice. Subsequently, participants were invited to choose a quit smoking date within the next two weeks. Then, respondents could choose in which situations they expected difficulties to refrain from smoking and also whether they wanted to formulate coping plans (to restrain from smoking) in those difficult situations, after which they received an overview of their self-formulated plans – in case they decided to made any. When the questionnaire was completed, all advice was combined into one overall smoking cessation advice, which could be saved, printed and emailed to the participant.
Recruitment and procedure
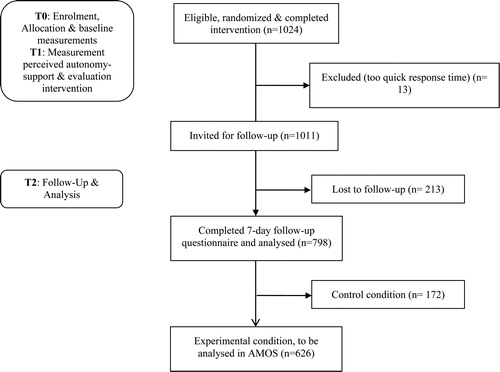
The study was approved by the Institutional Review Board (reference number 2017-PC-7599) and is registered with the Dutch Trial Register (NL6512/NTR-6700). As illustrated in , we recruited 1024 participants using an ISO-certificated online research panel, called PanelClix, from the end of February to mid-April 2018. Prior to their enrolment in the study, participants were provided with information about the study and were asked to provide their online informed consent. Then (T0), participants were automatically and at-random assigned to one of the five conditions by a computer software randomization device. Seven days after participants completed the baseline questionnaire, intervention, and intervention evaluation (T1), they were prompted via email by the same online research panel to fill out a brief follow-up questionnaire (T2). A total of 1011 participants was eligible for the seven-day follow-up, as 13 participants had to be excluded due to too short response time at the baseline measurement. Subsequently, 213 participants were lost-to follow-up, which lead to a final sample size of 798 participants including the control condition (n = 172), leaving 626 participants for statistical analysis. Participants’ approximately 25-minute participation was rewarded by PanelClix with 200 Clix, which equals circa 2.50 euro.
Figure 2. Flow chart of participant progress.
Inclusion and exclusion criteria
Participants eligible to participate in the study were 18 years or older, intended to quit smoking within the following six months, had access to the Internet, and provided online informed consent. In addition, participants had to have smoked during the last seven days and be sufficiently proficient in the Dutch language to complete the questionnaires and read the advice provided as part of the intervention.
Pilot
Two pilot studies were conducted. First, a sample of five smoking cessation feedback messages was pilot-tested among undergraduate communication science students (N = 18) from the local university. The objective of this first pilot study was to examine whether participants were able to distinguish the autonomy-supportive from the controlling feedback messages, as rewritten based on the original intervention. Similarly as in the study by Miller et al. (Citation2007), students received a definition of autonomy-supportive and controlling language style and subsequently were asked to rate each feedback message as follows: ‘To what extent did you perceive the advice as autonomy-supportive or controlling?’ on a five-point Likert scale from 1 (‘strongly autonomy-supportive’) to 5 (‘strongly controlling’). Students were also able to leave any comments they wanted to make regarding these messages. Students who received autonomy-supportive messages also scored lower on the response scale (M = 2.46, SD = 0.62, p < 0.001) than students who received controlling messages (M = 3.68, SD = 0.32). As students were well able to distinguish the autonomy-supportive from the controlling smoking cessation messages,Footnote1 we considered our language manipulation as successful and continued to manipulate the original intervention’s feedback messages based on those five examples.
In a second pilot test, the five versions of the online intervention and assessment of our outcome measures were pilot tested among smokers from different socio-demographic backgrounds (N = 11) and experts from the fields of smoking cessation, internet interventions, and health communication (N = 5). Every version of the intervention was tested by one expert and at least two smokers. This second pilot study aimed to investigate the face validity of the instructions and questionnaire items (questions and response categories) as well as the lay-out and length of the intervention, in order to avoid falsified answers, misinterpretations, and missing responses by respondents. Also, we wanted to test whether the stimulus material was perceived as intended (i.e. whether the language and choice manipulation were clear and distinguishable). Pilot-test participants wished for more instructions in the questions in the intervention, so we added brief explanations to some questions to better guide participants through the intervention. Moreover, most pilot-test participants perceived the introduction of the intervention as too long. Therefore, the research team decided to shorten the introduction to solely consist of a brief welcome, followed by participant information, and brief instructions on how to fill in the questionnaire. In addition, most participants had difficulties understanding the measure for need for autonomy, as well as the manipulation measurement. Thus, we adapted the need for autonomy and manipulation measurements to make them better understandable (i.e. took out double negatives). The majority of participants perceived the experimental stimuli as intended, thus no adaptions were made in message frames.
Experimental stimuli
In four conditions, the message frame of the intervention was manipulated while keeping the content of the smoking cessation advice similar. In the control condition, the message frame was not manipulated (i.e. stayed neutral as in the original smoking cessation intervention) and no content-tailoring was used.
Language
In the autonomy-supportive condition, all smoking cessation advice was manipulated by encouraging respondents to accept more responsibility for their own behaviour, by taking the message recipient’s perspective into account through reflective feedback, and by using language which minimised pressure (Deci et al., Citation1994; Markland et al., Citation2005; Resnicow et al., Citation2008, Citation2014; Williams et al., Citation1999). In the controlling language condition, smoking cessation messages were manipulated by using directive and forceful sentences with imperatives and commands. Furthermore, controlling messages often stated the message source to be perceived as more authoritative and positive filling terms were avoided where possible. For an example of the smoking cessation advice in autonomy-supportive and controlling language, see . To assess the validity of our language manipulation, we used three items asking to which degree respondents perceived the tone of the advice as controlling or autonomy-supportive, e.g. “The advice was formulated in a pressuring tone” (1 = ‘strongly disagree’; 5 = ‘strongly agree’) and a lower value indicates a perception of choice. The three items could not form a reliable scale.
Table 1. Example of smoking cessation advice.
Choice
We operationalized the provision of choice as offering participants to choose for themselves whether they would like to receive additional information on smoking cessation seven times throughout the online assessment by responding to the question ‘Would you like to receive more tips about this topic?’ with ‘yes’ or ‘no’. Respondents could also choose to plan their own quit date or to receive a quit date from the programme. Further, participants in the choice condition could choose whether and for which of nine potentially difficult situations they wanted to formulate coping plans, i.e. plans to cope with these situations in case they would occur (Smit et al., Citation2010; Citation2014). These plans were expected to be personally relevant and helpful for participants in their smoking cessation attempt, as they were tailored to situations that were earlier indicated by participants as to be potentially difficult. In the no choice condition, participants were not asked whether they wanted to see additional information, or whether they wanted to plan a quit date, but received additional smoking cessation information tailored to their earlier responses and a random quit date within the next two weeks. Furthermore, participants in the no choice condition were instructed to formulate coping plans for all nine situations that were presented by the intervention as situations in which it could be difficult to refrain from smoking. Three items examined the validity of our choice manipulation, by assessing whether respondents perceived a feeling of choice throughout the intervention, e.g. ‘In this programme, I could choose a quit smoking date myself’ (1 = ‘strongly disagree’; 5 = ‘strongly agree’) and a higher value indicates controlling language use. For the three choice manipulation items, a reliable scale could be formed (Cronbach’s α= .83, M = 3.39, SD = 0.33). Respondents in the no content-tailored control condition were not offered any opportunity to receive or choose a quit smoking date or to make coping plans for smoking cessation, since formulating – and reading this plan as part of the tailored feedback – could be perceived as content-tailoring.
Measures
Background variables
At baseline (T0), demographic variables were measured: age, gender (1 = male, 2 = female), living arrangement (1 = with partner, 2 = with partner and child(ren), 3 = with child(ren), 4 = by myself, 5 = other), educational level (1 = low: primary school/basic school, 2 = medium: secondary school/high school degree, 3 = high: high school/college degree/university degree), presence of respiratory or cardiovascular diseases (1 = no, 2 = yes). In case of female gender, we also assessed current pregnancy (1 = no, 2 = yes).
Outcome
Seven days post-intervention (T2) respondents’ intention to quit smoking was measured based on the TPB, by measuring the respondent’s intention, desire, and self-prediction to quit smoking (Armitage & Conner, Citation2001; Francis et al., Citation2004). Answers were given on a seven-point Likert scale from 1 (‘strongly disagree’) to 7 (‘strongly agree’) where a higher value indicates a higher intention to quit smoking. The scale had good reliability (Cronbach’s α= .91, M = 4,75, SD = 0.14).
Mediators
Post-intervention (T1), perceived autonomy-support was measured with the Virtual Climate Care Questionnaire, which consists of 15 items that can be answered on a seven-point Likert scale 1 (‘strongly agree’) to 5 (‘strongly disagree’) and a lower value indicates low perceived autonomy-support (VCCQ; Smit et al., Citation2017). The VCCQ scale had good reliability (Cronbach’s α = .97, M = 3.46, SD = 0.15).
After seven days (T2), self-determined motivation to quit smoking was measured with the Treatment Self-Regulation Questionnaire (TSRQ; Levesque et al., Citation2007). The TSRQ has been validated for smoking cessation and was translated from English to Dutch. The TSRQ assesses the degree of self-determined motivation people hold with regards to their engagement in a health behaviour and was answered on a seven-point Likert scale ranging from 1 (‘not true at all’) to 7 (‘very true’) where high values indicate autonomous motivation. The TSRQ sub-scales had good reliability (Cronbach’s α self-determined= .89, M = 3.87, SD = 0.15).
Also at T2, the concepts of attitude, social influence, self-efficacy, and intention to quit smoking were assessed. Eleven items derived from the I-Change model measured attitude towards smoking cessation on three dimensions (i.e. disadvantages of smoking cessation, physical and cognitive advantages of smoking cessation) and were answered on a five-point Likert scale ranging from 1 (‘no, does not’) to 5 (‘yes, does a lot’) with higher items indicating a positive attitude towards smoking cessation (and a negative attitude towards smoking cessation for items measuring disadvantages of smoking cessation, respectively). All sub-scales appeared to have acceptable reliability (Cronbach’s α disadvantages= .76, M = 2.27, SD = 0.59; Cronbach’s α physical= .77, M = 4.05, SD = 0; Cronbach’s α cognitive= .74, M = 3.25, SD = 0.48).
Social influence was assessed based on the I-Change Model, measuring the concepts of social support (three items) and social norms (three items), which take into account a respondent’s partner, children, and family and were formulated as statements to which respondents could answer within five response categories ranging from 1 (no support to quit smoking) to 5 (a lot of support to quit smoking) (de Vries et al., Citation2003; Smit et al., Citation2012). We recoded the social support scale, as we considered respondents who answered ‘9 = not applicable’ as people who did not receive social support (Hoving et al., Citation2006). The sub-scales for social support and social norms had acceptable to good reliability (Cronbach’s αsocial norms= .71, M = 2.19, SD = .05; Cronbach’s αsocial support= .57, M = 3.20, SD = .08).
Self-efficacy was measured according to the I-Change Model by nine items, which were answered on a five-point Likert scale from 1 (‘strongly disagree’) to 5 (‘strongly agree’) and people with a lower value having a low self-efficacy perception. The scale had good reliability with Cronbach’s alpha = .90 (M = 3.27, SD = .18). The scale measured respondents’ stress-, routine-, and skill perceptions to refrain from smoking (e.g. ‘Do you think you can refrain from smoking after dinner?’).
Moderator
At T0, need for autonomy was measured with the Health Causality Orientations Scale (HCOS). The HCOS is a novel scale, which is based on the General Causality Orientations Scale (Deci & Ryan, Citation1985b). Responses were given on a five-point Likert scale from 1 (‘very unlikely’) to 5 (‘very likely’) and participants scoring high on the response scale having a higher need for autonomy. Participants received four different vignettes for which they had to indicate the likelihood of responding in three different ways (each reflecting a different type of orientation, i.e. self-determined, and controlled orientation towards experts, and towards family and friends). For instance, one of the vignettes read ‘Imagine you would have to get motivated to quit smoking. How likely would it be that you would: (A) motivate yourself (self-determined orientation), (B) ask an expert to motivate you (controlled orientation experts), (C) ask family and friends to motivate you (controlled orientation family and friends)’. Mean scores of the four responses reflecting a self-determined orientation resulted in a reliable scale (Cronbach’s α= .76, M = 3.95, SD = 0.13)Footnote2.
Full descriptions of scales including item-wording and factor loadings are provided in the supplemental material.
Statistical analysis
First, descriptive analyses were conducted to determine sample characteristics. Second, two-sided t-tests and chi-square tests and analysis of variance (ANOVA) were conducted where appropriate to check for differences in background variables and smoking related behaviours between the intervention and control groups. Also, ANOVAs were conducted to assess differences between our conditions on perceived autonomy-support, to assess whether our manipulation worked as intended. In addition, we conducted a non-response analysis to determine whether selective dropout had occurred by comparing those who completed the questionnaire at T2 with those lost to follow-up at T2 with regard to the same set of variables, with two-sided t-tests and chi-square tests. These analyses were all done using the statistical computer software program IBM SPSS version 25.
The full hypothesized model was tested with Structural Equation Modelling (SEM) in IBM AMOS version 25. SEM is better suited to conduct moderated mediation analysis of more complex regression models compared to conventional multiple regression, as SEM tests the overall goodness-of-fit of the theoretical model, which moderated mediation analysis using multiple regression (e.g. in SPSS) is unable to do. Also, SEM captures changes and additional relationships in the model that may emerge between variables (Kline, Citation2011). Multiple linear regression would be more difficult to regress multiple mediating and moderating variables simultaneously, as hypothesised in our model. Another benefit of SEM is that it combines a structural model with a measurement model, which subsequently reduces measurement error (i.e. systematic and random), as it is not assumed that scales perfectly measure underlying concepts.
Of our final sample (N = 798), only participants in the experimental conditions (N = 626) were considered for SEM analysis, excluding control condition participants (N = 172) for this particular analysis. Based on this sample of 626 respondents, we conducted a post-hoc power analysis with the G-power software (Faul et al., Citation2009), which indicated that the conducted analysis with the given sample size and alpha error probability (i.e. 1 − β = .05) had a power of .94 to uncover small effect sizes (f2 =0.02). We proceeded as follows. Firstly, we assessed the measurement of our theoretical constructs using confirmatory factor analysis. Then, interaction terms were created to test a moderation of the need for autonomy on the effect of choice and language, and their combination, on perceived autonomy-support. As we used latent variables for the analysis, matched-pair products were created, according to Marsh et al. (Citation2004). With this method, information from the same indicator is not repeated (Kline, Citation2011). This was done for clarity reasons, as creating latent interaction terms with all possible combinations of the indicators would have made the model too complex. Next, interaction terms were stepwise added to the measurement model. We added error covariances between moderator-items and their interaction terms. This was expected, as those items were constructed by multiplication with each other and had high correlations (≥ .8). Also, error-covariances were added among items measuring social norms, as those items measured similar concepts. After establishing model fit with the measurement model, we built the structural regression model based on our hypotheses with direct paths from the exogenous variables (i.e. language, choice, their combination and the need for autonomy) to perceived autonomy-support (H1a,b,c, H3a,b,c) (). Also, we added direct and indirect paths from all exogenous variables to self-determined motivation (H2a,b,c,d) (). Furthermore, we added direct and indirect paths from self-determined motivation, attitudes, social influence, and self-efficacy to the intention to refrain from smoking (H4) ().
Figure 3. Hypothesized structural model with significant paths.
Note. Results are presented as standardized total effects. For clarity, items of latent variables (ellipse) are not presented. Observed variables are presented as rectangles. Cog = cognitive advantages of smoking cessation. Phy = physical advantages of smoking cessation. Con = disadvantages of smoking cessation. Dotted lines represent non-significant paths. Straight lines represent significant paths (p < .05).
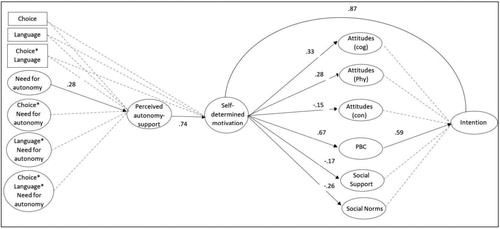
As our hypothesised structural regression model is nested under the earlier predicted measurement model, we compared this model to the measurement model with a chi-square comparison test.Footnote3 Succeeding to establish sufficient model fit for our hypothesised model, we interpreted the model structure. As our model is very complex, for clarity reasons we present the results only for the significant regression weights. The correlation matrix, question wording, and factor loadings are in the online supplement. The significance level was set at 5% and we report total unstandardized effects.
Results
Sample characteristics and non-response analysis
Sample descriptives can be found in .
Table 2. Comparison of participants who completed the study with those who dropped out.
Comparisons of the 798 participants who completed the study and the 213 participants who were lost-to-follow-up after seven days showed no significant differences in demographics, such as gender, age, educational level. However, people who did not complete the follow-up measurement were significantly more often living alone (036), had lower perceptions of perceived autonomy-support (t = −3.14, df = 1009, p = .002), and had more positive attitudes towards smoking cessation (t = −2.20, df = 1009, p = .028). The analysis did not reveal significant differences in smoking related behaviours, such as number of cigarettes smoked per day or past quit attempts (). Attrition after seven days was unrelated to experimental condition.
Randomization
Comparisons of participants’ demographics, such as age and educational level, as well as their smoking behaviour did not show significant differences between the experimental conditions, expect from one item assessing addiction level. Thus, we deemed the randomization successful. Of the 798 people who completed the follow-up measurement, n = 167 (20.9%) participants were randomized into the autonomy-supportive language & choice condition, n = 160 (20.1%) participants into the autonomy-supportive language & no-choice condition, n = 147 (18.4%) participants into the controlling language & choice condition, n = 152 (19.0%) participants into the controlling language & no-choice condition, and n = 172 (21.6%) participants were randomized into the control condition.
Manipulation assessment
As expected, participants in the choice conditions perceived more choice (M = 3.71, SD = .97) than participants in the no choice condition (M = 2.98, SD = .88), F(1) = 125,345, p < .005 as higher values indicate a perception of choice. Three items testing whether the tone of our messages was perceived as intended were analysed separately. Only two language manipulation items showed significant differences between participants who received smoking cessation advice in autonomy-supportive language (M = 2.85, SD = 1.08; M = 2.35, SD = 1.00) compared to controlling language (M = 3.12, SD = 1.07; M = 2.53, SD = 1.13), F(1) = 12,706, p= .000 and F(1) = 5,421, p= .020 respectively, while lower mean scores indicate autonomy-support. One item, namely ‘I feel understood by the smoking cessation advice’ did not show significant differences among the autonomy-supportive and the controlling language condition (autonomy-supportive language condition: M = 3.48; SD = 1.01 compared to controlling language condition: M = 3.51; SD = .95).
Normality
We evaluated the assumptions of multivariate normality and linearity, and observed several outliers among endogenous variables (i.e. perceived autonomy-support, self-determined motivation, social norms, negative and positive attitudes towards smoking cessation). All outliers were checked, considered random and therefore not removed. There was no missing data among the endogenous variables and we choose to use maximum likelihood parameter estimation with 200 bootstrap samples with the bootstrap factor set at 2, as one item from social influence was non-normally distributed (Kurtosis =3.93; Skewness =2.06). No multicolinearity existed.
Confirmatory factor analysis to establish the measurement model
We conducted a CFA with all factors relating to our theoretical model (i.e. autonomy-supportive language, offering choice, their combination, need for autonomy, perceived autonomy-support, self-determined motivation, attitude, social influence, self-efficacy, and intention). Our default measurement model appeared to have a poor model fit according to conventional goodness-of-fit indices (Byrne, Citation2016): χ2 df= 1461 (3810,711), p <.000,Footnote4 CMIN/DF = 2,608, Comparative Fit Index (CFI) = .89; Root Mean Square Error of Approximation (RMSEA) = .051, 90% confidence interval (CI) [.049, .053]. The modification indices suggested several error correlations: one between items of perceived autonomy-support, one between items measuring self-determined motivation, one between items measuring social influence, and three between items measuring self-efficacy. Stepwise adding those six error-covariances led to significantly better model fit. provides an overview of model fit indices without and with interactions. Standardized factor loadings (see ) were all near to or above .70 showing good convergent validity, except for four items measuring attitudes towards smoking cessation, two items measuring social support and one item from social norms, two items measuring self-efficacy, one item assessing self-determined motivation, and two items from need for autonomy which loaded with lower values (range: 0.22 and 0.64) on scales. As those items also had lower residual covariances, we assumed random measurement error.
Table 3. Fit indices of the measurement model.
Model testing
Our hypothesized model without the interaction terms of the moderator had good fit with the data χ2 df= 1507 (3562,635), p = .000, CMIN/DF = 2,364, CFI=.91, and RMSEA of .047, 90% CI [.045, .049]. When adding the 3-way interaction of the need for autonomy and the experimental conditions, the structural model still had good fit with the data χ2 df= 2203 (4539,979), p = .000, CMIN/DF = 2,061, CFI=.95, and RMSEA of .041, 90% CI [.039, .043]. The results from SEM analysis are depicted in the structural model in .
Hypothesis testing
Effects of autonomy-supportive message frames on perceived autonomy-support and self- determined motivation
In hypothesis 1, we expected a positive effect from autonomy-supportive language use (H1a), the provision of choice (H1b), and their combination (H1c) on perceived autonomy-support. Neither the use of autonomy-supportive language, the provision of choice, nor their combination had a significant effect on perceived autonomy-support. Subsequently, we reject hypothesis 1. Next, in our second hypothesis, we assumed that the use of autonomy-supportive language (H2a) and the provision of choice (H2b), as well as their combination (H2c), would lead to higher levels of self-determined motivation and that those effects were mediated via perceived autonomy-support (H2d). There was no significant effect of autonomy-supportive language, the provision of choice, or their combination on self-determined motivation to quit smoking. Also, perceived autonomy-support did not significantly mediate the effects of autonomy-supportive language and the provision of choice on self-determined motivation. Thus, we also reject hypothesis 2. Mean values of perceived autonomy-support, which were rather on the higher end of the scale are provided in .
Table 4. Means of perceived autonomy-support and need for autonomy per experimental condition (n = 626).Table Footnotea
Moderation of the need for autonomy
We expected that people with a high need for autonomy would perceive higher levels of autonomy-support when receiving smoking advice in autonomy-supportive language (H3a) and when being offered with choice (H3b), and even more so with their combination (H3c), than people with a low need for autonomy. Results from the structural model with interaction terms showed no significant moderation of respondents’ need for autonomy on effects of autonomy-supportive language use, the provision of choice, nor their combination on perceived autonomy-support. Yet, the need for autonomy had a positive direct effect on perceived autonomy-support (b = .31, p = .005). Hypothesis 3 is rejected. Also, as depicted in , smokers’ need for autonomy was rather high.
Effects from self-determined motivation to quit smoking on intention to quit
In hypothesis 4, we expected that self-determined motivation led to intention to quit smoking via self-efficacy, attitudes, and social influence. With our structural model, we could confirm a significant positive effect from self-determined motivation on intention to quit smoking (b = .86, p = .000), which was mediated by negative attitudes towards smoking cessation, subjective norms and self-efficacy. Moreover, self-efficacy had a weak positive direct effect on intention (b = .13, p = .002), whereas negative attitudes towards smoking cessation had a negative direct relationship with intention to quit smoking (bnegative attitudes = −.29, p = .000) and receiving social support for smoking cessation enhanced intention to quit (bsocial suppor t= .09, p = .012). Thus, we confirm hypothesis 4. An overview of the direct and indirect effects is provided in appendix II.
Discussion
The aim of the present study was to test the effectiveness of autonomy-supportive message frames in online communication about smoking cessation by means of testing the effects of the use of autonomy-supportive language and the provision of a choice on perceived autonomy-support. Also, we sought to test whether the individual need for autonomy interacted with the message frame used, in such a way that individuals with a higher need for autonomy would benefit more from autonomy-supportive message framing. Next, we tested whether autonomy-supportive message frames could lead to enhanced self-determined motivation to quit, and if this eventually led to the formation of a stronger intention to quit smoking. To the best of our knowledge, this was the first study testing effects of autonomy-supportive message frames in the context of an online health communication intervention aimed at smoking cessation.
Effects of the use of autonomy-supportive language, the provision of choice, and the need for autonomy on perceived autonomy-support and self-determined motivation
Contrary to our expectations, we did not find any significant effects of autonomy-supportive language, the provision of choice, or their combination on people’s perceived autonomy-support. Also, we had to reject our hypothesis that the use of autonomy-supportive language and the provision of choice would lead to more self-determined motivation to quit smoking. Notable, however, is that the average level of perceived autonomy-support was rather high across all conditions, even in the control condition. Since smokers across all conditions – even in the neutrally formulated and non-tailored control condition – reported high levels of perceived autonomy-support, it could be that the internet environment itself is perceived as an autonomy-supportive context. People looking for online health communication interventions are able to do so whenever the time and location is convenient for them. Regardless of the type of message frame used, the internet environment could have led to such a feeling of freedom and choice, that variations in message frame no longer mattered. No literature was found to confirm this assumption. Moreover, participants’ positive motivation to quit smoking, which was an inclusion criterion for this study, could possibly explain these findings. That is, participants who already wished to quit smoking before their enrolment in the study might not have perceived a pressure to stop (i.e. lower perceived autonomy-support) when receiving smoking cessation tips in controlling language or when not being provided with choice, in potential contrast with participants not yet motivated to quit. Smokers not (yet) motivated to quit smoking could have felt more pressure to quit and still have negative attitudes towards smoking cessation, which in turn could have diminished their perceived autonomy-support. Also, given study participant’s positive motivation to quit, these participants could have already formed a positive opinion about smoking cessation. Thus, controlling wording, such as ‘must quit’ could not have diminished their perceived levels of autonomy-support. Our finding contradicts results from previous studies conducted in offline and face-to-face settings. For example, Williams and colleagues (2002) found that an autonomy-supportive interpersonal communication style (e.g. emphasizing the smoker’s own choice to quit and seeing smoking cessation from the smoker’s perspective) in a brief smoking cessation counselling session enhanced smokers’ self-determined motivation. A potential reason that we were not able to replicate Williams and colleagues’ findings could be rooted in the different environments, namely, face-to-face (offline) versus online setting. A teacher or physician talking to someone in person could be perceived more autonomy-supportive due to non-verbal cues as body language, tone of voice, or mimics, than an online feedback letter.
In this line of thought, non-verbal cues of message frames might be better expressed in combination with written words as represented in our message frames only, or with other stimuli such as in illustrations, animations and/or auditory messages. For instance, studies that investigated the presentation of eHealth information in relation to recall of this health information (Bol et al., Citation2015; Meppelink et al., Citation2015), showed that health information is recalled better among participants when it is presented audio-visually, thus a combination of spoken text and a related animation or illustration as compared to text-only health information. Therefore, we recommend future research to test whether the addition of visuals, illustrations or auditory messages, alone or combined with autonomy-supportive vs. controlling text message frames might lead to enhanced message frame effects. A control condition should be used in such studies, to check for confounding effects.
Politeness Theory (Jenkins & Dragojevic, Citation2013) provides an alternative explanation for why people perceived high levels of autonomy-support, also in our controlling language condition. According to this theory, controlling language does not necessarily have to be perceived as impolite or demeaning - thus lowering the message recipient’s level of perceived autonomy or freedom and subsequently leading to reactance arousal - when the controlling message is formulated in a polite way and emphasizes the message recipient’s freedom to choose (i.e. in our controlling language & choice condition). An additional explanation for the high levels of perceived autonomy-support in this study, could be that smokers across all experimental conditions were asked (or forced, in the controlling language conditions conditions) to formulate coping plans for potentially difficult situations. Subsequently, the formulation of coping plans could have been perceived as receiving freedom and being able to incorporate own ideas about smoking cessation. This is illustrated by responses to our open-ended think aloud measure like ‘feeling like I am creating my own advice’.
The need for autonomy as a moderator
Next, we were not able to confirm Resnicow and colleagues' (2008, 2014) finding that smokers’ need for autonomy moderates the effects of message framing. This might be explained by our finding that, in the present study, on average, smokers had a high need for autonomy. Congruent with previous research on SDT, study participants’ high need for autonomy might provide an explanation for not finding any significant effects of autonomy-supportive message frames on perceived autonomy-support, as those people are more prone to perceive higher levels of autonomy-support (Deci & Ryan, Citation1987). In more detail, people with an autonomous orientation feel more volitional in their actions when the behaviour of question is congruent with their own values and goals. As participants needed to be motivated to quit to be eligible for the study, this could have caused their high feelings of autonomy-support. Therefore, future studies investigating autonomy-supporting message frame effects should sample more heterogenic participants with regards to their need for autonomy, by means of a real-life trial instead of panel research.
Effects from self-determined motivation on intention
Self-determined motivation predicted intention to quit smoking which was positively mediated by a smoker’s self-efficacy perception, and negatively mediated by people’s negative attitudes towards smoking cessation and social norms about smoking cessation. This finding confirms earlier research on SDT and the integration of the motivational sequence in the TPB (Hagger & Chatzisarantis, Citation2009). Also, self-determined motivation to quit was negatively related to a person’s social norms about quitting. This finding seems logical, as social norms and social pressures can be considered controlling beliefs – thus the opposite of self-determined beliefs and self-determined motivation to quit (Joseph et al., Citation2016). Next, self-determined motivation was negatively related to the negative attitudes towards smoking cessation, which also seems logical, as being intrinsically motivated to quit aligns with perceiving less disadvantages of smoking cessation. For instance, in Cognitive Dissonance theory (Harmon-Jones & Mills, Citation2019) it is stated that a person with non-congruent thoughts (such as simultaneously believing that quitting fits one’s values and that it makes one unhappy), would try to eliminate the non-congruent thought to reach well-being. Thus, a smoker with a high level of self-determined motivation would likely change negative attitudes towards smoking cessation into positive ones to reduce cognitive dissonance – and vice versa. To support this line of argumentation, we found that self-determined motivation to quit enhanced self-efficacy, which also enhanced intention to quit smoking. Therefore, we could assume that as a person’s trusts in own efficacy to quit smoking increases, negative attitudes decrease, too. This line of reasoning is supported by results from a secondary analysis, in which we found a negative direct effect from self-efficacy on negative attitudes (b= −.13, p = .000) in line with previous research (e.g. Smit et al., Citation2014).
Limitations
A limitation of the current study is that for the measurement of the need for autonomy, we had to use a novel, not yet validated scale, the HCOS. However, the scale that was used as a basis for the development of the HCOS – the General Causality Orientations Scale – previously proved both valid and reliable (Deci & Ryan, Citation1985b). Moreover, the HCOS showed to have good reliability in our study. In addition, we preferred to use the HCOS, because this scale was adapted specifically to a health context. Given its theoretical basis, reliance on the both valid and reliable GCOS and good reliability in the present study as well as in a previous study by (Smit & Bol, Citation2019), we highly recommend future research efforts to use, but especially validate, the HCOS.
Moreover, as the present study was an online experiment for which participants from an online panel were recruited, results might have a low ecological validity because participants might have been more used to online assessments, which could have potentially biased the results. As a result of their research experience, participants could for example have spent less time processing our stimulus material, might have clicked faster through the intervention, or could have on purpose responded in ways that they had lower chances to drop out from participation. Before drawing the conclusion that message framing has no effects, this study might need to be replicated in a more real-life setting with smokers actually searching for a smoking cessation intervention (e.g. via a search engine), having a strong intention to quit and being more likely to read and process our message manipulations more attentively.
In addition, in accordance with evidence from theories like the theory of planned behaviour, intention to quit smoking (in the near future) was used as the main outcome and as a proxy measure for actual quit smoking behaviour. This might limit our results, as we were consequently unable to observe whether smokers indeed translated their positive intention to quit in actual smoking cessation (attempts). As we would ultimately want to know whether autonomy-supportive message frames could effectively lead to increased smoking abstinence rates, we recommend future research to also consider actual quit smoking behaviour as an outcome.
Since this study was one of the first to test the effect of message framing an autonomy-supportive way on perceived autonomy-support, motivation, and socio-cognitive factors for behaviour change, we acknowledge that based on the health communication literature different ways of message framing seem to potentially increase intervention effectiveness. For instance, as proposed by Rothman et al. (Citation2006), framing messages based on the regulatory focus could be more effective in changing health behaviour.
Conclusion
The results of this study suggest that autonomy-supportive message frames did not significantly induce higher levels of perceived autonomy-support and self-determined motivation to quit than controlling message frames. Also, the need for autonomy did not moderate the effect of autonomy-supportive message frames on perceived autonomy-support. On average, participating smokers reported a high need for autonomy and also perceived high levels of autonomy-support, regardless of the condition they were randomized into. This could be due to their positive motivation to quit smoking and likely positive opinion towards smoking cessation. As expected, self-determined motivation had a positive effect on intention to quit smoking, which was moderated by smokers’ self-efficacy, attitudes and subjective norms about smoking cessation. To our knowledge, our study is the first that aimed to test the effect of autonomy-supportive message framing on people’s perceived autonomy-support while considering the individual need for autonomy as a moderator; and whether autonomy-supportive message frames – through increased perceived autonomy-support - lead to more self-determined motivation, and an increased intention to quit smoking. Therefore, one should be cautious in drawing the conclusion that online computer-tailored autonomy-supportive smoking cessation advice is not effective in inducing perceived autonomy-support and self-determined motivation. To draw more definite conclusions, future studies first need to test the hypotheses within more heterogenic samples of participants with regards to their need for autonomy, such as by means of a real life randomized controlled trial.
Supplemental Material
Download MS Word (14.5 KB)Acknowledgements
The authors would like to thank Inge van Strien-Knippenberg for her valuable support in the preparations of the data collection.
Disclosure statement
None to declare.
Data availability statement
The data that support the findings of this study are available from the corresponding author, MA, upon reasonable request.
Additional information
Funding
Notes
1 As the sample size consisted of 18 participants, we decided not to provide t-test results in the text.
2 We also measured controlled orientation with eight items from the HCOS, which are for conciseness reasons not further described above. Items that reflected a controlled orientation combined into in scales with good reliability both for experts (Cronbach’s α= .86, M = 2.69, SD = 1.05) and for family and friends (α= .89, M = 2.63, SD = 1.04), and correlations of controlled items with autonomous items were – as expected – in a different direction than self-determined items.
3 We acknowledge that there might be existing equivalent models, however, we argue that those models would not be plausible according to SDT and theories of planned behaviour. Also, our theoretical model has been previously tested and proven to be valid. For a meta-analysis, see Hagger and Chatzisarantis (Citation2009). Furthermore, we conducted an experiment and therefore adaptions of causal paths from the experimental conditions were not possible. Thus, we did not compare our measurement model to equivalent models.
4 As our sample size exceeds 400 cases, the chi-square was expected to be statistically significant (http://davidakenny.net/cm/fit.htm).
5 Only respondents who were considered for analysis without respondents randomized into the control condition.
References
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. https://doi.org/10.1016/0749-5978(91)90020-T
- Armitage, C. J., & Conner, M. (2001). Efficacy of the theory of planned behaviour: A meta-analytic review. The British Journal of Social Psychology, 40(Pt 4), 471–499. https://doi.org/10.1348/014466601164939
- Bergh, C. M. M. R., Den Harteloh, P. P. M., & Croes, E. (2017). Doodsoorzaak nr. 1 bij jonge Nederlanders: de sigaret. Nederlands Tijdschrift Voor Geneeskunde, 161(1). https://www.ntvg.nl/artikelen/doodsoorzaak-nr-1-bij-jonge-nederlanders-de-sigaret/volledig], retrieved July 2020.
- Bol, N., van Weert, J. C., de Haes, H. C., Loos, E. F., & Smets, E. M. (2015). The effect of modality and narration style on recall of online health information: Results from a Web-based experiment. Journal of Medical Internet Research, 17(4), e104. Published 2015 Apr 24. https://doi.org/doi: https://doi.org/10.2196/jmir.4164
- Byrne, B. M. (2016). Structural equation modeling with AMOS. Routledge. https://doi.org/10.4324/9781315757421
- De Vries, H., & Brug, J. (1999). Computer-tailored interventions motivating people to adopt health promoting behaviours: Introduction to a new approach. Patient Education and Counseling, 36(2), 99–105. https://doi.org/10.1016/s0738-3991(98)00127-x
- de Vries, H., Mudde, A., Leijs, I., Charlton, A., Vartiainen, E., Buijs, G., Clemente, M. P., Storm, H., González Navarro, A., Nebot, M., Prins, T., & Kremers, S. (2003). The European Smoking prevention Framework Approach (EFSA): An example of integral prevention. Health Education Research, 18(5), 611–626. https://doi.org/10.1093/her/cyg031
- Deci, E. L., Eghrari, H., Patrick, B. C., & Leone, D. R. (1994). Facilitating internalization: The self-determination theory perspective. Journal of Personality, 62(1), 119–142. https://doi.org/10.1111/j.1467-6494.1994.tb00797.x
- Deci, E. L., & Ryan, R. M. (1985a). Intrinsic motivation and self-determination in human behavior (Perspectives in social psychology). Plenum.
- Deci, E. L., & Ryan, R. M. (1985b). The general causality orientations scale: Self-determination in personality. Journal of Research in Personality, 19(2), 109–106. https://doi.org/10.1016/0092-6566(85)90023-6
- Deci, E. L., & Ryan, R. M. (1987). The support of autonomy and the control of behavior. Journal of Personality and Social Psychology, 53(6), 1024–1037. https://doi.org/10.1037/0022-3514.53.6.1024
- Deci, E. L., & Ryan, R. M. (2000). The " What " and " Why " of goal pursuits: Human needs and the self-determination of behavior. Psychological Inquiry, 11(4), 227–241. https://doi.org/10.1207/S15327965PLI1104_01
- Etter, J.-F., & Perneger, T. V. (2001). Effectiveness of a computer-tailored smoking cessation program. Archives of Internal Medicine, 161(21), 2596–2601. https://doi.org/10.1001/archinte.161.21.2596
- Faul, F., Erdfelder, E., Buchner, A., & Lang, A. G. (2009). Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods. 41(4), 1149–1160.
- Francis, J., Eccles, M. P., Johnston, M., Walker, A. E., Grimshaw, J., Foy, R., & Bonetti, D. (2004). Constructing questionnnaires based on the theory of planned behaviour: A manual for health services researchers. University of Newcastle upon Tyne.
- Gagné, M., & Deci, E. L. (2005). Self-determination theory and work motivation. Journal of Organizational Behavior, 26(4), 331–362. https://doi.org/10.1002/job.322
- Hagger, M. S., & Chatzisarantis, N. L. D. (2009). Integrating the theory of planned behaviour and self-determination theory in health behaviour: A meta-analysis. British Journal of Health Psychology, 14(Pt 2), 275–302. https://doi.org/10.1348/135910708X373959
- Hagger, M. S., & Chatzisarantis, N. L. D. (2011). Causality orientations moderate the undermining effect of rewards on intrinsic motivation. Journal of Experimental Social Psychology, 47(2), 485–489. https://doi.org/10.1016/j.jesp.2010.10.010
- Harmon-Jones, E., & Mills, J. (2019). An introduction to cognitive dissonance theory and an overview of current perspectives on the theory. In Cognitive dissonance: Reexamining a pivotal theory in psychology (2nd ed., pp. 3–24). American Psychological Association. https://doi.org/10.1037/0000135-001
- Hawkins, R. P., Kreuter, M., Resnicow, K., Fishbein, M., & Dijkstra, A. (2008). Understanding tailoring in communicating about health. Health Education Research, 23(3), 454–466. https://doi.org/10.1093/her/cyn004
- Hoving, E. F., Mudde, A. N., & De Vries, H. (2006). Smoking and the Ø pattern; predictors of transitions through the stages of change. Health Education Research, 21(3), 305–314. https://doi.org/10.1093/her/cyl033
- Jenkins, M., & Dragojevic, M. (2013). Explaining the process of resistance to persuasion: A politeness theory-based approach. Communication Research, 40(4), 559–590. https://doi.org/10.1177/0093650211420136
- Joseph, R. P., Daniel, C. L., Thind, H., Benitez, T. J., & Pekmezi, D. (2016). Applying psychological theories to promote long-term maintenance of health behaviors. American Journal of Lifestyle Medicine, 10(6), 356–368. https://doi.org/10.1177/1559827614554594
- Kinnafick, F. E., Thogersen-Ntoumani, C., & Duda, J. L. (2016). The effect of need supportive text messages on motivation and physical activity behaviour. Journal of Behavioral Medicine, 39 (4), 574–586. https://doi.org/10.1007/s10865-016-9722-1
- Kinnafick, F. E., Thogersen-Ntoumani, C., Duda, J. L., & Taylor, I. (2014). Sources of autonomy support, subjective validity and physical activity behaviour associated with participation in a lunchtime walking intervention for physically inactive adults. Psychology of Sport and Exercise, 15(2), 190–197. https://doi.org/10.1016/j.psychsport.2013.10.009
- Kline, R. B. (2011). Principles and practice of structural equation modeling (Todd D. Little, Ed.) (3rd ed.). The Guilford Press.
- Kreuter, M. W., & Wray, R. J. (2003). Tailored and targeted health communication: Strategies for enhancing information relevance. American Journal of Health Behavior, 27(1), 227–232. https://doi.org/10.5993/AJHB.27.1.s3.6
- Legault, L. (2016). The need for autonomy. Encyclopedia of Personality and Individual Differences. https://doi.org/10.1007/978-3-319-28099-8
- Levesque, C. S., Williams, G. C., Elliot, D., Pickering, M. A., Bodenhamer, B., & Finley, P. J. (2007). Validating the theoretical structure of the Treatment Self-Regulation Questionnaire (TSRQ) across three different health behaviors. Health Education Research, 22(5), 691–702. https://doi.org/10.1093/her/cyl148
- Lustria, M. L., Noar, S. M., Cortese, J., Van Stee, S. K., Glueckauf, R. L., & Lee, J. (2013). A meta-analysis of web-delivered tailored health behavior change interventions. Journal of Health Communication, 18(9), 1039–1069. https://doi.org/10.1080/10810730.2013.768727
- Markland, D., Ryan, R. M., Tobin, V. J., & Rollnick, S. (2005). Motivational Interviewing and self-determination theory. Journal of Social and Clinical Psychology, 24(6), 811–831. https://doi.org/10.1521/jscp.2005.24.6.811
- Marsh, H. W., Wen, Z., & Hau, K. T. (2004). Structural equation models of latent interactions: Evaluation of alternative estimation strategies and indicator construction. Psychological Methods, 9(3), 275–300. https://doi.org/10.1037/1082-989X.9.3.275
- Meppelink, C. S., van Weert, J. C., Haven, C. J., & Smit, E. G. (2015). The effectiveness of health animations in audiences with different health literacy levels: An experimental study. Journal of Medical Internet Research, 17(1), e11. https://doi.org/10.2196/jmir.3979
- Miller, C. H., Lane, L. T., Deatrick, L. M., Young, A. M., & Potts, K. A. (2007). Psychological reactance and promotional health messages: The effects of controlling language, lexical concreteness, and the restoration of freedom. Human Communication Research, 33(2), 219–240. https://doi.org/10.1111/j.1468-2958.2007.00297.x
- Moustaka, F. C., Vlachopoulos, S. P., Kabitsis, C., & Theodorakis, Y. (2012). Effects of an autonomy-supportive exercise instructing style on exercise motivation, psychological well-being, and exercise attendance in middle-age women. J Phys Act Health, 9(1), 138–150. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/22232500 https://doi.org/10.1123/jpah.9.1.138
- Ng, J. Y. Y., Ntoumanis, N., Thogersen-Ntoumani, C., Deci, E. L., Ryan, R. M., Duda, J. L., & Thøgersen-Ntoumani, C. (2012). Self-determination theory applied to health contexts: A meta-analysis. Perspectives on Psychological Science: A Journal of the Association for Psychological Science, 7(4), 325–340. https://doi.org/10.1177/1745691612447309
- Noar, S. M., Harrington, N. G., & Aldrich, R. S. (2009). The role of message tailoring in the development of persuasive health communication messages. Annals of the International Communication Association, 33(1), 73–133. https://doi.org/10.1080/23808985.2009.11679085
- Resnicow, K., Davis, R. E., Zhang, G., Konkel, J., Strecher, V. J., Shaikh, A. R., Tolsma, D., Calvi, J., Alexander, G., Anderson, J. P., & Wiese, C. (2008). Tailoring a fruit and vegetable intervention on novel motivational constructs: Results of a randomized study. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine, 35(2), 159–169. https://doi.org/10.1007/s12160-008-9028-9
- Resnicow, K., Zhou, Y., Hawley, S., Jimbo, M., Ruffin, M. T., Davis, R. E., Shires, D., & Lafata, J. E. (2014). Communication preference moderates the effect of a tailored intervention to increase colorectal cancer screening among African Americans. Patient Education and Counseling, 97(3), 370–375. https://doi.org/10.1016/j.pec.2014.08.013
- Rothman, A., Bartels, R., Wlaschin, J., & Salovey, P. (2006). Strategic use of gain-and loss-framed messages to promote healthy behaviour: How thoery can inform practice. Journal of Communication, 56 (suppl_1), S202–S220. https://doi.org/10.1111/j.1460-2466.2006.00290.x
- Ryan, R. M., & Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. The American Psychologist, 55(1), 68–78. https://doi.org/10.1037//0003-066x.55.1.68
- Sheeran, P., & Orbell, S. (2000). Self-schemas and the theory of planned behavior. European Journal of Social Psychology, 30(4), 533–550. (January), https://doi.org/10.1002/1099-0992(200007/08)30:4<533::AID-EJSP6>3.0.CO;2-F
- Sheeran, P., & Webb, T. L. (2016). The intention–behavior gap. Social and Personality Psychology Compass, 10(9), 503–518. https://doi.org/10.1111/spc3.12265
- Smit, E. S., De Vries, H., & Hoving, C. (2012). Effectiveness of a web-based multiple tailored smoking cessation program: A randomized controlled trial among Dutch adult smokers. Journal of Medical Internet Research, 14(3), e82. https://doi.org/10.2196/jmir.1812
- Smit, E. S., Candel, M. J. J. M., Hoving, C., & de Vries, H. (2016). Results of the PAS study: A randomized controlled trial evaluating the effectiveness of a web-based multiple tailored smoking cessation program combined with tailored counseling by practice nurses. Health Communication, 31(9), 1165–1173. https://doi.org/10.1080/10410236.2015.1049727
- Smit, E. S., Dima, A. L., Immerzeel, S. A. M., van den Putte, B., & Williams, G. C. (2017). The virtual care climate questionnaire: Development and validation of a questionnaire measuring perceived support for autonomy in a virtual care setting. Journal of Medical Internet Research, 19(5), e155. https://doi.org/10.2196/jmir.6714
- Smit, E. S., de Vries, H., & Hoving, C. (2010). The PAS study: A randomized controlled trial evaluating the effectiveness of a web-based multiple tailored smoking cessation programme and tailored counselling by practice nurses. Contemporary Clinical Trials, 31(3), 251–258. https://doi.org/10.1016/j.cct.2010.03.001
- Smit, E. S., Linn, A. J., & van Weert, J. C. M. (2015). Taking online computer-tailoring forward. The European Health Psychologist, 17(1), 25–31.
- Smit, E. S., & Bol, N. (2019). From self-reliers to expert-dependents: identifying classes based on health-related need for autonomy and need for external control among mobile users. Media Psychology, 23(3), 391–324. https://doi.org/10.1080/15213269.2019.1604235
- Smit, E. S., Evers, S. M. A. A., de Vries, H., & Hoving, C. (2013). Cost-effectiveness and cost-utility of Internet-based computer tailoring for smoking cessation. Journal of Medical Internet Research, 15(3), e57. https://doi.org/10.2196/jmir.2059
- Smit, E. S., Hoving, C., Schelleman-Offermans, K., West, R., & de Vries, H. (2014). Predictors of successful and unsuccessful quit attempts among smokers motivated to quit. Addictive Behaviors, 39(9), 1318–1324. https://doi.org/10.1016/j.addbeh.2014.04.017
- Su, Y. L., & Reeve, J. (2011). A meta-analysis of the effectiveness of intervention programs designed to support autonomy. Educational Psychology Review, 23(1), 159–188. https://doi.org/10.1007/s10648-010-9142-7
- Taylor, G. M. J., Dalili, M. N., Semwal, M., Civljak, M., Sheikh, A., & Car, J. (2017). Internet-based interventions for smoking cessation. Cochrane Database of Systematic Reviews, (9, September). 129pp. https://doi.org/10.1002/14651858.CD007078.pub5
- Williams, G. C., Cox, E. M., Kouides, R., & Deci, E. L. (1999). Presenting the facts about smoking to adolescents: effects of an autonomy-supportive style. Archives of Pediatrics & Adolescent Medicine, 153(9), 959–964. https://doi.org/10.1001/archpedi.153.9.959
- Williams, G. C., Gagné, M., Ryan, R. M., & Deci, E. L. (2002). Facilitating autonomous motivation for smoking cessation. Health Psychology, 21(1), 40–50. https://doi.org/10.1037//0278-6133.21.1.40
- Williams, G. C., McGregor, H. A., Sharp, D., Levesque, C., Kouides, R. W., Ryan, R. M., & Deci, E. L. (2006). Testing a self-determination theory intervention for motivating tobacco cessation: Supporting autonomy and competence in a clinical trial. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 25(1), 91–101. https://doi.org/10.1037/0278-6133.25.1.91
- World Health Organisation. (2018). Tobacco fact sheet. Fact sheet.